BP, HR, PR ka apasa me kya relation h... bradycardia Tachycardia Hypertension Hypotension.... bradycardia but normal bp ya raised bp...Tachycardia but low ya normal bp....no puls but bp present.... nr but puls present..hr but no pr...febal puls strong puls...aise aur bhi scenarios bante h...ye sab kaise samje basic to mbbs ang pg lavel tak.....ache samjha do
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Ab main ek bahut detailed, structured answer likhta hun - Basic se MBBS/PG level tak - Hindi-English mix mein.
BP, HR aur PR - Complete Conceptual Guide
Basic se PG Level tak
PART 1: Pehle Teen Terms Ko Alag-Alag Samjho
Bahut log in teeno ko ek samajhte hain - yahi confusion ki jad hai.
| Term | Full Form | Kya Measure Karta Hai | Kahan Measure Hota Hai |
|---|---|---|---|
| HR (Heart Rate) | Heart Rate | Heart kitni baar beat karta hai per minute | ECG / Chest auscultation / Apex beat |
| PR (Pulse Rate) | Pulse Rate | Arteries mein pressure wave kitni baar per minute feel hoti hai | Radial/carotid/femoral artery palpation |
| BP (Blood Pressure) | Blood Pressure | Blood vessels ki wall par blood ka force | Sphygmomanometer / Arterial line |
Key Insight: HR = electrical event, PR = mechanical/vascular event, BP = pressure measurement. Teeno same source se start hote hain (heart) but alag cheezein measure karte hain.
