AMBU bag in neonate, different part of its and how to use with proper picture
Reading File
Finding Sources
Finding Sources
Searching the Web
AMBU bag parts neonatal bag valve mask ventilation diagram labeled
Finding Sources
Loading Image
Searching the Web
neonatal AMBU bag how to use steps technique newborn resuscitation
Loading Image
Loading Image
Reading Web Page
https://www.neoresus.org.au/wp-content/uploads/2015/01/Opera…
I now have excellent material. Let me compile the comprehensive answer.
AMBU Bag (Bag-Valve-Mask) in Neonates
The AMBU bag (Artificial Manual Breathing Unit), also called a self-inflating bag-valve-mask (BVM), is the most common device used for positive pressure ventilation (PPV) in neonatal resuscitation. About 10% of neonates need breathing assistance at birth, and the AMBU bag is the first-line tool.
Parts of a Neonatal AMBU Bag (Labeled Diagram)
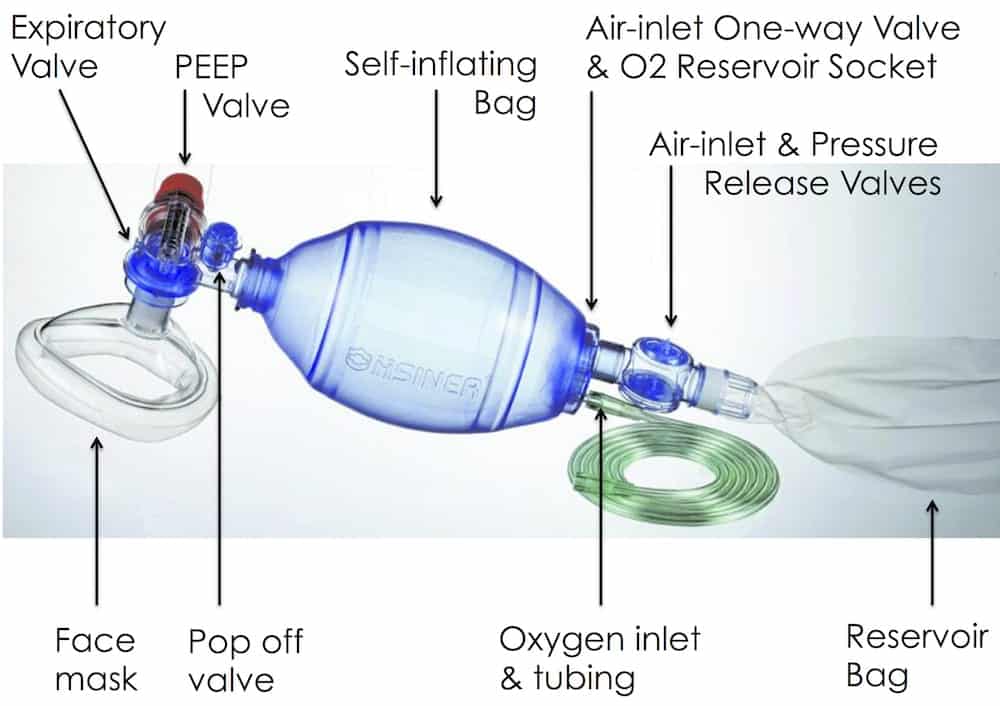

Parts Explained
1. Self-Inflating Bag
- The main compressible chamber (240 mL for neonates - this is the correct size for newborn resuscitation)
- Re-inflates automatically after each squeeze by drawing in air/oxygen
- Do NOT need a pressurized gas source to function - it works on room air alone
- In neonates: use a 240 mL bag (never adult 1600 mL bags)
2. Face Mask
- Sits over the baby's nose and mouth, creating an airtight seal
- Neonatal masks come in size 0 (premature) and size 1 (term newborn)
- Correct size: covers from the bridge of the nose down to just below the lower lip - must not cover the eyes or overlap the chin
- Typically made of soft, transparent silicone for visualization of lip color and secretions
3. Patient Valve (Non-Rebreathing / One-Way Valve)
- Sits between the bag and the mask
- Directs gas flow one way - from bag to patient during inspiration
- During expiration, opens the expiratory valve so exhaled air exits to atmosphere (not back into the bag)
- Prevents rebreathing of CO2
4. Pop-Off Valve (Pressure Relief Valve / Pressure-Limiting Valve)
- Critical safety feature for neonates
- Factory-set at 35-45 cmH2O - automatically releases excess pressure above this threshold
- Protects delicate neonatal lungs from barotrauma and pneumothorax
- Can be occluded manually with a finger when higher pressure is needed (e.g., in meconium cases) - but use with caution
5. Oxygen Inlet (O2 Inlet Tube + Tubing)
- Located at the tail end of the bag
- Connects to an oxygen source via standard green tubing
- Flow rate for neonates: minimum 5 L/min to deliver 40-60% O2 (without reservoir)
6. Reservoir Bag (O2 Reservoir)
- Attached to the oxygen inlet at the distal end of the bag
- Stores 100% O2 between squeezes
- With reservoir bag + ≥5 L/min flow: delivers 90-100% O2
- Without reservoir: delivers only ~40% O2
- Per MSF guidelines: connect O2 reservoir after 2 minutes of ventilation if oxygen is available - start with room air first
7. Air-Inlet One-Way Valve (Fish-Mouth / Inlet Valve)
- At the base of the bag near the O2 inlet
- Allows ambient air to rush into the bag as it re-expands after a squeeze
- Ensures bag re-inflates quickly between breaths
8. PEEP Valve (optional add-on)
- Some neonatal bags include an attachable PEEP (Positive End-Expiratory Pressure) valve
- Typically set at 5 cmH2O in neonates to maintain FRC (functional residual capacity)
How to Use - Step-by-Step (Neonatal)
Pre-Use Preparation
| Step | Action |
|---|---|
| 1 | Choose correct bag size - 240 mL for all neonates |
| 2 | Choose correct mask size - Size 0 (preterm) or Size 1 (term) |
