About hernia
hernia types classification anatomy surgical management clinical overview
hernia repair surgery outcomes
Hernia - A Comprehensive Clinical Overview
Definition
Classification
By Reducibility / Clinical State
| State | Description |
|---|---|
| Reducible | Contents can be returned to the cavity spontaneously or manually |
| Irreducible (incarcerated) | Cannot be reduced; does not automatically imply ischaemia |
| Obstructed | Bowel within the sac is obstructed but not yet ischaemic |
| Strangulated | Blood supply to the contents is compromised - a surgical emergency |
The risk of strangulation depends heavily on the size of the hernia neck. Femoral hernias strangulate in up to 40–50% of cases at presentation, while incisional hernias strangulate in only ~2%. Among all patients with small bowel obstruction from hernia, intestinal ischaemia occurs in up to 75% and necrosis in over 25%. - Sleisenger & Fordtran's GI and Liver Disease; Maingot's Abdominal Operations
By Location
External (Abdominal Wall) Hernias
- Inguinal (direct and indirect)
- Femoral
- Umbilical / Paraumbilical
- Epigastric
- Spigelian
- Incisional (ventral)
- Obturator
- Lumbar (Petit's triangle, Grynfeltt-Lesshaft)
- Perineal
- Sciatic
Internal Hernias
- Congenital: paraduodenal, through the foramen of Winslow
- Iatrogenic: after Roux-en-Y gastric bypass (Petersen's defect), colectomy, pancreaticoduodenectomy - Maingot's
Inguinal Hernia (Most Common)
Epidemiology
- Most common hernia overall; ~10:1 male to female predominance
- More frequent on the right side
- A patient with one inguinal hernia has a 50% lifetime risk of developing one on the other side - Bailey & Love
Anatomy of the Inguinal Canal
- Anteriorly: external oblique aponeurosis
- Posteriorly: transversalis fascia (reinforced medially by the conjoint tendon)
- Superiorly: arching fibres of internal oblique and transversus abdominis, forming the conjoint tendon
- Inferiorly: inguinal ligament (rolled-under edge of external oblique)
Types
Indirect (Lateral / Oblique) Inguinal Hernia
- Passes through the deep inguinal ring lateral to the inferior epigastric vessels
- Travels obliquely through the inguinal canal in the path of the processus vaginalis
- Can descend into the scrotum (scrotal hernia)
- Can be congenital (due to a patent processus vaginalis, failure of closure before birth) or acquired
- All paediatric inguinal hernias are indirect by definition
- Higher risk of strangulation than direct hernias due to a narrower neck
Direct (Medial) Inguinal Hernia
- Always acquired - due to weakness in the posterior wall medial to the inferior epigastric vessels
- Protrudes through Hesselbach's triangle (boundaries: inferior epigastric vessels laterally, lateral border of rectus abdominis medially, inguinal ligament inferiorly)
- Broad base - rarely strangulates
- More common in elderly men
- The bladder can be pulled into a direct hernia
Sliding Hernia
- An indirect hernia where a retroperitoneal organ (e.g., sigmoid colon on the left, caecum on the right) forms part of the wall of the hernia sac
- Needs careful identification at surgery to avoid bowel injury during sac excision - Bailey & Love
Pantaloon (Saddle-bag) Hernia
- Combined direct and indirect hernia straddling the inferior epigastric vessels, creating a "pantaloon" shape
Femoral Hernia
Anatomy
- Protrudes through the femoral canal - a small space just medial to the femoral vein, bounded by:
- Laterally: femoral vein
- Anteriorly: inguinal ligament
- Posteriorly: pectineal (Astley Cooper's) ligament
- Medially: lacunar (Gimbernat's) ligament - has a sharp, unyielding edge that impedes reduction
- Appears below and lateral to the pubic tubercle (inguinal hernia is above and medial)
Key Clinical Points
- Less common than inguinal hernia
- More common in women (wider female pelvis enlarges the femoral canal)
- Commonly seen in thin, elderly women
- Easily missed on examination
- ~50% present as an emergency with strangulation - highest strangulation rate of all hernias
- The femoral pulse is lateral to the hernia; a saphena varix (enlarged saphenous vein) is an important differential - it disappears on lying down and has a fluid thrill - Bailey & Love
Umbilical Hernia
In Children
- Occurs in up to 10% of infants; higher in premature babies and Black infants (8x higher)
- Increases in size with crying; rarely strangulates under age 3