PART 2: Formulas Samjho - Iske Bina Sab Ratta Maarna Padega
Formula 1: BP ka Aadhar
Mean Arterial Pressure (MAP) = Cardiac Output (CO) × Total Peripheral Resistance (TPR)
Formula 2: Cardiac Output
CO = Heart Rate (HR) × Stroke Volume (SV)
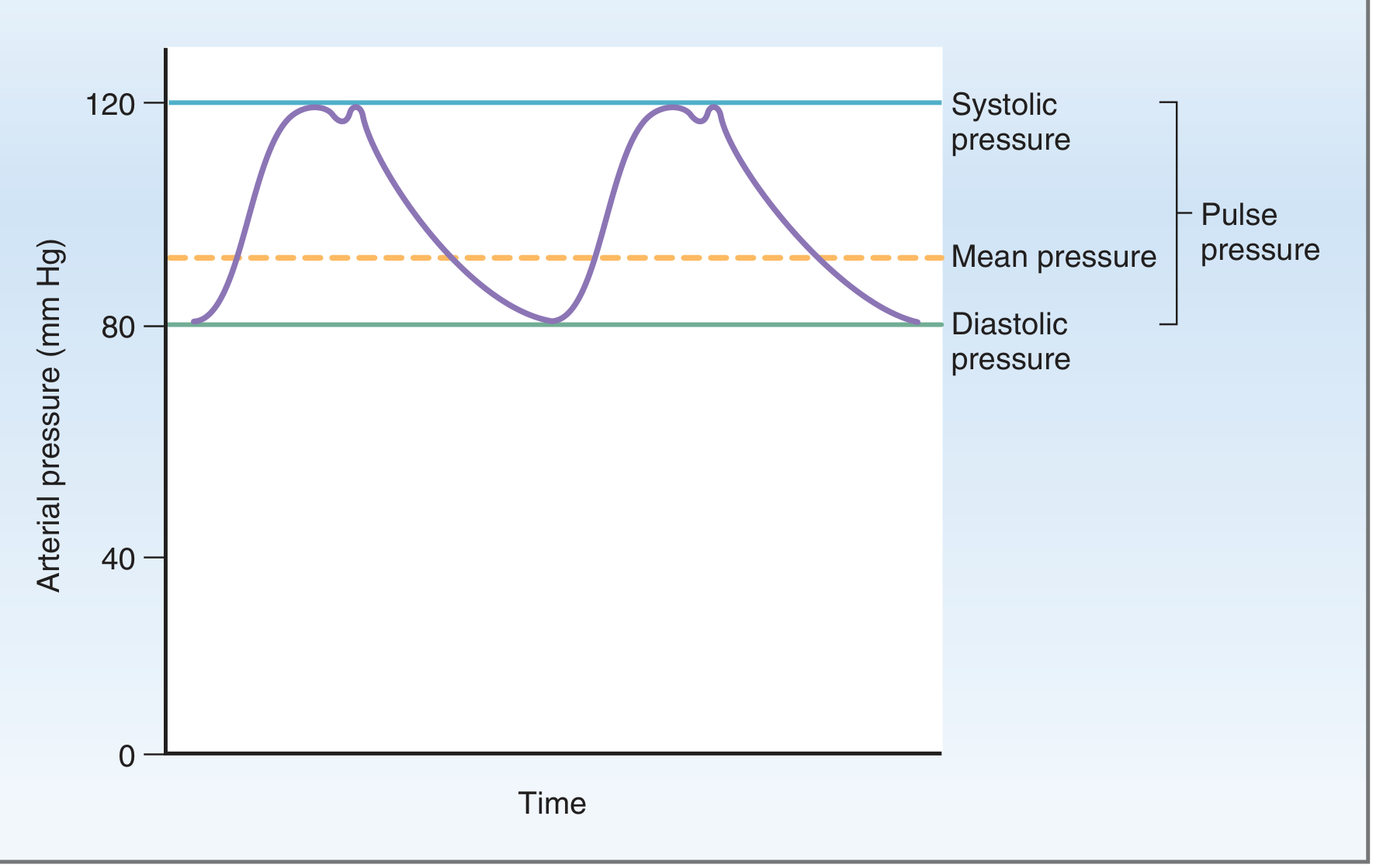
Formula 3: Pulse Pressure (PP)
Pulse Pressure = Systolic BP - Diastolic BP
(Normal: 40 mmHg)
Pulse Pressure directly proportional to Stroke Volume - ye sabse important concept hai!
PART 3: HR aur BP Ka Relation - The Baroreceptor Reflex
Ye ek automatic feedback system hai. Isko samjho toh sab scenarios khud clear ho jaate hain.
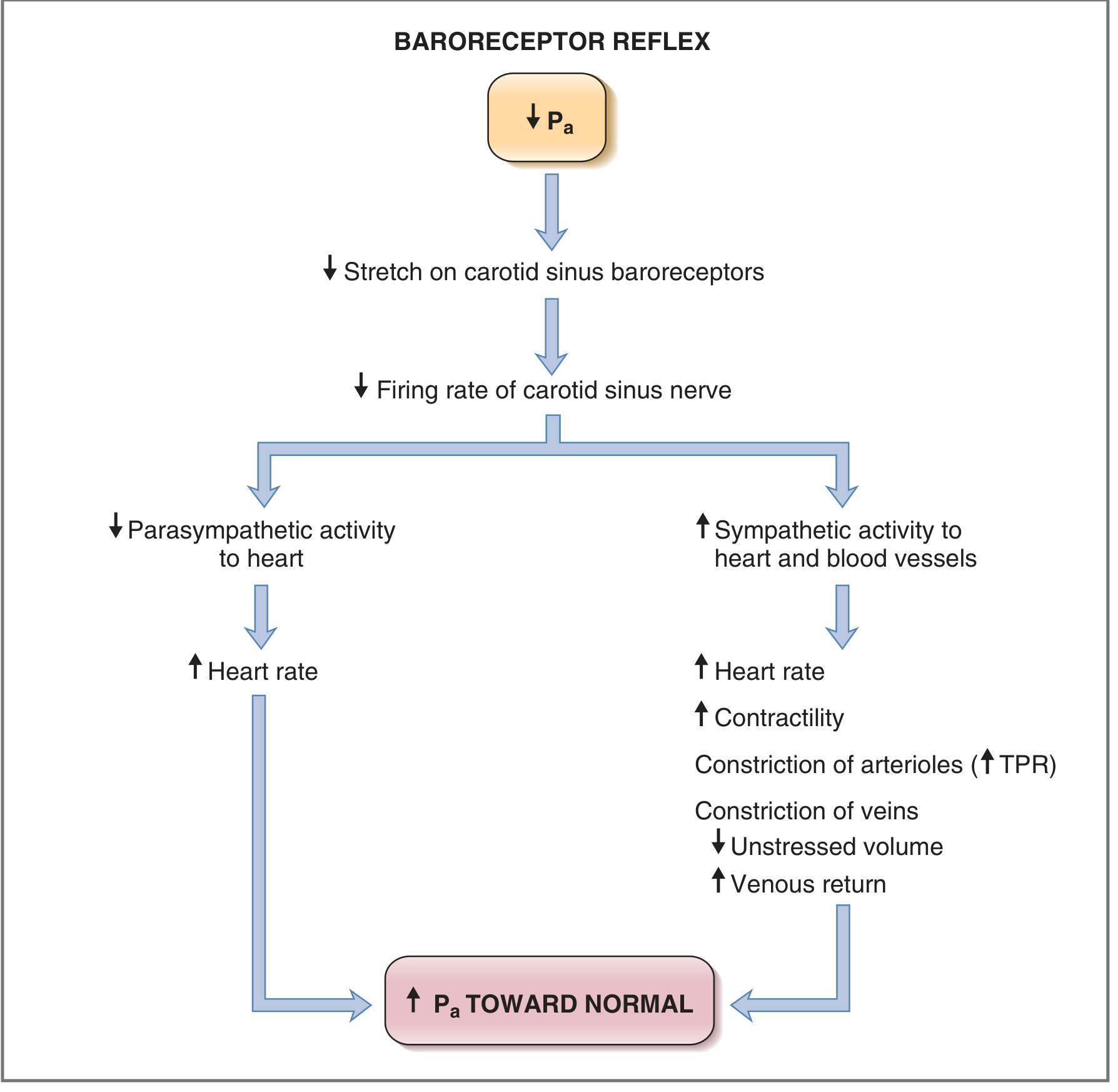
Normal Rule: BP girne par HR badhega (compensatory tachycardia). BP badhne par HR ghategaa (reflex bradycardia).
LEKIN - Ye rule hamesha nahi chalta! Yahi interesting scenarios banate hain.
PART 4: HR vs PR - Kab Alag Hote Hain?
HR = PR (Normal situation)
Har heartbeat ek pulse wave generate karta hai jo radial artery tak pahunchti hai.
HR > PR = "Pulse Deficit"
Matlab: Heart beat kar raha hai, par kuch beats radial artery tak nahi pahunch rahi.
Cause: Woh beats itni weak hain ki unka stroke volume itna kam hai ki peripheral pulse generate nahi ho raha.
Classic Example:
