Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive information from the textbooks to answer all 6 questions thoroughly. Let me compile the full answer.
Case 1: Cervical Cancer - Complete Analysis
1. Most Likely Diagnosis
Invasive Squamous Cell Carcinoma of the Cervix - confirmed by cervical biopsy in this case.
The clinical picture is classic: a multiparous 38-year-old woman with post-coital bleeding (the hallmark symptom of cervical cancer), foul-smelling vaginal discharge, an erythematous cervix with an ulcerative lesion, HSIL on Pap smear, acetowhite lesion on colposcopy, and biopsy-confirmed invasive squamous cell carcinoma.
"Invasive squamous cell carcinoma is the most common variety of invasive cancer in the cervix." - Berek & Novak's Gynecology
2. Risk Factors
The following are established risk factors for cervical cancer, directly tied to HPV exposure and other cofactors:
| Category | Specific Factors |
|---|---|
| Sexual behavior | Early first intercourse (<16 years), multiple sexual partners, partner with multiple partners |
| HPV-related | Persistent high-risk HPV infection |
| Lifestyle | Cigarette smoking (acts as a co-carcinogen) |
| Sociodemographic | Low socioeconomic status, high parity, non-white race |
| Immunological | Chronic immunosuppression (e.g., HIV infection) |
| Screening failure | Never undergone cervical cancer screening (as in this patient) - ~30% of cervical cancers occur in women who have never had a Pap test |
| Other | In utero diethylstilbestrol (DES) exposure; prior treatment for high-grade lesions |
This patient's key risk factors are: high parity (multiparous), no prior screening, and presumed HPV exposure.
"There are numerous risk factors for cervical cancer: young age at first intercourse (younger than 16 years), multiple sexual partners, cigarette smoking, race, high parity, low socioeconomic status, and chronic immune suppression." - Berek & Novak's Gynecology
3. Virus Associated with This Disease
Human Papillomavirus (HPV) - specifically the high-risk strains, is the causative agent.
Key facts:
- HPV 16 and HPV 18 account for approximately 70% of all cases of cervical intraepithelial neoplasia (CIN) and cervical carcinoma