- 95% resolve spontaneously by age 2 - conservative management is appropriate
- Surgical repair is indicated if it persists beyond age 2 - Bailey & Love
In Adults
- Predisposed by obesity, pregnancy, cirrhosis with ascites - conditions that increase intra-abdominal pressure or thin the linea alba
- The neck is often narrow, making strangulation common (~60% at emergency surgery)
- Umbilical hernias account for ~15% of emergency hernia surgery - Sleisenger & Fordtran's
- Paraumbilical hernias (adjacent to but not exactly at the umbilicus) are now classified together with umbilical hernias under current guidelines
Incisional (Ventral) Hernia
- Occurs through a weakness at a previous surgical wound
- Risk factors: wound infection, obesity, malnutrition, steroid use, poor surgical technique, raised intra-abdominal pressure
- Usually has a wide neck - relatively low strangulation rate (~2%) compared with inguinal/femoral types
- Management: surgical repair with mesh (open or laparoscopic). Larger defects require component separation techniques - Bailey & Love; Maingot's
Other Notable Hernias
| Type | Location | Key Feature |
|---|---|---|
| Spigelian | Through the semilunar line at the lateral edge of rectus abdominis | Interparietal (lies between muscle layers); easily missed |
| Obturator | Through the obturator foramen | Causes medial thigh pain (Howship-Romberg sign); more common in thin elderly women |
| Epigastric | Through the linea alba above the umbilicus | Usually contains extraperitoneal fat; small and often painful |
| Lumbar | Through Petit's (inferior) or Grynfeltt-Lesshaft (superior) triangle | Rare; acquired or congenital |
| Richter's | Any hernia site | Only one wall of the bowel is trapped - may strangulate without obstruction; no bowel obstruction symptoms |
| Littre's | Any hernia site | Hernia sac contains a Meckel's diverticulum |
| Maydl's (W hernia) | Any site | Double loop ("W") of bowel in the sac; the intermediate loop inside the abdomen can strangulate |
Diagnosis
Clinical
- History: a groin, abdominal, or other lump that increases with standing, coughing, or straining; reducible on lying down; dragging or aching discomfort
- Examination: impulse on coughing, reducibility, site relative to anatomical landmarks (pubic tubercle, ASIS), transillumination (to differentiate from hydrocele)
Investigations
- Usually clinical - imaging is rarely needed for straightforward hernias
- Ultrasound: useful for occult hernias, differentiating groin masses; limited sensitivity in supine patients (hernia may reduce)
- CT scan: most useful for obese patients, suspected internal hernias, incarcerated/strangulated hernias, or preoperative planning for complex abdominal wall hernias
- MRI: useful for occult or sports hernia (athletic pubalgia) - Bailey & Love
- Herniography (contrast injection into the peritoneum) is rarely used today
Principles of Surgical Repair
Terminology
- Herniorrhaphy: repair by suture closure of the defect alone (used in children, where the anatomy is normal)
- Hernioplasty: reconstruction of the weakened abdominal wall (needed in adults)
Open Repairs (Inguinal)
| Technique | Description |
|---|---|
| Bassini's repair | Classic; approximates conjoint tendon to inguinal ligament; higher recurrence |
| Shouldice repair | 4-layer, running suture repair of transversalis fascia; gold standard tissue repair; ~1-2% recurrence in specialist hands |
| Lichtenstein (tension-free mesh) | 8×15 cm polypropylene mesh over the posterior inguinal canal wall; slit to wrap around the spermatic cord. Most common repair worldwide. Recurrence <2% but chronic pain in up to 20% |
| Open preperitoneal (Stoppa) | Mesh placed in the preperitoneal space via a midline incision; used for complex/recurrent hernias |
Mesh plug repairs (e.g., Perfix plug) are not recommended by the 2018 European Hernia Society (EHS) guidelines due to risks of meshoma and migration into adjacent structures (bladder, bowel, vessels). - Bailey & Love
Laparoscopic Repairs
| Technique | Description |
|---|---|
| TEP (Totally Extraperitoneal) | Mesh placed in preperitoneal space without entering the peritoneal cavity; avoids bowel injury risk |
| TAPP (Transabdominal Preperitoneal) | Mesh placed preperitoneally after entering the peritoneal cavity; allows inspection of the contralateral side |
Femoral Hernia Repair Approaches
- Lockwood (low approach): through the groin below the inguinal ligament; useful for elective cases