- Atrial Fibrillation (AF) - Ye MBBS/PG ka most tested scenario hai. Irregular atrial activity mein kuch beats bahut jaldi aate hain, filling time kum milta hai, SV almost zero ho jata hai - heart beat hoti hai (HR ECG pe dikhta hai) par pulse nahi milti.
- Frequent Premature Ventricular Contractions (PVCs)
Clinically: Apical HR > Radial PR. Difference = Pulse Deficit. Larger the deficit, worse the cardiac function.
PART 5: Scenarios Systematically Samjho
Scenario 1: Bradycardia but NORMAL/HIGH BP
Concept: HR kam hai, par CO normal ya high ho sakta hai agar SV badhaya jaye.
CO = HR × SV
Agar HR ↓ lekin SV ↑↑ → CO normal → BP normal/high
Real Clinical Examples:
| Condition | Mechanism | HR | BP |
|---|---|---|---|
| Athletes | Trained heart, high SV | 40-50 bpm (resting) | Normal |
| Raised ICP (Cushing's Reflex) | Vagal bradycardia + peripheral vasoconstriction | ↓ | ↑↑ (Hypertension) |
| Hypothyroidism | Decreased chronotropy | ↓ | Normal/↑ diastolic |
| Beta-blocker overdose (mild) | Negative chronotropy | ↓ | May be maintained |
| Carotid Sinus Pressure | Reflex vagal | ↓ | Brief ↓ then normal |
| 2nd Degree Heart Block (Mobitz I) | Blocked beats | ↓ | Normal if compensated |
Cushing's Triad (PG Favourite): Hypertension + Bradycardia + Irregular respirations = Raised ICP. Brain ko khud bachane ki koshish.
Scenario 2: Tachycardia but LOW/NORMAL BP
Most common clinical scenario in emergency!
