Scorpion bite management
Reading File
Finding Sources
Finding Sources
Searching PubMed
scorpion envenomation management treatment
Searching the Web
scorpion envenomation management clinical guidelines 2024
Reading File
Reading File
Reading File
Searching Images
scorpion sting envenomation clinical findings
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive information from Harrison's 22E (2025), Andrews' Dermatology, and Medical Microbiology to compose a thorough answer.
Scorpion Bite (Sting) Management

Overview
Scorpions are nocturnal arachnids with ~1,000 known species, of which only ~30 pose lethal risk to humans. They hide in crevices, shoes, clothing, and bedding. Stings occur only in self-defense. Medically important species include:
| Species | Region | Venom Mechanism |
|---|---|---|
| Centruroides sculpturatus/exilicauda | USA (Southwest) | Neurotoxin (Na⁺ channel persistent activation) |
| Leiurus quinquestriatus | Middle East / North Africa | Catecholamine storm |
| Androctonus spp. | Mediterranean / North Africa | Catecholamine storm |
| Mesobuthus tamulus | India | Catecholamine storm |
| Tityus serrulatus | Brazil | Catecholamine storm + pancreatitis |
| Hemiscorpius lepturus | Iran | Cytotoxic (hemolysis, necrosis) |
Venom Mechanisms
- Neurotoxic (Centruroides): Keeps voltage-gated Na⁺ channels persistently open → uncontrolled neuronal firing → sympathetic/parasympathetic discharge
- Catecholamine storm (Leiurus, Androctonus, Mesobuthus, Tityus): Massive endogenous catecholamine release → hypertensive crisis, arrhythmias, pulmonary edema, myocardial injury
- Cytotoxic (Hemiscorpius): Direct tissue damage → hemolysis, tissue necrosis, hemoglobinuria, AKI
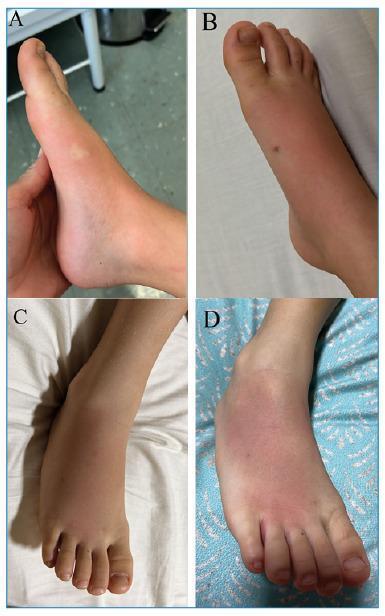
Clinical Features
Local (most stings)
- Immediate sharp pain, paresthesia, hyperesthesia
- Variable edema, ecchymosis, burning sensation
- Positive tap test (Centruroides): pain/paresthesia accentuated by tapping the site
- Typically resolves within a few hours; skin does not slough (except cytotoxic species)
Systemic (dangerous species / severe envenomation)
Neuromotor (Centruroides):
- Restlessness, profuse salivation, lacrimation, rhinorrhea
- Blurred vision, abnormal eye movements, slurred speech
- Muscle twitching/jerking (can mimic seizures)
- Cranial nerve dysfunction, hypersalivation
- Tachycardia, arrhythmias, hypertension, hyperthermia, rhabdomyolysis, acidosis
- Peak severity ~5 hours; symptoms subside in 1–2 days (pain/paresthesia may last weeks)
- Fatal respiratory arrest — highest risk in young children and elderly
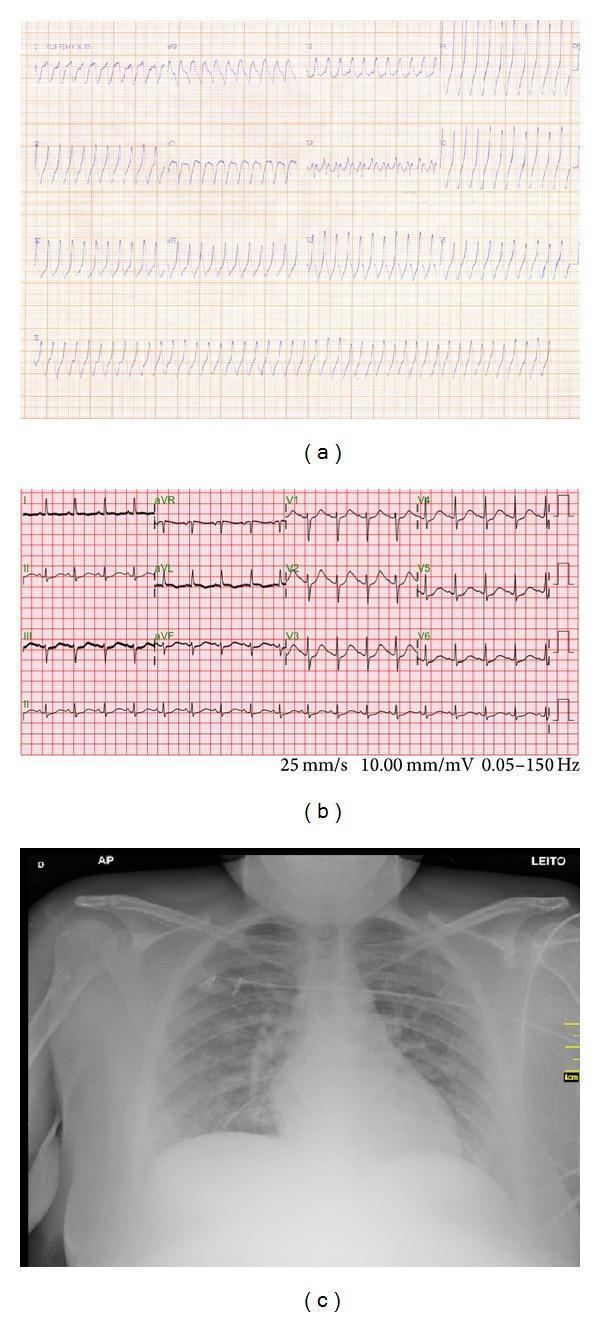
Cardiovascular (Leiurus, Androctonus, Mesobuthus, Tityus):
- Hypertensive crises, arrhythmias, pulmonary edema, myocardial damage
- Tityus trinitatis → acute pancreatitis
- Parabuthus/Buthotus (South Africa) → CNS toxicity
Cytotoxic (Hemiscorpius):
- Relatively asymptomatic at first
- 24h+: pain, hemolysis, tissue necrosis, hemoglobinuria → AKI
Management
1. First Aid / Pre-hospital
- Move patient away from the scorpion (do not handle it)
- Cold packs to the sting site — reduce venom absorption and swelling (hot packs are contraindicated — cause vasodilation and accelerate systemic spread)