- HPV is a DNA virus; its oncogenic activity depends on two viral proteins: E6 (binds and degrades tumor suppressor p53; upregulates telomerase) and E7 (binds and inactivates the RB protein, promoting uncontrolled cell cycle progression)
- Low-risk HPV types (6, 11) cause condylomas but rarely progress to carcinoma
- High-risk HPV integrates into the host genome, disrupting the regulatory gene for E6/E7, leading to their overexpression and genomic instability
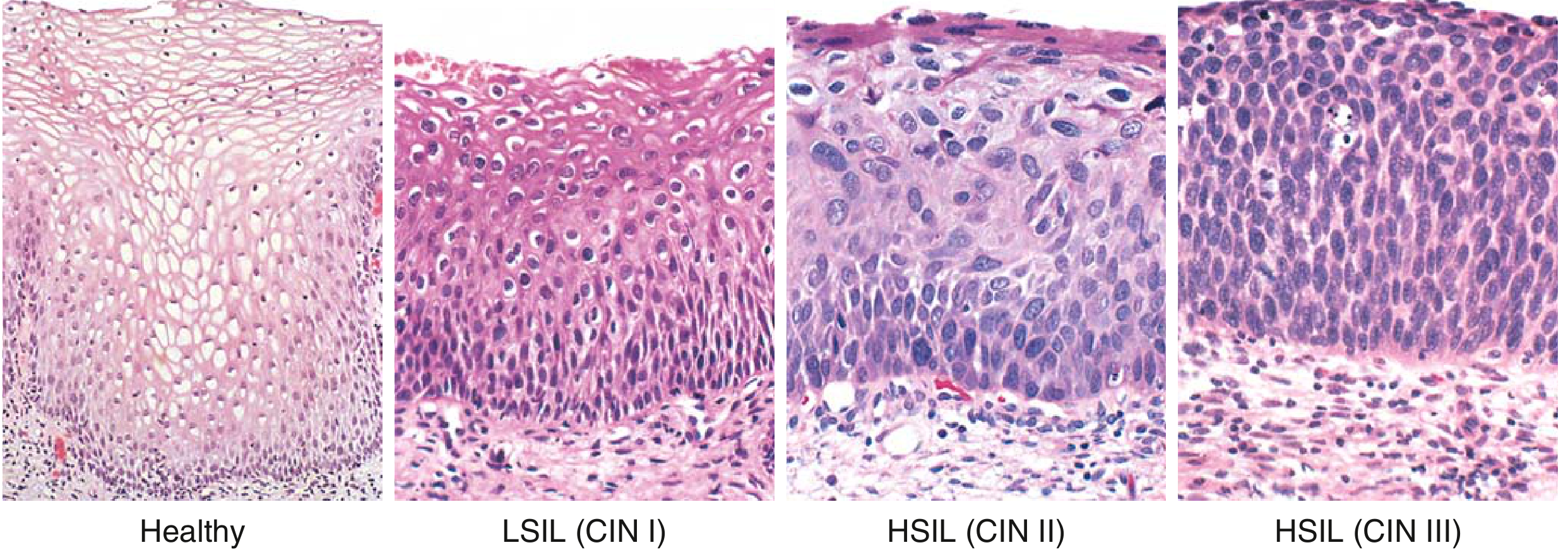
Spectrum of SIL from healthy to HSIL (CIN III) - Robbins & Kumar Basic Pathology
"Two high-risk HPV viruses, types 16 and 18, account for approximately 70% of cases of CIN and cervical carcinoma." - Robbins & Kumar Basic Pathology
4. FIGO Staging (2018 System)
The 2018 FIGO staging updated the 2008 system to incorporate imaging and pathologic findings:
| Stage | Description |
|---|---|
| I | Carcinoma strictly confined to the cervix |
| IA | Microscopic only; maximum depth of invasion <5 mm |
| IA1 | Stromal invasion <3 mm depth |
| IA2 | Stromal invasion ≥3 mm and <5 mm |
| IB | Invasive carcinoma ≥5 mm depth; limited to cervix |
| IB1 | ≥5 mm depth AND <2 cm greatest dimension |
| IB2 | ≥2 cm and <4 cm greatest dimension |
| IB3 | ≥4 cm greatest dimension |
| II | Invades beyond uterus but not to lower 1/3 vagina or pelvic wall |
| IIA | Upper 2/3 vagina involved; no parametrial involvement |
| IIA1 | Tumor <4 cm |
| IIA2 | Tumor ≥4 cm |
| IIB | Parametrial involvement |
| III | Extends to lower 1/3 vagina and/or pelvic wall, or hydronephrosis, or lymph nodes |
| IIIA | Lower 1/3 vagina involvement |
| IIIB | Pelvic wall and/or hydronephrosis/non-functioning kidney |
| IIIC | Pelvic (IIIC1) or para-aortic (IIIC2) lymph node involvement |
| IV | Extension beyond true pelvis or bladder/rectal mucosa involvement |
| IVA | Bladder or rectal mucosa involvement |
| IVB | Distant metastases |
In this case: The patient has no parametrial involvement and a small ulcerative lesion - most likely Stage IB1 or IB2 (clinically visible lesion confined to cervix). Final staging requires imaging and measurement.
Notable 2018 updates: horizontal spread no longer used for stage IA; Stage IB now has 3 substages; Stage IIIC added for lymph node metastasis.
