classify different type of swelling and managy
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed for a comprehensive answer. Let me compile it.
Classification of Swelling (Edema) and Management
Pathophysiology
Swelling (edema) forms when fluid accumulates in the interstitial space due to an imbalance of the Starling forces. There are five fundamental mechanisms:
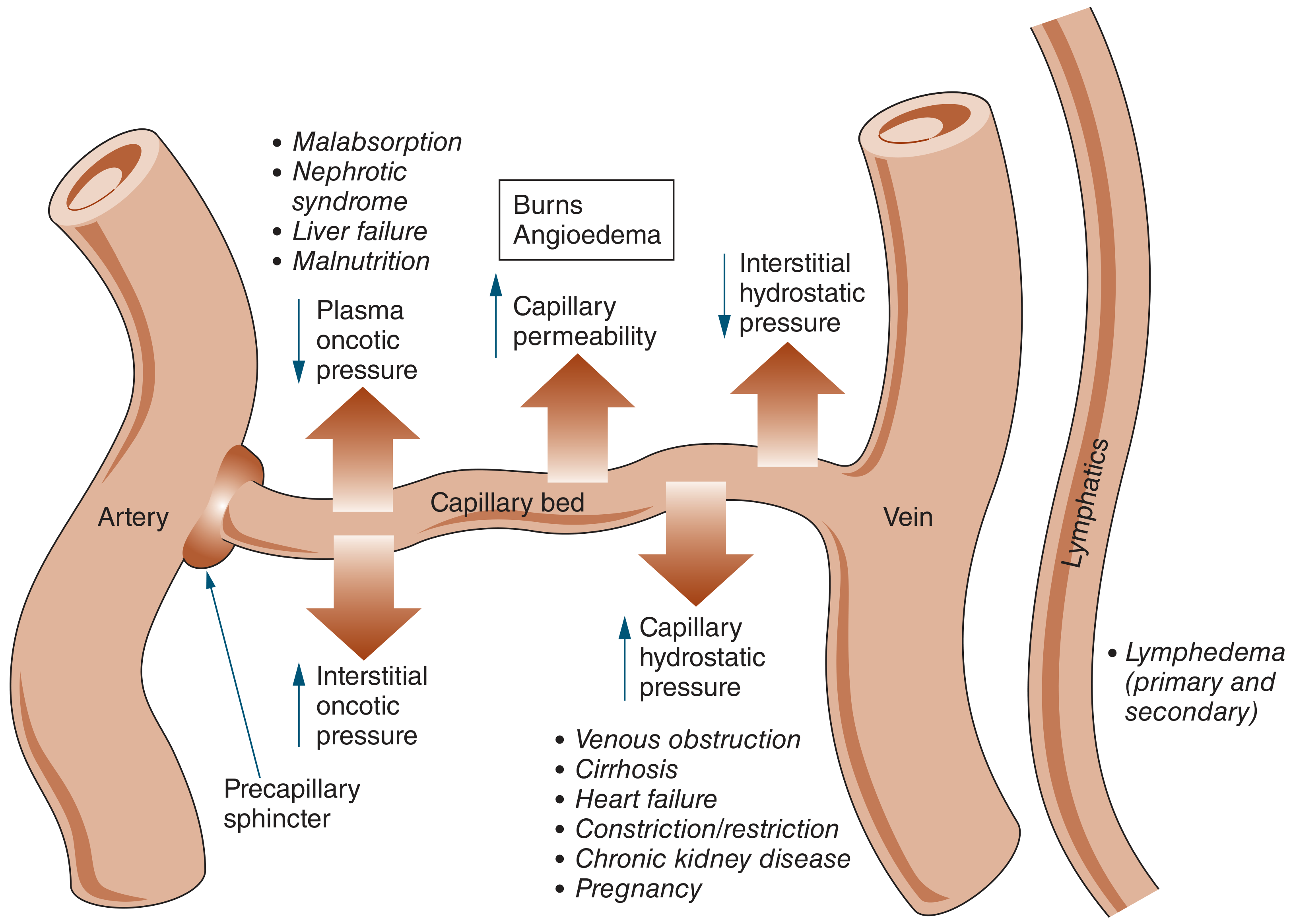
| Mechanism | Examples |
|---|---|
| Increased capillary hydrostatic pressure | Heart failure, cirrhosis, venous obstruction, pregnancy |
| Decreased plasma oncotic pressure | Nephrotic syndrome, malnutrition, liver failure, malabsorption |
| Increased capillary permeability | Burns, angioedema, inflammation, sepsis |
| Lymphatic obstruction | Primary/secondary lymphedema |
| Increased interstitial oncotic pressure | Myxedema (hypothyroidism) |
Classification by Distribution
A. Generalized (Bilateral / Systemic) Edema
Pitting edema - finger pressure leaves an indentation
1. Cardiovascular
- Heart failure with reduced or preserved ejection fraction
- Constrictive pericarditis
- Pulmonary hypertension
Clue: Dyspnea, orthopnea, elevated JVP, S3 gallop
2. Hepatic
- Cirrhosis (portal hypertension + hypoalbuminemia)
- Associated ascites
Clue: Jaundice, spider angiomata, palmar erythema, caput medusae
3. Renal
- Nephrotic syndrome (massive proteinuria, hypoalbuminemia)
- Chronic kidney disease (sodium retention)
Clue: Periorbital edema (especially in nephrotic syndrome), frothy urine
4. Nutritional / Hypoproteinemic
- Malnutrition, malabsorption syndromes
5. Drug-induced
- Calcium channel blockers (especially dihydropyridines, e.g., amlodipine)
- Direct vasodilators (hydralazine, minoxidil)
- NSAIDs
- Thiazolidinediones (pioglitazone)
- Estrogens, corticosteroids, testosterone
6. Endocrine
- Myxedema (hypothyroidism): non-pitting edema due to glycosaminoglycan accumulation
B. Bilateral Leg Edema (Venous/Lymphatic)
Venous Insufficiency (Chronic)
- Varicosities, lipodermatosclerosis in the "gaiter" region, skin ulceration
- Late: hemosiderin staining, eczema
Deep Vein Thrombosis (Bilateral)
- Bilateral pelvic or retroperitoneal lymphadenopathy, pregnancy
C. Unilateral Limb Edema
| Cause | Key Features |
|---|---|
| Unilateral DVT | Sudden onset, calf pain, warmth, Homan's sign |
| May-Thurner syndrome | Left leg; compression of left iliac vein by right iliac artery |
| Secondary lymphedema | Post-mastectomy arm, after radiation, malignancy |
| Cellulitis/erysipelas | Erythema, warmth, fever |