- Pressure dressing over the site
- Keep the patient calm
- Assess airway and vital signs
- Do not attempt to suck out venom or apply tourniquets
2. Risk Stratification
| Grade | Features | Management |
|---|---|---|
| Mild (local only) | Pain, paresthesia, positive tap test, no systemic signs | Home management; return precautions |
| Moderate | Mild systemic: tachycardia, HTN, sweating | ED observation, IV access, monitoring |
| Severe | Cranial nerve/neuromuscular dysfunction, cardiovascular collapse, respiratory failure | ICU, antivenom |
3. Symptomatic/Supportive Treatment
| Problem | Treatment |
|---|---|
| Mild local pain | Ice packs, oral analgesics, oral antihistamines |
| Agitation / involuntary movements | IV midazolam (continuous infusion) |
| Hypertension / pulmonary edema | Nifedipine, nitroprusside, hydralazine, or prazosin |
| Bradydysrhythmia | Atropine |
| Secretion management | Supportive, consider glycopyrrolate |
| Sedation with opiates/benzodiazepines | Monitor closely for respiratory compromise |
| Pain relief | Analgesics; avoid opiates where possible (may increase toxicity) |
⚠️ Contraindicated: Steroids, antihistamines, calcium channel blockers, and diuretics should be avoided for cardiac complications — they can worsen outcomes through negative cardiac effects.
4. Antivenom
- Indicated for: severe envenomation with cranial nerve/neuromuscular dysfunction, cardiovascular compromise, respiratory failure
- FDA-approved (USA): Equine-derived Centruroides sculpturatus IgG F(ab')₂ antivenom (Anascorp®)
- IV administration rapidly reverses cranial nerve dysfunction and muscular symptoms
- Other regions: Species-specific antivenoms exist for Leiurus, Androctonus, Tityus, Mesobuthus — follow local availability and national guidelines
- More effective when administered early after envenomation
- Watch for serum sickness (~1–2 weeks post-administration): treat with antihistamines, analgesics ± oral steroids
5. Pediatric Considerations
- Children are at highest risk for severe/fatal envenomation
- Even moderate symptoms in children should be treated as medical emergencies
- Antivenom threshold is lower in children
6. Tetanus Prophylaxis
- Ensure tetanus immunization status is current for all sting patients
What NOT to Do
- ❌ Hot packs (increase absorption)
- ❌ Opioid analgesics unless carefully monitored (increase toxicity)
- ❌ Calcium channel blockers, steroids, antihistamines, or diuretics for cardiac management
- ❌ Excision or suction of sting site
Disposition
| Finding | Disposition |
|---|---|
| Local pain only, nonlethal species confirmed | Discharge with return precautions |
| Systemic symptoms, uncertain species | Emergency department for observation |
| Neuromuscular dysfunction, cardiovascular compromise | ICU admission, antivenom, monitoring |
Prevention
- Shake out shoes, clothing, and bedding in endemic areas
- Use a flashlight at night
- Clear debris around dwellings
- Wear protective footwear outdoors at night
Sources: Harrison's Principles of Internal Medicine 22E (2025), p. 3778–3779; Andrews' Diseases of the Skin; Medical Microbiology 9e
This is a shared conversation. Sign in to Orris to start your own chat.