Explain hypernatremia as a viva question for my medicine viva
Reading File
Finding Sources
Searching the Web
hypernatremia causes classification treatment medicine viva
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from Goldman-Cecil Medicine and Tietz Textbook of Laboratory Medicine. I have everything needed for a thorough viva answer. Let me compose a complete, structured response.
Hypernatremia - Medicine Viva
Q: Define hypernatremia.
Hypernatremia is defined as a plasma sodium concentration >145 mmol/L. It always reflects a state of hypertonicity - an increased concentration of osmotically active solutes throughout all body fluid compartments. Mechanistically, it represents a deficit of total body water relative to total body sodium content.
Key point for viva: Hypernatremia is strictly a hyperosmolar condition. It NEVER occurs with normal or low osmolality.
Q: What is the normal defense against hypernatremia?
Two major protective mechanisms prevent hypernatremia:
- Thirst - even a 1% rise in serum osmolality triggers thirst, prompting water intake
- ADH (vasopressin) - released from the posterior pituitary in response to hyperosmolality; promotes water reabsorption in the collecting duct
Therefore, hypernatremia rarely develops in a conscious, alert patient with a normal thirst mechanism and free access to water. Most cases occur in infants, elderly, ICU patients, or those with altered mental status.
Q: How do you classify the causes of hypernatremia?
Classification is by extracellular fluid (ECF) volume / total body sodium status:
1. Hypovolemic Hypernatremia
Both sodium and water are lost, but water loss > sodium loss (hypotonic fluid loss).
| Source | Examples |
|---|---|
| Extrarenal | Diarrhea, vomiting, skin losses (burns, excessive sweating), respiratory losses |
| Renal | Loop diuretics, osmotic diuresis (DKA, HHNS), polyuric renal failure |
- Urine Na+ <10 mmol/L (extrarenal) or >20 mmol/L (renal)
- Urine osmolality >800 mOsm/kg with extrarenal loss (kidneys conserving appropriately)
2. Euvolemic (Normovolemic) Hypernatremia
Pure water loss without significant change in ECF volume. Key cause: Diabetes Insipidus (DI).
Central DI - decreased/absent ADH secretion:
- Head trauma, pituitary surgery/tumor, granulomatous disease (sarcoidosis, histiocytosis), hypoxia, inherited
Nephrogenic DI - renal resistance to ADH:
- Drugs: lithium (most common), demeclocycline, amphotericin B, vaptans, foscarnet
- Electrolyte disorders: hypercalcemia, hypokalemia
- Sickle cell disease, Sjögren syndrome, amyloidosis
- Mutant vasopressin receptors (rare)
Also: insensible losses (lung, skin) with inadequate replacement; primary hypodipsia (hypothalamic osmoreceptor damage).
3. Hypervolemic Hypernatremia
Net gain of both sodium and water, with sodium gain > water gain. Rare.
- Hypertonic saline infusion
- Sodium bicarbonate infusion (e.g., resuscitation)
- Hyperaldosteronism, Cushing syndrome
- Salt poisoning (accidental or deliberate ingestion of concentrated NaCl)
Q: What are the clinical features?
Symptoms are primarily neurological, due to osmotic shift of water out of brain cells causing cerebral shrinkage:
- Mild: Thirst, irritability, restlessness, tremors, ataxia
- Moderate: Confusion, lethargy, muscle cramps, hyperreflexia, fever, nausea/vomiting
- Severe: Seizures, focal neurological deficits, decreasing consciousness, coma, intracranial hemorrhage (due to tearing of bridging veins as brain shrinks)
Important viva point: Severity of symptoms correlates with rapidity of onset, not just the absolute sodium level. In chronic hypernatremia (slow rise), brain cells generate "idiogenic osmoles" (organic solutes like myoinositol, glutamine) to restore intracellular volume - so symptoms may be absent even at Na >175 mmol/L. In acute hypernatremia, symptoms can appear at Na >160 mmol/L.
Q: What investigations would you order?
- Serum sodium (confirm >145) + serum osmolality (always elevated)
- Urine osmolality - key discriminator:
- <100-200 mOsm/kg → DI (central or nephrogenic)
- >800 mOsm/kg → extrarenal water loss or hypertonic sodium gain
- 300-800 mOsm/kg → osmotic diuresis or partial DI
- Urine sodium (<10 mmol/L extrarenal; >20 mmol/L renal)
- 24-hour urine solute excretion:
- <600 mOsm/day + polyuria → DI
- >800-1000 mOsm/day → osmotic diuresis
- Blood glucose (rule out HHNS/DKA)
- Serum calcium, potassium (nephrogenic DI causes)
To distinguish central vs nephrogenic DI:
- Water deprivation test followed by desmopressin (DDAVP) administration
- Central DI: urine concentrates with DDAVP
- Nephrogenic DI: no response to DDAVP
Q: How do you treat hypernatremia?
Step 1: Address hemodynamic instability
If hypovolemia is severe, give isotonic saline (0.9% NaCl) first to restore tissue perfusion - even though it is not hypotonic, restoring circulation takes priority.