| Baker cyst (leg) | Posterior knee swelling, popliteal fullness |
D. Lymphedema (Primary vs. Secondary)
Classification by Allen's system (from Schwartz's Surgery, 11th Ed.):
Primary Lymphedema (lymphatic hypoplasia/dysfunction)
| Type | Onset | Features |
|---|---|---|
| Congenital (Milroy disease) | Before age 2 | Can involve limbs, genitalia, face; associated with Turner, Klippel-Trenaunay |
| Lymphedema praecox | Puberty to ~35 yrs | Most common (94%); female predominance 10:1; involves foot and calf |
| Lymphedema tarda | After age 35 | Uncommon (<10%) |
Associated syndromes: Yellow nail syndrome, Turner, Noonan, distichiasis-lymphedema, Emberger syndrome
Secondary Lymphedema (acquired obstruction)
- Post-mastectomy (most common cause in the USA)
- Radiation therapy
- Malignant occlusion
- Filariasis - Wuchereria bancrofti (most common worldwide cause)
- Podoconiosis (volcanic soil exposure)
- Recurrent lymphangitis/cellulitis
- Granulomatous disease (TB, sarcoid)
Clinical features: Non-pitting edema, heaviness, positive Stemmer sign (cannot pinch dorsal skin at base of 2nd toe), squared-off toes, dorsal foot involvement, skin hyperkeratosis in advanced disease, fluid weeping from lymph-filled vesicles.
E. Localized Edema
- Burns
- Angioedema / urticaria
- Trauma/hematoma
- Cellulitis, erysipelas
- Abscess
- Insect bites
- Allergic reactions
- Lipedema (bilateral, symmetric, spares the feet - does NOT respond to compression)
Distinguishing Pitting vs. Non-Pitting Edema
| Feature | Pitting | Non-Pitting |
|---|---|---|
| Finger pressure | Leaves pit | No pit |
| Common causes | Cardiac, renal, venous, hepatic, drug-induced | Lymphedema, myxedema, lipedema |
| Protein content | Low-protein transudate | High-protein exudate |
Management
1. Management of Systemic Causes (Treat the Underlying Disease)
| Cause | Key Treatment |
|---|---|
| Heart failure | ACE inhibitors/ARBs, beta-blockers, diuretics (furosemide), aldosterone antagonists, fluid restriction |
| Cirrhosis/ascites | Salt restriction, spironolactone ± furosemide, avoid NSAIDs, paracentesis for refractory ascites |
| Nephrotic syndrome | Treat underlying glomerulopathy, diuretics, ACE inhibitors (reduce proteinuria) |
| Hypothyroidism (myxedema) | Levothyroxine replacement |
| Drug-induced | Discontinue or switch offending drug |
| DVT | Anticoagulation (LMWH/DOAC), compression stockings |
2. Conservative Management of Lymphedema
(Current Surgical Therapy 14e; Schwartz's Surgery 11th Ed.)