- Lotheissen (high approach): via the inguinal canal; risk of weakening the canal
- McEvedy (high extraperitoneal approach): preferred for strangulated femoral hernias as it provides access for bowel resection
Complications of Hernia and Hernia Repair
Complications of Untreated Hernia
- Incarceration (irreducibility)
- Intestinal obstruction
- Strangulation and bowel necrosis
- Perforation, peritonitis, sepsis
Complications of Surgery
- Immediate: bleeding, haematoma, urinary retention, wound complications, femoral nerve block (from local anaesthetic)
- Short-term: seroma (common after laparoscopic repair; may mimic recurrence), wound infection, testicular swelling
- Long-term:
- Recurrence: target <5% at 5 years in specialist centres; mesh repairs have lower rates than suture alone
- Chronic pain (>3 months): affects up to 20% after open mesh repair, less after laparoscopic repair; can be neuralgic (nerve injury or irritation from mesh/suture), somatic, or visceral
- Mesh complications: infection, migration, erosion into viscera, meshoma formation
- Ischaemic orchitis / testicular atrophy: rare but serious; results from damage to the vas deferens or testicular vessels - Bailey & Love
Specialist hernia surgeons have demonstrably lower recurrence and chronic pain rates regardless of the technique used. - Bailey & Love, 28th Ed.
Special Situations
Paediatric Inguinal Hernia
- All congenital; all indirect; due to patent processus vaginalis
- High incarceration risk in infants due to narrow internal ring
- Repaired by herniorrhaphy (ligation of the patent processus vaginalis) without mesh
- If incarcerated but not strangulated: attempt gentle manual reduction under sedation, then repair within 24 h
- Emergency repair if strangulated (may require laparotomy + bowel resection) - Schwartz's Surgery, 11th Ed.
Internal Hernia After Laparoscopic Gastric Bypass
- Incidence 0.2-3% (much higher than with open approach)
- Due to lack of adhesion formation and marked weight loss reducing mesenteric fat (enlarging potential hernia openings)
- Petersen's defect: most common site (posterior to the alimentary limb)
- Presents with intermittent periumbilical pain, nausea, vomiting; CT may be non-diagnostic as the hernia can spontaneously reduce
- All mesenteric defects should be closed at the time of initial RYGB - Maingot's Abdominal Operations
Recent Evidence (2024-2025)
- A systematic review on incarcerated/strangulated inguinal hernias (EAST Practice Management Guideline, 2025) provides updated guidance on urgent surgical intervention, emphasising early operative management for strangulated hernias. [PMID: 40671180]
- A 2025 systematic review on hiatus hernia classification highlights ongoing variability in classification systems for hiatal hernias, emphasising the need for standardisation. [PMID: 40485346]
Generate a comparison poster: open vs. laparoscopic hernia repair
A clean, professional medical comparison poster titled "Hernia Repair: Open vs. Laparoscopic" with two clearly divided columns side by side. Left column header: "Open Repair (Lichtenstein)" with a scalpel/incision icon, right column header: "Laparoscopic Repair (TEP/TAPP)" with a laparoscope icon. Each column contains the following comparison rows with icons: Incision (left: single 5-8cm groin incision; right: 3 small port sites 0.5-1cm), Anesthesia (left: local/spinal/general; right: general anesthesia required), Operative Time (left: 30-45 min; right: 45-60 min), Hospital Stay (left: day surgery; right: day surgery), Return to Activity (left: 2-3 weeks; right: 1-2 weeks), Chronic Pain Risk (left: up to 20%; right: lower, ~10%), Recurrence Rate (left: less than 2%; right: equivalent), Best For (left: unilateral, elderly, high-risk patients, local anesthesia feasible; right: bilateral hernias, recurrent hernias, bilateral repair in one session), Advantages (left: simpler technique, cost-effective, any anesthesia; right: less post-op pain, faster recovery, better for bilateral), Disadvantages (left: higher chronic pain rate, larger scar; right: needs GA, longer learning curve, higher cost). Bottom section shows a summary table. Use a blue and green color scheme, white background, clear medical typography, subtle anatomical diagram of inguinal region in the background watermark. Professional, suitable for a hospital or medical education setting.
