Chronic diarrhoea
Reading File
Finding Sources
Searching PubMed
"chronic diarrhea" AND diagnosis AND management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
I now have comprehensive information to build a thorough answer. Let me compile it.
Chronic Diarrhoea
Definition
Diarrhoea is defined as a stool weight >200 g/day with increased liquidity or frequency (>3 stools/day). It is classified as chronic when it persists for >4 weeks. This separates it from acute and sub-acute forms and shifts the diagnostic focus toward non-infectious and structural causes.
Pathophysiological Classification
Chronic diarrhoea is best understood through its mechanism, which also drives the investigative pathway:
1. Osmotic (Watery)
Caused by osmotically active, poorly absorbed solutes drawing water into the lumen. Key feature: stops with fasting.
- Carbohydrate malabsorption (lactase deficiency, fructose intolerance)
- Osmotic laxatives: Mg²⁺, PO₄³⁻, SO₄²⁻
- Osmotic gap >125 mOsm/kg
2. Secretory (Watery)
Net secretion of electrolytes into the gut lumen, persisting with fasting. Osmotic gap is <50 mOsm/kg.
- Endocrinopathies: VIPoma, gastrinoma, carcinoid syndrome (5-HIAA), medullary thyroid carcinoma (calcitonin), pheochromocytoma, mastocytosis, hyperthyroidism, Addison's disease, somatostatinoma
- Microscopic colitis (collagenous and lymphocytic)
- IBD (Crohn's, UC)
- Bile acid malabsorption (ileal resection/disease)
- Neoplasia: colon carcinoma, lymphoma, villous adenoma (rectum)
- Medications and laxative abuse
- Idiopathic: Brainerd (epidemic) diarrhea, sporadic secretory diarrhea
- Bacterial toxins, SIBO (also contributes to fatty diarrhoea)
- Disordered motility: IBS, diabetic autonomic neuropathy, post-vagotomy, post-sympathectomy
3. Fatty (Steatorrhoea)
Suggests malabsorption or maldigestion. Stool fat >7 g/day on a standard fat diet.
- Malabsorption: Celiac disease, Whipple's disease, short bowel syndrome, SIBO, mesenteric ischaemia
- Maldigestion: Pancreatic exocrine insufficiency, inadequate luminal bile acid (cholestatic liver disease, ileal disease/resection)
4. Inflammatory
Blood or leukocytes/calprotectin in stool signals mucosal disruption.
- IBD (Crohn's, UC, ulcerative jejunoileitis)
- Invasive infections: TB, yersiniosis, amebiasis, strongyloidiasis, C. difficile, CMV, HSV
- Ischaemic colitis
- Radiation enteritis
- Colorectal neoplasia
Note: These categories overlap - e.g. celiac disease causes both osmotic and secretory diarrhoea; gastrinoma may cause either.
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
- Harrison's Principles of Internal Medicine, 22nd ed. (2025)
Key Alarm Features ("Red Flags")
These warrant urgent investigation:
- Age >50 years or new onset in older patients
- Rectal bleeding / haematochezia
- Nocturnal diarrhoea (waking from sleep)
- Significant unintentional weight loss
- Anaemia, hypoalbuminaemia, elevated CRP
- Family history of IBD or colorectal cancer
- Recent antibiotic use (consider C. difficile)
- Immunocompromised state
Diagnostic Approach
History
Characterise: onset, duration, stool frequency and consistency (Bristol Stool Scale), relation to fasting, nocturnal episodes, fat in stool (floating, greasy, hard to flush), blood, mucus, pain (relation to bowel movements - relieved by BM suggests IBS), urgency, tenesmus.
Ask about: travel, medications (especially antibiotics, NSAIDs, PPIs, metformin, colchicine, laxatives), diet (lactose, sorbitol, fructose, alcohol), family history (IBD, celiac), prior surgery (ileal resection, cholecystectomy, vagotomy), radiation therapy.
Physical Examination
Look for: dermatitis herpetiformis (celiac), erythema nodosum (UC), flushing (carcinoid), oral aphthous ulcers (IBD/celiac), thyroid mass, heart murmurs, arthritis, peripheral oedema, hepatomegaly, abdominal mass, lymphadenopathy, perianal fistulas, anal sphincter laxity, orthostatic hypotension (autonomic neuropathy).