- Compression garments - 20-60 mmHg graded compression stockings; worn during waking hours; replace every 6 months. Reduces limb volume by ~30-45%.
- Limb elevation - adjunct therapy, especially overnight
- Intermittent pneumatic compression (IPC) - 4-6 hours/day at home; 30-60 mmHg; reduces edema volume temporarily
- Manual lymphatic drainage (Vodder technique) - massage directing lymph proximally; in combination with compression reduces edema and infections per year
- Complete decongestive therapy (CDT) - combination of manual drainage + compression + exercise; most effective multimodal approach
- Skin care and hygiene - prevents cellulitis entry points
- Weight loss and aerobic exercise - proven in large clinical studies to reduce severity
- Diuretics - NOT recommended for isolated lymphedema (can worsen fibrosis and increase interstitial protein); only used when comorbidities require them
- Antibiotic therapy - at earliest signs of cellulitis; drug of choice: penicillin or cephalosporin (Streptococcus/Staphylococcus); for recurrent infections: prophylactic benzathine penicillin 1.2 MU IM monthly, or erythromycin 250 mg BD, or penicillin V 1 g daily
3. Surgical Treatment for Lymphedema
Two main categories:
| Category | Indication | Procedures |
|---|---|---|
| Physiologic (restore lymph flow) | Early disease | Lymphovenous anastomosis (LVA), vascularized lymph node transfer (VLNT) |
| Debulking/Reductive | Late/refractory fibro-fatty disease | Charles procedure, liposuction/suction-assisted protein lipectomy (SAPL) |
New microsurgical techniques (ICG-guided LVA) are increasingly used even in early stages.
Key Differentiating Points in Practice
- Bilateral pitting edema - always look for cardiac, hepatic, or renal cause first
- Unilateral leg edema - rule out DVT first (urgent)
- Non-pitting bilateral lower extremity that spares feet - think lipedema (tenderness, female, family history)
- Non-pitting that involves toes + positive Stemmer sign - lymphedema
- Periorbital + dependent edema + frothy urine - nephrotic syndrome
Sources: Schwartz's Principles of Surgery 11th Ed. | Current Surgical Therapy 14th Ed. | Andrews' Diseases of the Skin | Symptom to Diagnosis 4th Ed.
Swelling means cyst dermoid like
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I now have sufficient content to provide a detailed surgical swelling classification and management answer. Let me compile the full response.
Classification of Surgical Swellings and Management
Surgical swellings (lumps/tumors/cysts) are localized abnormal tissue masses. The traditional surgical approach classifies them first by clinical characteristics, then by tissue of origin.
Part 1: Clinical Classification of Any Swelling
Before deciding the type, every swelling is examined systematically:
| Clinical Feature | What It Tells You |
|---|---|
| Fluctuant | Fluid-filled (cyst, abscess, haematoma) |
| Transilluminant | Clear fluid (cyst, hygroma) |
| Pulsatile + expansile | Aneurysm or arteriovenous connection |
| Reducible | Hernia (returns to cavity on pressure) |
| Compressible | Vascular (haemangioma, lymphangioma) |
| Hard / stony | Malignancy, bone, calcified lesion |
| Tethered to skin | Epithelial origin (sebaceous/epidermoid cyst) |
| Tethered to underlying structure | Deep tissue tumor or lymph node |
| Mobile, slips away | Lipoma |
| Attached to bone | Osteoma, chondroma, exostosis |
| Non-pulsatile, non-compressible | Solid tumor (benign or malignant) |
Part 2: Classification by Tissue of Origin
A. CYSTS (Fluid-filled, epithelial-lined)
1. Epidermoid Cyst (Sebaceous Cyst - misnomer)
Most common cutaneous cyst. Filled with keratin (not sebum - the old name "sebaceous cyst" is incorrect).