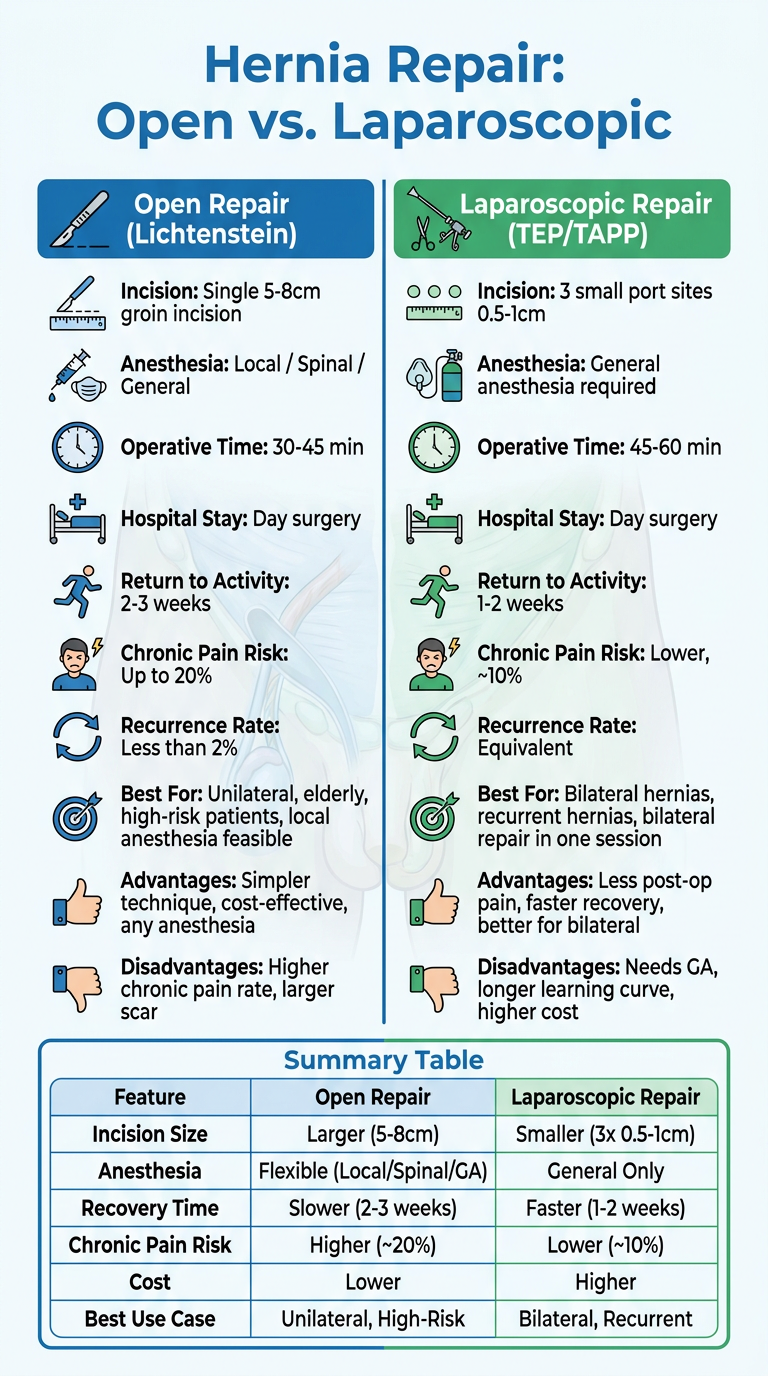
| Parameter | Open (Lichtenstein) | Laparoscopic (TEP/TAPP) |
|---|---|---|
| Incision | Single 5-8 cm groin cut | 3 small ports (0.5-1 cm) |
| Anaesthesia | Local / spinal / general | General only |
| Chronic pain | Up to 20% | ~10% (lower) |
| Recurrence | <2% | Equivalent |
| Recovery | 2-3 weeks | 1-2 weeks |
| Best for | Elderly, high-risk, unilateral | Bilateral, recurrent hernias |
| Cost | Lower | Higher |
| Learning curve | Shorter | Longer |
Create a surgical technique guide (step-by-step) for Lichtenstein repair
Lichtenstein inguinal hernia repair surgical technique steps mesh placement
https://pmc.ncbi.nlm.nih.gov/articles/PMC11297121
Lichtenstein Tension-Free Inguinal Hernia Repair
Step-by-Step Surgical Technique Guide
Principle: Introduced by Dr. Irving Lichtenstein in 1984, this tension-free technique reinforces the posterior wall of the inguinal canal with a flat polypropylene mesh, eliminating the tissue tension that caused pain and high recurrence rates with earlier suture repairs. It is currently the most widely performed inguinal hernia repair in the world.