5. Management of Early-Stage Disease
Early-stage cervical cancer (Stages I to IIA) has two equally effective primary treatment options:
A. Radical Surgery (Preferred for younger patients)
- Radical (Wertheim's) hysterectomy with bilateral pelvic lymph node dissection
- Advantages: preserves ovarian function in premenopausal women, avoids radiation side effects, allows accurate pathological staging, enables examination of specimens
- For very early disease (Stage IA1 without LVSI): simple hysterectomy or even cone biopsy if fertility preservation is desired
- For Stage IA2-IB2: radical hysterectomy + pelvic lymphadenectomy
B. Radiation Therapy
- External beam radiotherapy (EBRT) to the pelvis + intracavitary brachytherapy
- Used when surgery is contraindicated or patient prefers it
- Concurrent cisplatin-based chemotherapy (chemoradiation) is the standard when radiation is used, as it acts as a radiosensitizer
C. Advanced Disease (Stages IIB-IV)
- Concurrent chemoradiation (cisplatin-based) + brachytherapy is the mainstay
- Neoadjuvant chemotherapy followed by surgery is also used in some settings
"Early-stage disease (stages I to IIA) can be treated with either radical surgery or radiation therapy. Advanced stage disease (stages IIB to IV) is best treated with chemoradiation, including brachytherapy." - Berek & Novak's Gynecology
6. Prevention
Prevention operates at two levels:
Primary Prevention (Reducing HPV exposure/infection)
-
HPV Vaccination:
- Recommended for boys and girls at 11-12 years (before sexual debut); catch-up vaccination up to age 26 (and selectively up to 45)
- Quadrivalent vaccine (types 6, 11, 16, 18) and the 9-valent vaccine (covers 9 HPV types including 31, 33, 45, 52, 58) - very effective in preventing HPV infections
- Vaccination of males is critical due to their role in spreading HPV and the toll of HPV-related anal/oropharyngeal cancers in men
- Note: vaccination does not replace screening in already-exposed women
-
Behavioral measures: Delaying age of first intercourse, limiting number of sexual partners, condom use, smoking cessation
Secondary Prevention (Early detection via screening)
- Pap smear (cervical cytology): Detects precancerous SIL/CIN before invasion
- HPV DNA testing: Highly sensitive; particularly useful in women ≥30 years (combined with Pap as co-testing)
- Colposcopy + biopsy: For abnormal screening results
- Treatment of precancerous lesions (CIN): LEEP (Loop Electrosurgical Excision Procedure), cryotherapy, cold knife conization - prevents progression to invasive cancer
"Another important aspect of cervical cancer prevention is vaccination against high-risk HPV types... The 9-valent vaccine is very effective in preventing HPV infections and is expected to greatly lower the frequency of genital warts and cervical cancers." - Robbins & Kumar Basic Pathology
This patient's case illustrates the critical importance of screening - she had never undergone cervical cancer screening, which allowed an invasive lesion to develop undetected.
Sources:
- Berek & Novak's Gynecology, Chapter 38 - Cervical Cancer
- Robbins & Kumar Basic Pathology, Chapter 17 - Cervical Neoplasia
- Goldman-Cecil Medicine, Chapter on Cervical Cancer
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have all the information needed. Let me compile the comprehensive answer.
Clinical Scenario 5: Endometrial Cancer - Complete Analysis
Patient Summary: 62-year-old postmenopausal woman (menopause 12 years ago), nulliparous, on tamoxifen for breast cancer x 6 years, presenting with intermittent vaginal bleeding x 3 months, watery vaginal discharge, lower abdominal discomfort. TVUS: endometrial thickness 16 mm with irregular lining. Biopsy: endometrioid adenocarcinoma. MRI: tumor confined to uterus, <50% myometrial invasion, no lymph nodes.
1. Most Likely Diagnosis
Endometrial Carcinoma - Type 1 (Endometrioid Adenocarcinoma)
This is confirmed by the endometrial biopsy. Based on the MRI findings (tumor confined to uterus, <50% myometrial invasion, no lymph node enlargement), this is FIGO Stage IA endometrial cancer.