Step 2: Calculate and replace the free water deficit
Formula:
Free Water Deficit = 0.4 × premorbid weight (kg) × [(Na/140) - 1]
For example: 70 kg patient with Na = 168:
= 0.4 × 70 × (168/140 - 1) = 28 × 0.2 = 5.6 L
Step 3: Rate of correction
- Acute hypernatremia (<24-48 hrs): can correct more rapidly
- Chronic/unknown duration: reduce sodium by no more than 0.5-1.0 mmol/L/hour, and no more than 10-12 mmol/L in 24 hours
- Rationale: Rapid correction in chronic hypernatremia risks cerebral edema - because brain cells have accumulated idiogenic osmoles; when free water floods in suddenly, brain cells swell excessively
Step 4: Fluid choice
- Oral tap water (if patient can drink) - best option
- D5W (5% dextrose in water) - provides free water IV
- Half-normal saline (0.45% NaCl) - provides hypotonic solution
- Account for ongoing losses (insensible ~1 L/day + urine losses)
Step 5: Specific causes
- Central DI: Intranasal or IV desmopressin (DDAVP)
- Nephrogenic DI: Remove offending drug; low-sodium diet + thiazide diuretics (paradoxically reduce urine volume); NSAIDs (adjunct)
- Osmotic diuresis/DKA: Insulin + fluid therapy
- Hypervolemic hypernatremia: Hypotonic fluids + loop diuretics; dialysis if severe
Monitoring
- Check serum sodium every 4 hours during correction
- Monitor volume status closely to avoid hypervolemia
Q: What is the prognosis?
Hypernatremia carries a mortality of 40-60% in critically ill/ICU patients, though much of this reflects the severity of underlying illness. Neurological complications (seizures, intracranial hemorrhage) and too-rapid correction (cerebral edema) are major causes of adverse outcomes.
Diagnostic Algorithm
This diagram summarizes the workup approach based on volume status and urine findings:
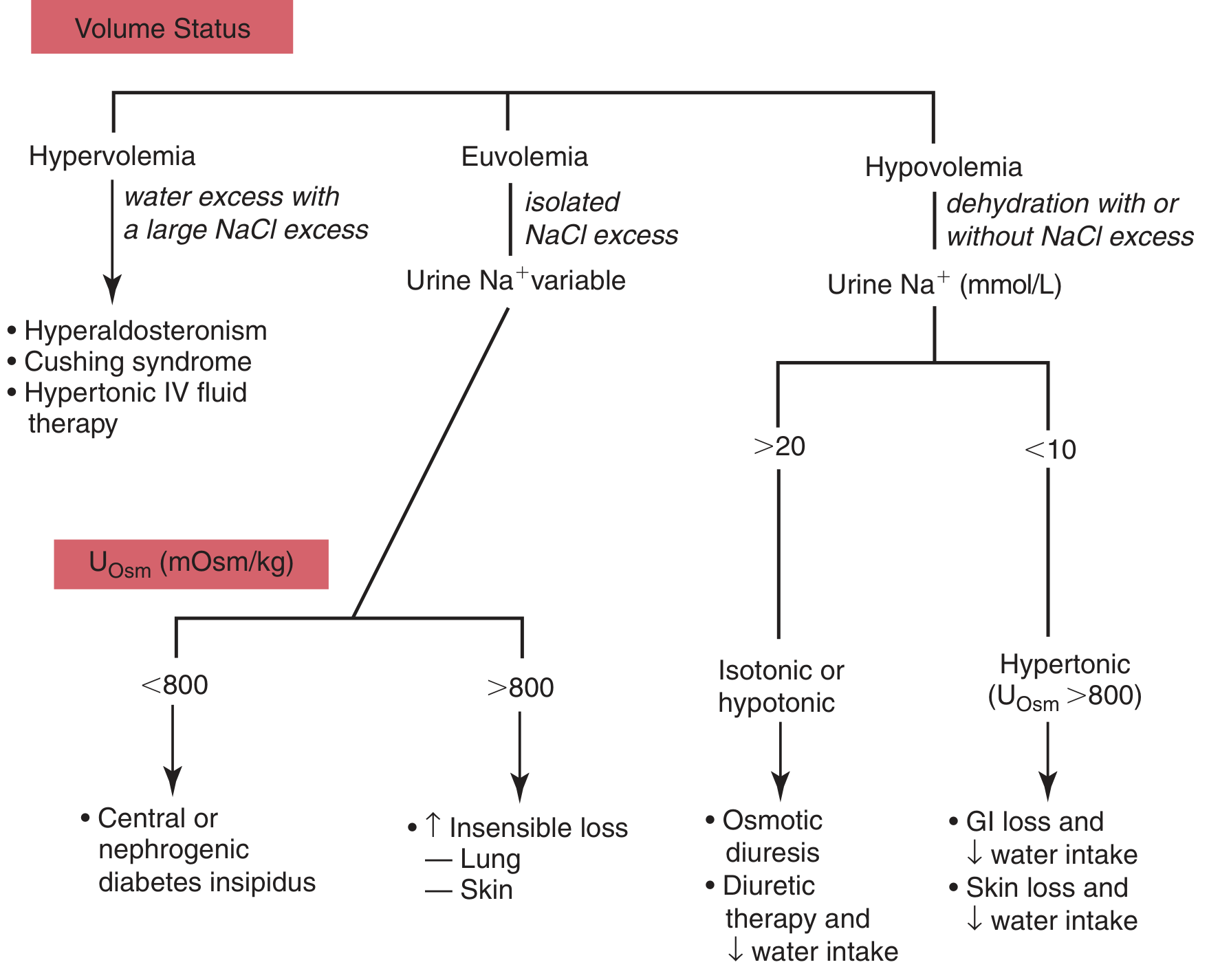
(Tietz Textbook of Laboratory Medicine, 7th Edition, Fig. 50.4)
High-Yield Viva Points Summary
| Point | Answer |
|---|---|
| Definition | Na+ >145 mmol/L |
| Always associated with | Hyperosmolality |
| Most common cause overall | Inadequate water intake / insensible losses |
| Most common renal cause | Diabetes insipidus |
| Most common drug causing nephrogenic DI | Lithium |
| Main symptoms | Neurological (confusion, seizures, coma) |
| Max safe correction rate | 10-12 mmol/L per 24 hours |
| Why not correct too fast? | Cerebral edema from rapid water influx into cells with idiogenic osmoles |
| Formula | Free water deficit = 0.4 × wt × (Na/140 - 1) |
| First fluid in hypovolemia | Isotonic saline (to restore perfusion), then switch to hypotonic |
Sources: Goldman-Cecil Medicine International Edition (p.1204); Tietz Textbook of Laboratory Medicine 7th Ed (p.1941)
You are right but give in easy way answer
Hypernatremia - Simple Viva Answer
"What is hypernatremia?"
Na+ > 145 mEq/L in blood.