Pre-operative Preparation
- Inject a field block along the line of incision (subcutaneous and deep to external oblique)
- Infiltrate around the pubic tubercle
- Block the ilioinguinal and iliohypogastric nerves medial to the ASIS
STEP 1 - Skin Incision
- Mark an oblique incision 2 cm above and parallel to the inguinal ligament, running from just medial to the anterior superior iliac spine (ASIS) to just lateral to the pubic tubercle
- Length: 6-8 cm
- Incise skin and subcutaneous fat; ligate or cauterise superficial epigastric and superficial circumflex iliac veins to control bleeding
Current Surgical Therapy 14e
STEP 2 - Exposure of External Oblique Aponeurosis
- Deepen dissection through Camper's and Scarpa's fascia to reach the shiny, white external oblique aponeurosis
- Identify the external (superficial) inguinal ring medially - an inverted V-shaped defect in the aponeurosis
- Create superior and inferior flaps of skin and subcutaneous tissue to expose:
- The full width of the external oblique
- The shelving edge of the inguinal ligament inferiorly
- The aponeurotic portion of internal oblique superiorly
STEP 3 - Opening the Inguinal Canal
- Using Metzenbaum scissors, incise the external oblique along the direction of its fibres, starting at the external ring and extending laterally beyond the level of the deep inguinal ring (superolateral direction)
- This opens the anterior wall of the inguinal canal and exposes its contents
- Evert the two flaps of external oblique aponeurosis and hold them with retractors
Bailey and Love's Short Practice of Surgery, 28th Ed.
STEP 4 - Nerve Identification and Protection ⚠️
| Nerve | Location | Risk |
|---|---|---|
| Ilioinguinal nerve | Runs on the anterior surface of the spermatic cord within the canal | Entrapment in suture or mesh |
| Iliohypogastric nerve | Courses along the anterior surface of the internal oblique, ~1 cm above and medial to the deep ring | Suture injury during superior mesh fixation |
| Genital branch of genitofemoral nerve | Runs within the spermatic cord alongside the external spermatic vein | Injury during cord dissection |
- All three nerves can be identified in 70-90% of cases with careful dissection
- Identification and protection reduces chronic pain incidence to <1% in experienced hands
- If a nerve is trapped, damaged, or likely to be compressed by mesh: perform elective neurectomy at that time (resect a segment and bury the end in muscle)
Lichtenstein technique - 10 recommendations, PMC11297121 (2024)
STEP 5 - Isolation of the Spermatic Cord
- At the level of the pubic tubercle, encircle the spermatic cord (in men) or the round ligament (in women) with a Penrose drain for easy retraction
- Gently separate the cord from the floor (posterior wall) of the canal by blunt dissection
STEP 6 - Hernia Sac Dissection and Management
Indirect Hernia Sac
- The indirect sac lies on the anterolateral surface of the cord
- Divide overlying cremasteric fibres to expose the sac fully
- Separate the sac from the vas deferens and testicular vessels with careful sharp/blunt dissection - avoid injury to the vas
- For small/moderate sacs: simply ligate the sac at the neck with an absorbable suture and excise the distal portion, or invert the sac through the deep ring (no excision needed)
- For large/scrotal sacs: do not attempt full dissection to the neck (risk of haematoma, ischaemic orchitis). Divide the sac at mid-canal, oversew the proximal end, and leave the distal sac in situ (open or closed)
Direct Hernia Sac / Posterior Wall Weakness
- Inspect the posterior wall (floor of the canal) medial to the inferior epigastric vessels
- A direct defect is imbricated or inverted by plication of the transversalis fascia with an absorbable suture
- Unlike suture repairs, there is no attempt to formally reconstruct the floor - the mesh will reinforce it
Current Surgical Therapy 14e; Bailey & Love 28th Ed.