- Cause: Plugging of follicular orifice
- Sites: Anywhere on skin (face, scalp, trunk, scrotum)
- Features: Subepidermal nodule 0.5-2 cm, central punctum (pathognomonic), cheesy foul-smelling content when ruptured
- Histology: Lined by keratinizing stratified squamous epithelium
Management:
- If infected: Incision and drainage (I&D) first, wait for inflammation to settle
- Definitive: Complete surgical excision (including entire cyst wall + punctum) after infection resolves - incomplete removal causes recurrence
- Biopsy rarely needed - clinical diagnosis
2. Dermoid Cyst
Arises from ectodermal tissue trapped along embryonic fusion lines. Unlike epidermoid cysts, the wall contains skin appendages (hair follicles, sebaceous glands, sweat glands). Endoderm is never found inside a dermoid.
- Sites (along embryonic closure zones):
- External angular dermoid (lateral end of eyebrow) - most common
- Nasal root / midline forehead
- Floor of mouth
- Midline scalp (frontal to occipital)
- Chest, back, abdomen, perianal area
- Presentation: Usually first year of life (70% identified by age 5)
- Features: Firm, cystic, non-pulsatile, does NOT transilluminate, NOT attached to overlying skin, may tether to underlying bone/tissues. A punctum or tuft of hair may project from a pit.
- Complications: Can connect to CNS or pleura - infection can spread intracranially. Associated with spina bifida, tethered cord.
- Histology: Lined by keratinizing stratified squamous epithelium + skin appendages (hair follicles, sweat/sebaceous glands)
Management:
- Pre-op assessment: CT/MRI mandatory before excision of midline/spinal dermoids to rule out intracranial/intraspinal communication
- Definitive: Total surgical excision (incomplete removal = recurrence)
- If intracranial connection found: Refer to neurosurgery
- Lateral eyebrow dermoids: Can be excised without imaging (low risk of intracranial extension)
3. Thyroglossal Duct Cyst
- Moves upward on swallowing AND on tongue protrusion (pathognomonic)
- Midline neck, most common at hyoid bone level
- Management: Sistrunk's operation (excise cyst + middle 1/3 of hyoid bone + core of tongue base tissue) - reduces recurrence
4. Branchial Cyst (Branchial Cleft Cyst)
- Lateral neck, anterior border of sternocleidomastoid (SCM), upper 1/3
- Contains cholesterol crystals - aspirate looks like "old engine oil"
- Management: Surgical excision of cyst and its tract
5. Ranula
- Floor of mouth, sublingual gland duct obstruction
- Plunging ranula extends through mylohyoid into the neck
- Management: Marsupialization or excision with sublingual gland removal
6. Ganglion
- Diverticular swelling related to a joint or tendon sheath, contains synovial fluid
- Common sites: dorsum of wrist (most common), volar wrist, foot, ankle
- Transilluminates (clear fluid)
- May resolve spontaneously after trauma ruptures it; but recurrence is common
- Management: Reassurance if asymptomatic; aspiration (high recurrence); surgical excision under GA/regional block with bloodless field - neck must be traced and ligated; send for histology if solid tissue found to exclude synovioma
7. Pilonidal Cyst/Sinus
- Natal cleft (posterior midline between buttocks)
- Acquired condition - shed hair drills into skin
- Often presents with abscess/discharge
- Management (acute): I&D; Definitive: Wide excision ± flap reconstruction (Karydakis, Z-plasty, or Limberg flap); removal of coccyx may be needed for large cysts
B. SOLID BENIGN SWELLINGS
1. Lipoma
Benign tumor of mature adipocytes. Most common soft tissue tumor.