Initial Laboratory Screen (Box 16.6 - Sleisenger)
| Blood Tests | Stool Tests |
|---|---|
| CBC (anaemia, eosinophilia) | Faecal occult blood |
| Comprehensive metabolic panel | Faecal calprotectin or lactoferrin (sensitivity 92%, specificity 82% for inflammation) |
| IgA tissue transglutaminase + total IgA | Bacterial culture, O&P, Giardia and Cryptosporidium antigens or multiplex PCR |
| CRP/ESR | Qualitative or quantitative stool fat (Sudan stain: sensitivity 76%, specificity 99%) |
Stool Osmotic Gap
- Calculated as: 290 − 2 × (stool Na⁺ + stool K⁺)
- <50 mOsm/kg → secretory
-
125 mOsm/kg → osmotic
Directed Investigation by Mechanism
Fatty diarrhoea:
- Upper endoscopy + small-bowel biopsy (celiac, Whipple's)
- Small-bowel MRI/CT enterography
- Pancreatic function tests (faecal elastase, secretin stimulation)
- Stool fat >20 g/day → pancreatic cause likely; 14-20 g/day → small bowel cause
Secretory diarrhoea:
- Stool volume, osmolality, pH; laxative screen
- Hormonal screen: serum gastrin, VIP, calcitonin, TSH, urinary 5-HIAA, urinary metanephrines, chromogranin A, somatostatin
- Consider ACTH stimulation test (Addison's), immunoglobulins, serum protein electrophoresis
Inflammatory diarrhoea:
- Colonoscopy with ileoscopy + biopsies (diagnostic yield up to 30% in chronic diarrhoea)
- Even normal mucosa should be biopsied - microscopic colitis (lymphocytic/collagenous) is only visible histologically
- CT/MRI abdomen and pelvis
IBS / Functional diarrhoea (Rome criteria met, no alarm features):
- Flexible sigmoidoscopy with biopsies to exclude microscopic colitis
- Consider empirical trials: low-FODMAP/lactose-exclusion diet, bile acid sequestrant (cholestyramine), rifaximin for SIBO
Diagnostic Algorithm
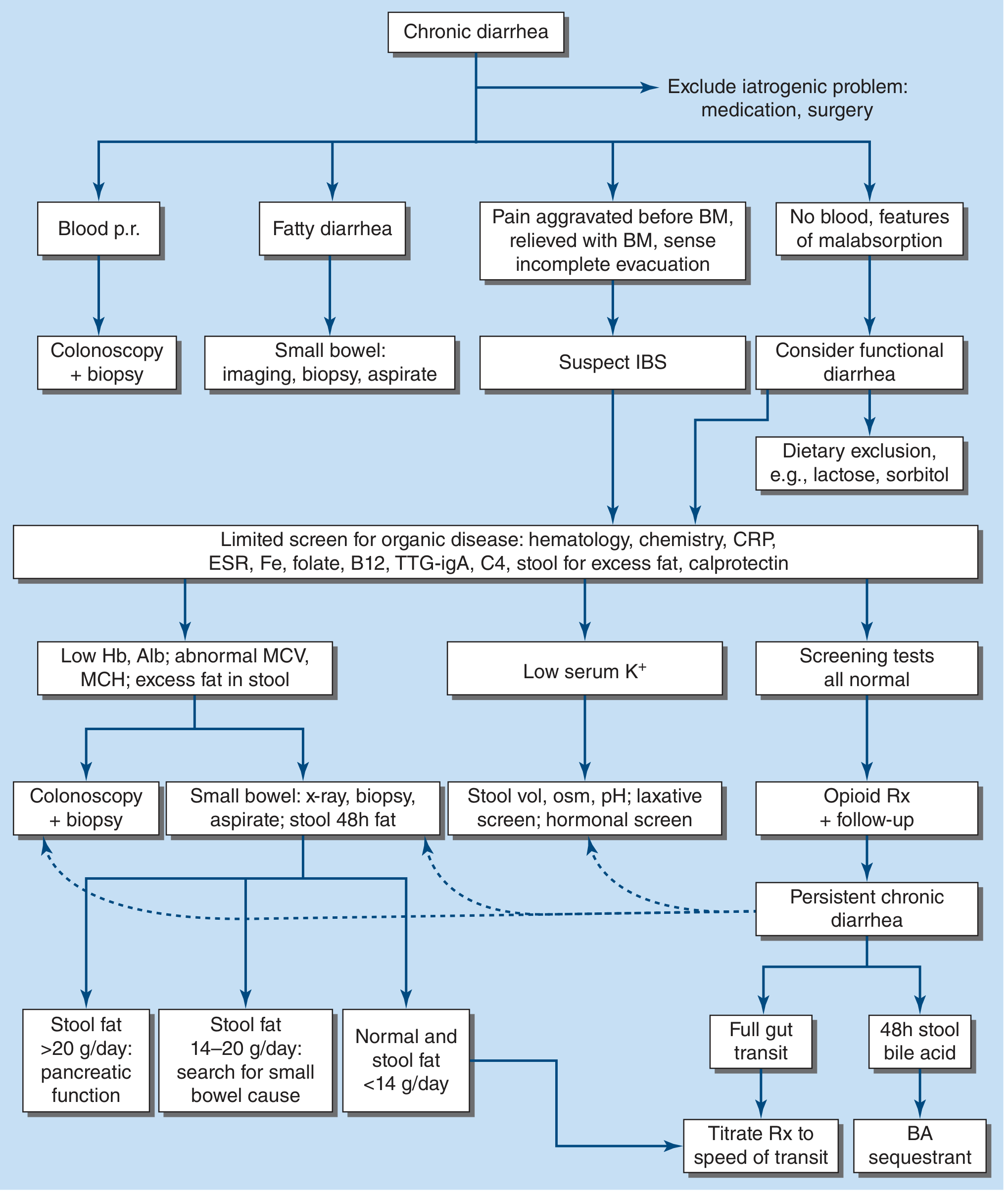
Algorithm for management of chronic diarrhoea. Reproduced from Harrison's Principles of Internal Medicine 22E (2025).
Management
Treatment is directed by aetiology and may be curative, suppressive, or empirical:
| Goal | Example |
|---|---|