STEP 7 - Mesh Positioning
- Medially: overlap the pubic symphysis by ≥2 cm
- Superiorly: extend 3-4 cm above the inguinal triangle (conjoint tendon)
- Laterally: extend 5-6 cm beyond the internal inguinal ring
- The mesh lies posterior to the spermatic cord, between the cord and the posterior canal wall
- Divide the mesh along its long axis from the lateral end, creating two tails:
- Wider upper tail (approximately 2/3 of the mesh width)
- Narrower lower tail (approximately 1/3)
- These tails will recreate the deep inguinal ring around the cord
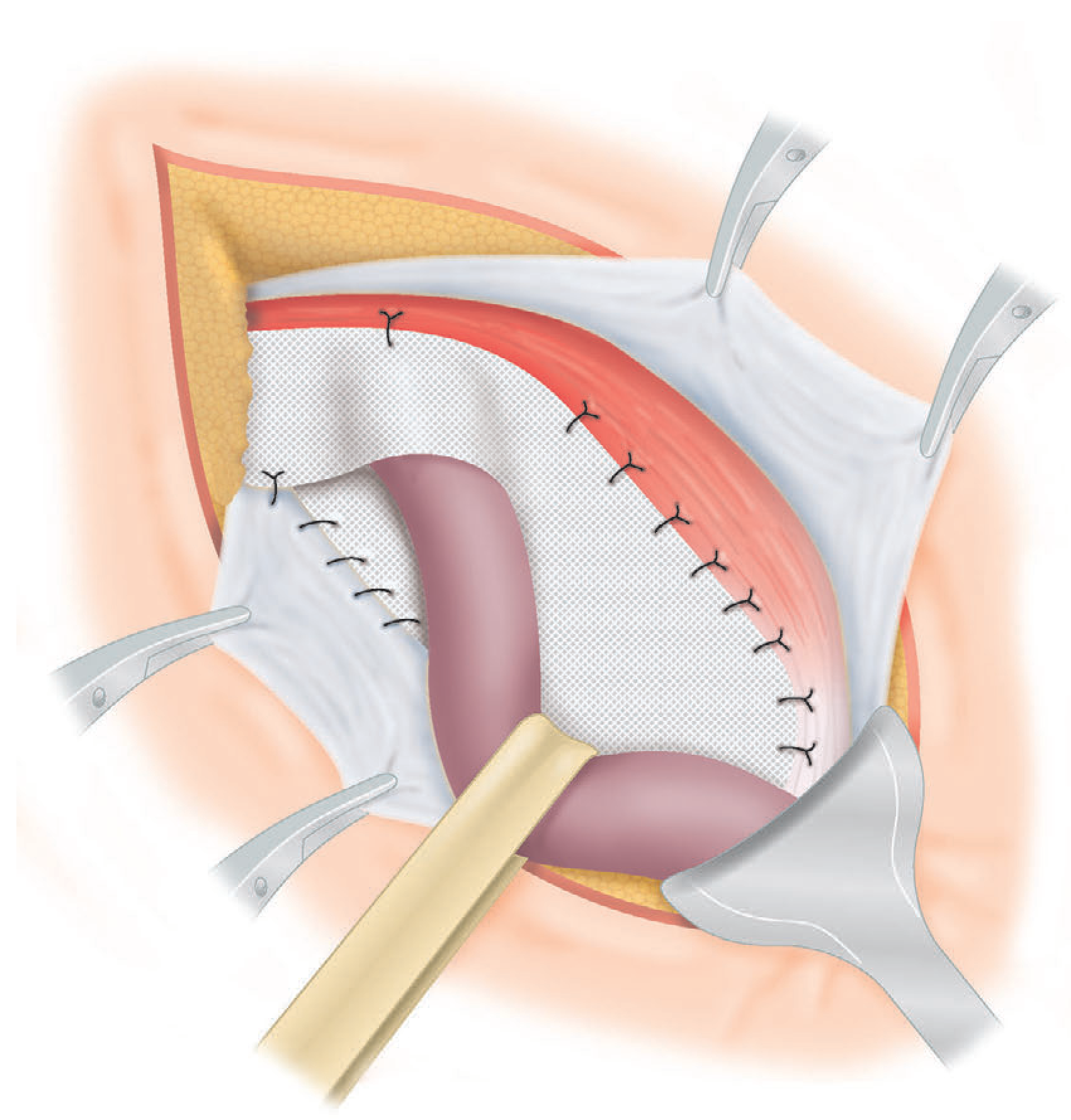
STEP 8 - Mesh Fixation
Zone 1 - Medial Fixation (Pubic Tubercle)
- Secure the medial end of the mesh to the aponeurotic tissue overlying the pubic tubercle with 1-2 interrupted absorbable sutures
- Do NOT stitch to the periosteum of the pubic bone (risk of osteitis)
- Overlap the pubic tubercle by at least 2 cm to prevent medial recurrence
Zone 2 - Inferior Fixation (Inguinal Ligament)
- Using a continuous non-absorbable monofilament suture (e.g., 2-0 prolene), sew the lower edge of the mesh to the inguinal ligament, passing the needle through the ligament 3-4 times
- Run the suture from the pubic tubercle laterally to just past the deep inguinal ring
- Keep the mesh slightly relaxed (dome-shaped) rather than pulled taut - this compensates for mesh contraction and prevents recurrence under intra-abdominal pressure
Zone 3 - Superior Fixation (Internal Oblique / Conjoint Tendon)
- Place interrupted absorbable sutures (NOT running suture) to fix the upper edge of the mesh to the aponeurosis of the internal oblique or the conjoint tendon
- Restricted to medial to the deep inguinal ring - avoid suturing laterally where the iliohypogastric nerve courses
- Sutures should be loosely tied to prevent tissue necrosis and nerve entrapment
Alternative fixation: Cyanoacrylate (surgical glue) or self-adherent mesh - randomised trials (Matikainen 2017, 2021) show equivalent recurrence and chronic pain rates vs. suture fixation, with potentially faster operative time. - Current Surgical Therapy 14e
STEP 9 - Recreating the Internal (Deep) Inguinal Ring
- Cross the two mesh tails behind the spermatic cord (upper tail anterior to lower tail)
- Secure the tails with a single interrupted non-absorbable suture to snugly reform the internal ring around the cord