CO = HR × SV
Agar SV ↓↓ (blood loss, pump failure)
→ HR ↑↑ (compensatory)
→ But CO still low
→ BP ↓ ya marginally maintained
Examples:
| Condition | Why Tachy? | Why Low/Normal BP? |
|---|---|---|
| Hemorrhagic Shock (Class I & II) | Baroreceptor reflex compensation | BP normal initially (compensated), tachy is early sign |
| Septic Shock | SVR drop + fever | Low BP despite very high HR |
| Cardiac Tamponade | Compensatory | Low CO due to external compression |
| Dehydration | Hypovolemia | Orthostatic hypotension with tachy |
| SVT / VT with poor function | The arrhythmia itself | Filling time too short → SV ↓ → BP ↓ |
| PE (Pulmonary Embolism) | Sympathetic surge | RV failure → low CO → low BP |
Golden Rule in Shock: Tachycardia is the EARLIEST sign of hypovolemia. BP normal hone ka matlab safe nahi hai! - Tintinalli's Emergency Medicine
Scenario 3: NO PULSE but BP PRESENT
Ye ek important but tricky concept hai.
Pulseless Electrical Activity (PEA) / EMD:
- ECG pe organized rhythm dikhta hai
- BP measured on arterial line: measurable (sometimes very low like 40-50 systolic)
- Radial pulse palpable nahi
- Kyu? BP itna kam hai ki peripheral vessels collapse ho jaate hain, tactile pulse feel nahi hoti
Braunwald's Heart Disease: "Pulseless sustained VT - a perceptible pulse may not be present (<60 mm Hg systolic)" - Roberts & Hedges' Clinical Procedures in Emergency Medicine
Practical Implication: Pulseless na matlab BP zero. ALWAYS use Doppler or arterial line in shock. Radial pulse disappears at systolic ~70 mmHg, carotid at ~50 mmHg.
Palpable Pulse Threshold:
Carotid: ~60 mmHg systolic
Femoral: ~70 mmHg systolic
Radial: ~80 mmHg systolic
(Memory: R > F > C in pressure required)
Scenario 4: NO BP but PULSE PRESENT
Mechanism: Aortic Regurgitation (AR) is the textbook example!
Wide Pulse Pressure:
- Systolic BP: High (160-200) - kyunki large SV eject hota hai
- Diastolic BP: Very LOW (<40) - kyunki blood regurgitate ho jaata hai LV mein
- Pulse Pressure = 160-30 = 130 mmHg (bahut wide!)
Ye "bounding pulse" deta hai - felt strongly peripherally. Harrison's: "Bounding pulses, wide pulse pressure, diastolic BP typically 60 mmHg or less" - Harrison's Principles of Internal Medicine 22E
Other causes of wide pulse pressure (strong/bounding pulse):
- Hyperthyroidism
- Fever / severe anemia
- AV fistula
- Severe bradycardia (large SV per beat)
- Beriberi (wet)
Scenario 5: FEEBLE PULSE (Pulse present, barely palpable)
Narrow Pulse Pressure = Small difference between Systolic and Diastolic
Narrow PP = Low SV OR Increased Arterial Stiffness
Causes:
| Condition | Mechanism | Clinical |
|---|---|---|
| Aortic Stenosis | Low SV (obstruction) + slow rise | Pulsus parvus et tardus - small, slow rising pulse |
| Cardiac Tamponade | Low filling → Low SV | Pulsus paradoxus + feeble pulse |
| Severe LV failure | Poor contractility → Low SV | Feeble, rapid pulse |
| Hemorrhagic Shock (advanced) | Low volume → Low SV | Thready/feeble rapid pulse |
| Constrictive Pericarditis | Low filling | Feeble, JVP raised |
Pulsus Parvus et Tardus: AS ka pathognomonic - small amplitude, late-peaking, slow-rising pulse. Ye feel karo carotid artery pe - "anacrotic shoulder" bhi feel ho sakti hai.
Scenario 6: STRONG/BOUNDING PULSE
Wide pulse pressure ke causes (as above in AR section).