| Curative | Resection of colorectal cancer; antibiotics for Whipple's disease or tropical sprue; drug discontinuation |
| Suppressive - dietary | Lactose restriction (lactase deficiency), gluten-free diet (celiac) |
| Suppressive - pharmacological | Anti-inflammatory agents (IBD); bile acid sequestrants (cholestyramine, colestipol, colesevelam for bile acid malabsorption); PPIs (gastrinoma); octreotide (carcinoid syndrome, VIPoma); indomethacin (medullary thyroid carcinoma); pancreatic enzyme replacement (pancreatic insufficiency) |
| Symptomatic (mild-moderate) | Loperamide, diphenoxylate (avoid in severe IBD - risk of toxic megacolon) |
| Symptomatic (severe) | Codeine or tincture of opium |
| IBS-D specific | 5-HT₃ antagonists (alosetron, ondansetron); rifaximin (non-absorbed antibiotic); eluxadoline (μ-opioid/κ-opioid agonist, δ-opioid antagonist - caution: sphincter of Oddi spasm, especially post-cholecystectomy); clonidine (diabetic autonomic diarrhoea - watch for orthostatic hypotension) |
| HIV/AIDS diarrhoea | Crofelemer (antisecretory agent) |
Supportive care: Fluid and electrolyte replacement is essential in all patients. Replacement of fat-soluble vitamins (A, D, E, K) in chronic steatorrhoea.
Specific Conditions to Highlight
Microscopic Colitis
Presents as chronic, watery, non-bloody diarrhoea; most common in middle-aged to elderly women. Normal colonoscopic appearance - diagnosis requires biopsy. Two subtypes: collagenous colitis (thickened subepithelial collagen band) and lymphocytic colitis (increased intraepithelial lymphocytes). Common triggers: NSAIDs, PPIs, SSRIs.
Bile Acid Malabsorption (BAM)
After terminal ileal resection or disease (Crohn's), bile acids escape into the colon causing secretory diarrhoea. Diagnosed with SeHCAT test (75Se-labelled bile acid retention) or serum C4 (7α-hydroxy-4-cholesten-3-one). Treatment: bile acid sequestrants.
Celiac Disease
IgA anti-tissue transglutaminase antibody (with total IgA to exclude IgA deficiency); confirmed by duodenal biopsy (villous atrophy, crypt hyperplasia, intraepithelial lymphocytosis). Treatment: strict gluten-free diet.