- The reconstructed ring should admit just the cord without compression - admit a fingertip alongside the cord to confirm adequate laxity
- The lateral portions of the tails lie flat beneath the external oblique
Crossing the tails behind the cord (rather than in front) prevents lateral recurrence. This is one of Lichtenstein's original five operative principles.
STEP 10 - Wound Closure
- External oblique aponeurosis: continuous 2-0 absorbable suture, reconstituting the inguinal canal and re-forming the external ring (should admit just the cord)
- Scarpa's fascia: interrupted 3-0 absorbable suture (reduces dead space and wound seroma)
- Skin: subcuticular 3-0 absorbable suture or surgical staples
Critical Technical Points Summary
| Step | Key Pitfall | How to Avoid |
|---|---|---|
| Nerve identification | Chronic pain from nerve entrapment | Identify all 3 nerves before mesh placement |
| Medial fixation | Medial recurrence if <2 cm pubic overlap | Always overlap pubic tubercle by ≥2 cm |
| Superior suture placement | IH nerve injury | Interrupted sutures only; stay medial to deep ring |
| Mesh tension | Mesh contraction → recurrence/pain | Leave mesh slightly relaxed/domed |
| Sac dissection (large) | Haematoma, ischaemic orchitis | Divide and leave distal sac; don't strip to fundus |
| Keyhole creation | Lateral recurrence | Cross tails behind the cord, not in front |
| Inferior suture | Mesh mobilisation | Pass needle through ligament 3-4 times |
Post-operative Care
- Day surgery in the majority of cases
- Mobilise and eat/drink same day
- Return to light activity: 48-72 hours
- Return to desk work: 1-2 weeks
- Return to manual/heavy labour: 4-6 weeks
- Avoid constipation and straining (stool softeners if needed)
- Scrotal support / ice pack for swelling in the first 24-48 hours
Complications to Counsel Pre-operatively
| Complication | Rate |
|---|---|
| Wound seroma | 5-10% (self-limiting) |
| Haematoma | 1-2% |
| Wound infection | 1-2% |
| Urinary retention | 1-2% |
| Recurrence at 5 years | <5% (specialist centres aim for <2%) |
| Chronic pain (>3 months) | Up to 20% (open mesh); neuralgic type most severe |
| Ischaemic orchitis / testicular atrophy | <0.5% (higher in re-do surgery) |
| Mesh infection / meshoma | Rare |