Endometrioid adenocarcinoma is the most common subtype (~80-85% of all endometrial cancers). It is a Type 1 (estrogen-dependent) tumor with a favorable prognosis when confined to the uterus.
2. Risk Factors Present in This Patient
This patient has multiple high-risk factors, all present simultaneously:
| Risk Factor | Relative Risk | Present in Patient? |
|---|---|---|
| Nulliparity | 2-3x | ✅ Yes |
| Tamoxifen therapy | 2-3x | ✅ Yes (6 years for breast cancer) |
| Late menopause | 2.4x | ✅ (menopause at ~50 years) |
| Age (postmenopausal) | Increasing | ✅ Age 62 |
| Obesity (if present) | 3-10x | Possible (not stated) |
| Unopposed estrogen | 4-8x | Via tamoxifen partial agonism |
Why tamoxifen increases risk: Tamoxifen is a selective estrogen receptor modulator (SERM). While it acts as an estrogen antagonist in breast tissue, it exerts partial estrogen agonist activity on the endometrium, stimulating endometrial proliferation. This increases endometrial cancer risk by 2-3 fold. The risk is related to duration of use.
Why nulliparity increases risk: Nulliparous women are exposed to more cumulative unopposed estrogen cycles (no progesterone dominance during pregnancy), leading to endometrial proliferation over time.
"The use of tamoxifen for treatment of breast cancer is associated with a two- to threefold increased risk for the development of endometrial cancer." - Berek & Novak's Gynecology
3. Why Postmenopausal Bleeding is an Important Warning Symptom
Postmenopausal bleeding (PMB) is the cardinal symptom of endometrial cancer and must always be investigated urgently because:
- After menopause, the endometrium becomes atrophic and should produce no bleeding
- Any vaginal bleeding after 12 months of amenorrhea is abnormal by definition
- PMB indicates underlying pathology - in approximately 10% of cases, the cause is endometrial carcinoma
- Other causes include atrophic vaginitis, endometrial polyps, and hyperplasia - but malignancy must be excluded first
- Early detection of endometrial cancer (when still confined to the uterus) is associated with excellent survival rates (>90% 5-year survival for stage I)
- Delayed investigation allows progression to higher stages, reducing cure rates substantially
"Abnormal uterine bleeding is a warning sign for endometrial cancer if it develops in postmenopausal women." - Goldman-Cecil Medicine
This patient's 3-month history of intermittent PMB combined with watery vaginal discharge further heightens concern - watery/blood-tinged discharge is a recognized presentation of endometrial carcinoma.
4. Role of Transvaginal Ultrasonography (TVUS) in Evaluating PMB
TVUS is the first-line imaging investigation for postmenopausal bleeding because it is:
- Non-invasive, widely available, and inexpensive
- Highly sensitive for detecting endometrial pathology
Key diagnostic threshold:
- Endometrial thickness ≤4-5 mm in a postmenopausal woman = low risk of malignancy (endometrial cancer extremely unlikely; negative predictive value ~99%)
- Endometrial thickness >4-5 mm = requires further investigation (biopsy)
- This patient's endometrial thickness of 16 mm is markedly abnormal (more than 3x the threshold), indicating high suspicion for endometrial pathology
What TVUS can detect:
- Endometrial thickness (screening parameter)
- Irregular or heterogeneous endometrial lining (as in this case)
- Endometrial polyps, submucosal fibroids
- Focal vs. diffuse endometrial lesions
- Myometrial invasion depth (though MRI is more accurate for this)
"In a postmenopausal woman, an endometrial stripe of less than 5 mm on transvaginal ultrasound has a very high negative predictive value for endometrial cancer." - Swanson's Family Medicine Review
Important: TVUS is a triage tool, not a definitive diagnostic tool. A thick or irregular endometrium on TVUS mandates tissue sampling (biopsy).
5. Gold Standard Investigation for Confirming the Diagnosis
The gold standard for confirming endometrial cancer is endometrial biopsy with histopathological examination - as performed in this patient, which showed endometrioid adenocarcinoma.