SIBO (Small Intestinal Bacterial Overgrowth)
Glucose-hydrogen breath test (screening); gold standard is quantitative small bowel aspirate culture (>10⁵ CFU/mL). Causes both secretory and fatty diarrhoea. Treatment: antibiotics (rifaximin preferred), then address predisposing cause.
Sources: Harrison's Principles of Internal Medicine 22E (2025), p. 354-355 | Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Ch. 16
Generate a summary table comparing medication causes of chronic diarrhea
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive data from Sleisenger, Yamada, and Goldman-Cecil. Here is the detailed comparison table:
Medication-Induced Chronic Diarrhoea: Summary Table
Over 700 medications are recognised as potential causes of diarrhoea. The key to diagnosis is a thorough medication history on initial consultation - this can prevent an extensive, costly, and often invasive workup.
Comparison by Drug Class
| Drug Class | Key Agents | Mechanism | Diarrhoea Type | Notes |
|---|---|---|---|---|
| Antibiotics | Amoxicillin, clindamycin, cephalosporins, tetracycline, neomycin | Disruption of gut microbiota; C. difficile overgrowth | Secretory / Inflammatory | C. difficile colitis is the most serious complication; PPIs also increase this risk |
| Proton Pump Inhibitors (PPIs) | Omeprazole, lansoprazole, pantoprazole | Altered gastric pH → SIBO; promotes C. difficile growth; may cause microscopic colitis | Secretory / Inflammatory | Collagenous colitis linked to long-term use |
| H₂-receptor Antagonists | Ranitidine, famotidine | Altered gastric pH, similar to PPIs but lesser degree | Secretory | Less implicated than PPIs |
| Magnesium-containing antacids | Mg(OH)₂ antacids, Mg supplements | Osmotic - poorly absorbed Mg²⁺ draws water into lumen; also prosecretory at high doses | Osmotic | Stops with drug withdrawal; osmotic gap elevated |
| Laxatives / Cathartics | Senna, bisacodyl, castor oil, anthraquinones, phenolphthalein, dioctyl sodium sulfosuccinate | Stimulation of colonic secretion (stimulant laxatives); osmotic agents (Mg²⁺, sorbitol, lactulose, PO₄³⁻) | Osmotic (osmotic laxatives) / Secretory (stimulant laxatives) | Laxative abuse is a cause of secretory diarrhoea that persists with fasting |
| Metformin | Metformin | Increased intestinal motility; serotonin release; altered bile acid metabolism; microbiome changes | Secretory / Motility | Up to 30% of patients; dose-dependent; extended-release form better tolerated |
| NSAIDs | Ibuprofen, naproxen, mefenamic acid, phenylbutazone | Mucosal injury (prostaglandin inhibition); enteropathy; colitis | Inflammatory | Can cause or unmask microscopic colitis |
| Olmesartan (ARB) | Olmesartan | Sprue-like enteropathy - villous atrophy mimicking celiac disease | Malabsorptive | Accounts for up to 22% of idiopathic sprue cases; anti-TTG may be negative; resolves on drug withdrawal |
| ACE Inhibitors | Enalapril, ramipril, lisinopril | Visceral angioedema | Watery / Secretory | Presents with abdominal pain and diarrhoea; no urticaria or rash in visceral form |
| Beta-blockers | Propranolol, atenolol | Increased gut motility (beta-2 blockade reduces relaxation of gut smooth muscle) | Motility | |
| Immune Checkpoint Inhibitors (ICIs) | Nivolumab, pembrolizumab, ipilimumab (anti-CTLA-4) | Immune-mediated colitis / enteritis (autoimmune T-cell activation) | Inflammatory | Occurs in up to 40% of patients; can be fatal if untreated; treat with corticosteroids; anti-CTLA-4 > anti-PD-1 |
| Chemotherapy | 5-fluorouracil (5-FU), irinotecan, capecitabine, methotrexate, doxorubicin, cytarabine | Direct mucosal cytotoxicity; crypt cell destruction; reduced absorptive surface | Secretory / Inflammatory | Irinotecan: early (cholinergic) and late (secretory) diarrhoea; 5-FU + leucovorin: severe watery diarrhoea |
| Colchicine | Colchicine | Damages enterocyte membrane; inhibits microtubule-dependent absorption | Malabsorptive | Dose-dependent; common at therapeutic doses for gout |