- Sites: Anywhere with fat; common in back, neck, axilla, supraclavicular area, arms
- Features: Soft, lobulated, slips away under palpation ("slips sign"), non-tender, overlying skin normal, mobile
- Variants: Simple lipoma, fibrolipoma, angiolipoma (painful), hibernoma, pleomorphic lipoma
- Warning: Deep lipomas in axilla and supraclavicular area can be far more extensive than their surface suggests
Management:
- Small, asymptomatic lipomas: observe
- Excision indicated if: symptomatic, enlarging, cosmetically unacceptable, or doubt about diagnosis
- Technique: Squeeze tissue to make lipoma bulge forward, incise down to it, enucleate along cleavage plane
- Large/multilocular: blunt + sharp dissection; meticulous haemostasis; close dead space or insert suction drain
2. Fibroma / Dermatofibroma
- Firm, skin-colored/brown papule, usually lower legs
- "Dimple sign" - pinching causes central dimpling
- Management: Excision if symptomatic or uncertain diagnosis
3. Neurofibroma
- From nerve sheath; may be solitary or multiple (neurofibromatosis type 1 = von Recklinghausen disease)
- Features: Soft, fusiform, may be tender, positive "buttonhole sign" (finger invaginates through skin into soft center)
- Management: Excision; monitor for malignant transformation (neurofibrosarcoma)
4. Seborrheic Keratosis
- "Stuck-on" warty papule, older adults; NOT pre-malignant
- Management: Cryotherapy, curettage, shave excision if bothersome
C. VASCULAR SWELLINGS
| Type | Features | Management |
|---|---|---|
| Haemangioma (capillary) | Strawberry mark; involutes spontaneously in children | Observe; propranolol for problematic cases |
| Cavernous haemangioma | Deep bluish, compressible | Sclerotherapy/excision |
| AV malformation | Pulsatile, bruit, thrill; expansile | Embolization ± excision |
| Pyogenic granuloma | Rapidly growing vascular nodule; bleeds easily | Excision + curettage |
D. LYMPH NODE SWELLINGS
Classification by cause:
| Category | Examples |
|---|---|
| Reactive / Infective | Viral (EBV, CMV), bacterial (TB, cat-scratch), tonsillitis |
| Inflammatory | Sarcoidosis, SLE |
| Primary malignant | Hodgkin lymphoma, Non-Hodgkin lymphoma |
| Secondary (metastatic) | From head/neck, breast, GI, lung primaries |
Key features to distinguish:
- Soft, tender, mobile = reactive (infection)
- Hard, non-tender, matted (fixed together) = malignancy
- Soft, matted, with collar-stud abscess = TB (fluctuation through deep fascia)
Management: Treat underlying cause; excisional biopsy or FNAC; CT staging for lymphoma
E. MALIGNANT SWELLINGS
Features suggesting malignancy in any swelling:
- Hard, stony consistency
- Irregular margins
- Fixed to underlying structures or overlying skin
- Rapid growth
- Skin changes: ulceration, dimpling, peau d'orange
- Regional lymphadenopathy
- Systemic symptoms: weight loss, night sweats, fatigue
Common malignant swellings:
- Squamous cell carcinoma (SCC) - ulcerated, indurated, everted edges
- Basal cell carcinoma (BCC) - rolled/pearly edges, central ulcer (rodent ulcer)
- Melanoma - pigmented, ABCDE criteria (Asymmetry, Border, Color, Diameter, Evolution)
- Liposarcoma - deep, firm mass resembling lipoma but fixed
- Soft tissue sarcoma - deep to fascia, >5 cm, hard
Part 3: Summary - Key Clinical Differentiators
| Swelling | Skin Attachment | Fluctuant | Transilluminate | Moves with swallowing | Key Sign |
|---|---|---|---|---|---|
| Epidermoid cyst | Yes (punctum) | Yes | No | No | Central punctum |
| Dermoid cyst | No | Yes (firm-cystic) | No | No | Along fusion lines |
| Thyroglossal cyst | No | Yes | No | Yes (+ tongue protrusion) | Sistrunk operation |
| Branchial cyst | No | Yes | Sometimes | No | Lateral neck |
| Lipoma | No | No (soft) | No | No | Slips away |
| Ganglion | No | Yes | Yes | No | Near joint/tendon |
| Lymph node (reactive) | No | No | No | No | Tender, mobile |
| Lymph node (TB) | May be | Yes (collar-stud) | No | No | "Cold abscess" |
Part 4: General Principles of Management
- History and examination - site, size, duration, consistency, attachments, regional nodes, systemic symptoms
- Investigations - USS first-line for most soft tissue lumps; CT/MRI for deep or complex lesions; FNAC/core biopsy if malignancy suspected
- Observe - small, asymptomatic, clearly benign lesions (e.g., small lipoma)
- Aspiration - ganglion (high recurrence); FNAC for diagnosis
- Incision and drainage - infected cysts (epidermoid, pilonidal abscess)
- Excision - gold standard for most cysts; must remove entire wall to prevent recurrence
- Excision biopsy - when histological diagnosis is needed
- Specialized surgery - Sistrunk's for thyroglossal cyst; neurosurgical referral for intracranial dermoid extension
Sources: Fischer's Mastery of Surgery, 8th Ed. | Andrews' Diseases of the Skin | Pye's Surgical Handicraft, 22nd Ed. | Mulholland & Greenfield's Surgery, 7th Ed. | Schwartz's Principles of Surgery, 11th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.