Think of it simply: "Too much salt, too little water in the body."
"What causes it?" - Remember 3 types by volume
HYPOVOLEMIC EUVOLEMIC HYPERVOLEMIC
(dehydrated) (normal volume) (overloaded)
Water lost > Pure water loss Too much salt
sodium lost given/taken
Examples: Examples: Examples:
- Diarrhea - Diabetes - Hypertonic saline
- Vomiting Insipidus (DI) - Soy sauce ingestion
- Burns - Fever/sweating - Hyperaldosteronism
- Sweating - Not drinking
- Loop diuretics enough water
Diabetes Insipidus (DI) is the most important cause to know well.
- Central DI = brain not making ADH (head injury, tumor)
- Nephrogenic DI = kidney not responding to ADH (lithium, hypercalcemia)
"Why does the patient get symptoms?"
High sodium outside → water is pulled OUT of brain cells → brain shrinks → symptoms.
Mild: Thirst, restless, irritable
Moderate: Confusion, weakness
Severe: Seizures, coma, death
Exam trick: Acute onset = symptoms at Na ~160. Chronic = symptoms only at Na >175 (because brain makes "idiogenic osmoles" to protect itself over time).
"How do you investigate?"
| Test | What it tells you |
|---|---|
| Serum Na+ | >145 confirms it |
| Serum osmolality | Always HIGH |
| Urine osmolality | The KEY test |
| Urine Na+ | Renal vs extrarenal |
Urine osmolality interpretation:
- <200 → Diabetes Insipidus
- >800 → Extrarenal loss (diarrhea, burns) or sodium overload
- 300-800 → Osmotic diuresis (diabetes, mannitol)
"How do you treat it?"
Step 1 - Shocked patient? Give normal saline first (save life first)
Step 2 - Calculate water deficit:
Water deficit = 0.4 × weight (kg) × [(Na/140) - 1]
Example: 70 kg, Na = 168 → 0.4 × 70 × 0.2 = 5.6 litres
Step 3 - Replace SLOWLY
Do NOT drop Na faster than 10-12 mEq/L per day If you correct too fast → cerebral edema → patient gets worse
Step 4 - Fluid choice:
- Drinking water orally (best)
- D5W (5% dextrose) IV
- Half normal saline (0.45% NaCl)
Step 5 - Treat the cause:
- Central DI → Desmopressin (DDAVP)
- Nephrogenic DI → Stop lithium, thiazide diuretics, low-salt diet
- DKA → Insulin + fluids
One-line memory tricks
| To remember | Trick |
|---|---|
| Definition | Na > 145 |
| Main symptom | Brain shrinks → neuro symptoms |
| Key urine test | Osmolality tells you why |
| Correction rate | Max 10 mEq/day (slow = safe) |
| Too fast correction risk | Cerebral edema |
| Central DI treatment | DDAVP |
| Drug causing nephrogenic DI | Lithium |
Diagnostic Algorithm
Start with volume status → then check urine → diagnosis follows naturally.
That's the entire topic in a logical, exam-friendly flow. In a viva, always start with the definition, classify by volume, explain symptoms by mechanism, then investigations, then treatment - examiners love that structure.
This is a shared conversation. Sign in to Orris to start your own chat.