Additional unique ones:
- Aortic regurgitation - most classic
- Complete Heart Block - bradycardia → large SV per beat → wide PP → bounding pulse
- PDA (Patent Ductus Arteriosus) - diastolic run-off → low diastolic → wide PP → bounding/hyperkinetic pulse
Scenario 7: HR Present but NO PR - (Pulse Deficit - Revisited)
Already covered above (AF, frequent PVCs). Let me add more:
Complete scenario in AF:
- Heart has electrical activity (HR on ECG: say 120)
- Some beats contract well → good SV → pulse reaches radial (PR: say 80)
- Some beats contract poorly (very short RR interval before them) → SV negligible → no radial pulse
- Pulse Deficit = HR - PR = 120 - 80 = 40
- Larger deficit = more hemodynamically significant AF
PART 6: The BIG PICTURE - Master Table
| Scenario | HR | PR | BP | Classic Cause |
|---|---|---|---|---|
| Normal | 60-100 | = HR | 120/80 | Healthy |
| Athlete | ↓ (40-50) | = HR | Normal | Training |
| Sinus Brady + ↑BP | ↓ | = HR | ↑↑ | Raised ICP (Cushing's Triad) |
| Tachy + ↓BP | ↑↑ | = HR | ↓ | Hemorrhagic shock, sepsis |
| Tachy + Normal BP | ↑ | = HR | Normal | Compensated early hemorrhage, PE |
| Pulse Deficit (HR > PR) | ↑ | < HR | Variable | AF, PVCs |
| Bounding Pulse + Wide PP | ↓ or normal | = HR | High systolic, low diastolic | AR, Thyrotoxicosis |
| Feeble Pulse + Narrow PP | ↑ | < real HR tactilely | Low-normal systolic | AS, Tamponade, Severe LV failure |
| No Pulse + some BP on line | Variable | Absent | Very low (30-60 systolic) | PEA, PEA/EMD |
| Brady + Normal BP | ↓ | = HR | Normal | Athletic training, sleep, AV blocks |
PART 7: PG-Level High-Yield Special Pulses
| Pulse Name | Description | Disease |
|---|---|---|
| Pulsus Paradoxus | >10 mmHg fall in SBP during inspiration | Cardiac Tamponade, severe asthma |
| Pulsus Alternans | Alternating strong and weak beats, regular rhythm | Severe LV failure |
| Pulsus Bisferiens | Two systolic peaks per beat | Mixed AS + AR, HCM |
| Pulsus Parvus et Tardus | Small amplitude, slow rise | Severe AS |
| Corrigan/Water-Hammer Pulse | Rapid rise, rapid collapse (bounding) | Aortic Regurgitation |
| Dicrotic Pulse | One systolic + one diastolic peak | Severe cardiac failure, septic shock |
| Anacrotic Pulse | Notch on ascending limb | Severe AS |
PART 8: Exam Memory Tricks
"CAR" for Compensatory Tachycardia in Shock:
- C - CO falls
- A - Adrenergic activation
- R - Rate increases
Cushing's Triad: "BHI BHI" = Bradycardia, Hypertension, Irregular respiration = Raised ICP
Pulse Pressure = Stroke Volume indicator:
- Wide PP (>60) → High SV (AR, thyrotoxicosis, fever, anaemia)
- Narrow PP (<25) → Low SV (AS, tamponade, LV failure)
Pulse Deficit: Apex HR - Radial PR = Pulse Deficit. Only in AF typically (PG MCQ favourite)
Radial pulse disappears at Systolic BP ~80 mmHg - isliye no pulse + BP present ho sakta hai if BP 40-70 range mein hai (PEA scenario)
Summary in one line: BP = CO x TPR, CO = HR x SV. HR aur PR normally same hain but alag ho sakte hain (pulse deficit). BP aur HR antagonistically connected hain baroreceptor reflex se - lekin yahi reflex override ya bypass ho sakta hai multiple conditions mein, isliye ye ajeeb combinations milte hain clinically.
Sources: Costanzo Physiology 7th Ed | Ganong's Review of Medical Physiology 26th Ed | Medical Physiology (Boron & Boulpaep) | Harrison's Principles of Internal Medicine 22E | Tintinalli's Emergency Medicine | Roberts & Hedges' Clinical Procedures in Emergency Medicine | Braunwald's Heart Disease 12E
This is a shared conversation. Sign in to Orris to start your own chat.