| Gold salts | Auranofin (oral gold) | Intestinal inflammation | Inflammatory | |
| 5-Aminosalicylates (5-ASA) | Mesalazine, sulfasalazine | Paradoxical worsening of colitis; direct mucosal irritation | Inflammatory | Particularly relevant in IBD patients - must distinguish drug effect from disease flare |
| Prostaglandin analogues | Misoprostol | Directly stimulates intestinal secretion and motility | Secretory / Motility | Common dose-limiting side effect |
| Antiarrhythmics | Quinidine, digitalis, procainamide | Altered gut motility; direct mucosal effect | Motility / Secretory | |
| Antiretrovirals | Lopinavir/ritonavir, nelfinavir, didanosine | Multiple mechanisms - altered motility, malabsorption, microbiome disruption | Mixed | Very common; lopinavir/ritonavir is a major offender |
| Theophylline | Theophylline | cAMP-mediated secretion; increased gut motility | Secretory / Motility | Narrow therapeutic index; toxicity common |
| Cholestyramine / Bile acid sequestrants | Cholestyramine, colestipol, colesevelam | Bind bile acids → malabsorption of fat-soluble substances; paradoxically, at high doses cause malabsorptive diarrhoea (especially post-ileal resection) | Malabsorptive | Used therapeutically for bile acid diarrhoea but can cause diarrhoea when bile acid pool is overwhelmed |
| Selective Serotonin Reuptake Inhibitors (SSRIs) | Fluoxetine, sertraline | Increased serotonin → gut hypermotility (5-HT₄ activation); associated with microscopic colitis | Motility / Inflammatory | |
| Statins | Atorvastatin, simvastatin, rosuvastatin | Unclear; possible direct mucosal effect | Secretory | Uncommon but documented |
| Levothyroxine | Levothyroxine (synthroid) | Hyperthyroid state → accelerated gut transit | Motility | More common with over-replacement |
| Levodopa | Levodopa | Dopaminergic effect on gut motility; often also due to GI formulation | Motility | |
| Ursodeoxycholic / Chenodeoxycholic acid | UDCA, CDCA | Secretory effect in colon when reaching high luminal concentrations | Secretory | CDCA used historically for gallstones - high rate of diarrhoea |
| Herbal products / supplements | Senna, aloe, high-dose vitamin C, magnesium supplements | Osmotic or stimulant laxative effects | Osmotic / Secretory | Often underreported by patients |
| Heavy metals | Arsenic, lead, mercury | Direct mucosal toxicity | Inflammatory |
Mechanistic Summary
| Mechanism | Examples |
|---|---|
| Osmotic | Mg antacids, lactulose, sorbitol, PO₄, osmotic laxatives, magnesium supplements |
| Secretory | Stimulant laxatives, misoprostol, theophylline, SSRIs, 5-FU, bile acids (colon) |
| Motility / dysmotility | Metformin, levodopa, beta-blockers, SSRIs, levothyroxine |
| Mucosal injury / malabsorption | Colchicine, neomycin, methotrexate, olmesartan (sprue-like), NSAIDs |
| Microbiome disruption | Antibiotics, PPIs, antiretrovirals |
| Immune-mediated colitis | Checkpoint inhibitors (nivolumab, pembrolizumab, ipilimumab), gold salts |
| Visceral angioedema | ACE inhibitors |
Clinical Pearls
- Olmesartan must always be considered in unexplained malabsorptive diarrhoea - biopsy shows villous atrophy but anti-TTG is negative; stopping the drug is curative.
- Checkpoint inhibitors cause colitis that can be life-threatening (grade 3-4 in ~10%); fecal calprotectin and endoscopic biopsy are key.
- Irinotecan has two distinct diarrhoea phases: early (within 24h, cholinergic - treat with atropine) and late (>24h, secretory - treat with loperamide).
- Laxative abuse causes secretory diarrhoea that persists with fasting - consider a laxative screen (urine/stool) in unexplained cases.
- The principle of management for all drug-induced diarrhoea is discontinuation or substitution of the offending agent where possible.
Sources: Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Box 16.4 | Yamada's Textbook of Gastroenterology, 7th ed., Box 35.7 | Goldman-Cecil Medicine, International Edition
This is a shared conversation. Sign in to Orris to start your own chat.