Methods of tissue sampling (in order of invasiveness):
| Method | Description | Notes |
|---|---|---|
| Pipelle endometrial biopsy | Office-based suction curettage | First-line; ~90% sensitivity for endometrial cancer |
| Dilatation & Curettage (D&C) | Under anesthesia | Used when office biopsy fails or is inadequate |
| Hysteroscopy + directed biopsy | Direct visualization + targeted sampling | Best for focal lesions; gold standard for accuracy |
Hysteroscopy + directed biopsy is considered the most accurate method as it allows direct visualization of the endometrial cavity and targeted sampling of suspicious areas, avoiding sampling errors from blind techniques.
In this case, the endometrial biopsy confirmed endometrioid adenocarcinoma, and MRI pelvis was used for staging, showing:
- Tumor confined to uterus (Stage I)
- <50% myometrial invasion (Stage IA)
- No lymph node involvement
6. Standard Treatment for This Stage (Stage IA Endometrial Cancer)
Based on MRI showing tumor confined to uterus with <50% myometrial invasion = FIGO Stage IA endometrioid adenocarcinoma - this is low-risk, early-stage disease.
Primary Treatment: Surgery
Total Hysterectomy + Bilateral Salpingo-oophorectomy (TAH-BSO) is the cornerstone of treatment.
- The standard approach is Total Abdominal Hysterectomy (or laparoscopic/robotic-assisted) + Bilateral Salpingo-Oophorectomy
- Ovaries are removed because: (a) the risk of ovarian metastasis, (b) ovaries are a source of ongoing estrogen, (c) Lynch syndrome screening considerations
- Peritoneal washings are taken at the time of surgery
Lymph Node Assessment
For Stage IA, grade 1-2 disease (low risk):
- Systematic lymphadenectomy may be omitted - GOG33 data shows near-zero lymph node metastasis risk in superficially invasive, low-grade disease
- Sentinel lymph node (SLN) biopsy is increasingly used as a middle ground - it provides nodal staging information with less morbidity than full lymphadenectomy
Adjuvant Treatment (for Stage IA)
- Stage IA, grade 1-2, no lymphovascular invasion (LVSI): Surgery alone - no adjuvant therapy needed
- Stage IA, grade 3 or LVSI positive: Consider vaginal brachytherapy to reduce vaginal vault recurrence
- Chemotherapy (carboplatin + paclitaxel) is reserved for high-risk histologies (serous, clear cell) or advanced stages
Summary for this patient:
This patient (Stage IA, endometrioid - presumed low grade) should receive:
- TAH + BSO (via laparoscopy/robotic if available - equivalent oncologic outcomes, faster recovery)
- Sentinel lymph node mapping at time of surgery
- Likely no adjuvant radiotherapy if final pathology confirms Stage IA, grade 1-2, no LVSI
- Discontinue tamoxifen - switching to an aromatase inhibitor for her breast cancer is advisable given the endometrial risk
Prognosis: Stage IA endometrioid adenocarcinoma has a 5-year survival rate of approximately 90-95%.
"Widely accepted management of endometrial cancer consists of hysterectomy, removal of remaining adnexal structures, and appropriate surgical staging in patients considered at risk for extrauterine disease." - Berek & Novak's Gynecology
Sources:
- Berek & Novak's Gynecology, Chapter 37 - Endometrial Cancer (Risk Factors Table 37-1; Staging Table 37-6; Surgical Staging)
- Goldman-Cecil Medicine, Chapter 184 - Endometrial Cancer (Type 1 vs 2 Table; Pathobiology)
- Goodman & Gilman's Pharmacological Basis of Therapeutics - Tamoxifen endometrial effects
- The Washington Manual of Medical Therapeutics - TVUS threshold for postmenopausal bleeding
This is a shared conversation. Sign in to Orris to start your own chat.