| 3 | Assemble the bag, mask, and all valves - ensure all valves are seated properly |
| 4 | Test the bag - press the mask firmly against your palm and squeeze repeatedly. You must feel air pressure against your hand. If no resistance: do NOT use that device |
| 5 | Test the pop-off valve - occlude the patient port with your thumb and squeeze. Listen/look for the valve releasing at 35-45 cmH2O |
| 6 | If using O2: connect tubing and confirm the reservoir bag inflates |
Positioning the Baby
- Place the neonate on a firm, flat, warm surface
- Neck in neutral "sniffing" position - a small shoulder roll (~2 cm folded cloth) under the shoulders helps
- Avoid hyperextension or flexion of the neck - both obstruct the airway
- Head positioned at the edge of the resuscitation table/radiant warmer
Mask Placement (The "2-Point Top Hold" Technique)
- Stand at the baby's head (position yourself at the top of the baby)
- Hold the mask with your non-dominant hand:
- Place the apex of the mask over the bridge of the nose first
- Lower the mask onto the chin
- Use thumb and index finger in a "C" shape on the mask body
- Use middle, ring, and little finger to support the jaw (jaw thrust) - avoid pressing on soft tissues of the neck
- Verify the seal - no visible air leak at the mask edges
Ventilation Technique
- Rate: 40-60 breaths per minute ("breathe-two-three, breathe-two-three...")
- Pressure: Start at 20-25 cmH2O for the first breath; ongoing breaths at 15-20 cmH2O
- Inspiratory time: ~1 second per breath
- Squeeze the bag with 2-3 fingers only (not the whole hand) - neonatal tidal volume is only 5-8 mL/kg
- Signs of effective ventilation:
- Visible chest rise (slight, not exaggerated)
- Improving heart rate (most important sign)
- Improving SpO2 and color
- Breath sounds bilaterally on auscultation
Oxygen Protocol (NRP/WHO)
- Start with room air (21% O2) for term neonates ≥35 weeks
- Add O2 if SpO2 remains below target after 90 seconds:
- 1 min: 60-65%
- 2 min: 65-70%
- 3 min: 70-75%
- 4 min: 75-80%
- 5 min: 80-85%
- 10 min: 85-95%
- For preterm (<35 weeks): start with 21-30% O2 via blender if available
Common Mistakes to Avoid
| Mistake | Consequence | Correction |
|---|---|---|
| Wrong mask size | Poor seal, no ventilation | Choose mask that covers nose+mouth only |
| Neck hyperextension or flexion | Airway obstruction | Neutral sniffing position |
| Squeezing too hard | Pneumothorax, lung injury | Use 2-3 fingers, watch for gentle chest rise |
| Pressing on throat with fingers | Airway compression | Lift jaw, do not compress soft neck tissue |
| Not testing the bag before use | Device failure undetected | Always test against palm before applying to baby |
| Skipping pop-off valve test | Uncontrolled high pressure | Test before every use |
| Using an adult bag | Massively excessive tidal volume | Always use 240 mL neonatal bag |
Quick Reference Card
Bag size: 240 mL (neonatal)
Mask size: 0 = preterm | 1 = term
Rate: 40-60 breaths/min
Pressure: 20-25 cmH2O (initial) / 15-20 cmH2O (ongoing)
Pop-off valve: 35-45 cmH2O
O2 without res: ~40% FiO2
O2 with res: 90-100% FiO2
O2 flow rate: ≥5 L/min
Start O2: Room air first (term) / 21-30% (preterm)
Sources consulted: MSF Neonatal Resuscitation Guidelines, Victorian Newborn Resuscitation Project - Self Inflating Bag Guide, Textbook of Family Medicine 9e (Neonatal Resuscitation Equipment), LITFL BVM Components Reference.
This is a shared conversation. Sign in to Orris to start your own chat.