V
It looks like your message came through as just "V" - could you share what you'd like help with?
Cardiomegaly
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Here is a complete overview of Cardiomegaly, drawn from Harrison's, Robbins Basic Pathology, Goldman-Cecil Medicine, and Frameworks for Internal Medicine.
Cardiomegaly
Definition
Cardiomegaly refers to an enlarged heart, most commonly defined on a posteroanterior (PA) chest radiograph as a cardiothoracic (CT) ratio ≥ 0.5 - the transverse cardiac diameter divided by the maximum internal thoracic diameter. It is not a disease in itself; it is a sign of an underlying condition.
Important caveat: An enlarged cardiac silhouette on CXR does not automatically mean true cardiomegaly. Pericardial effusion, poor inspiratory effort, and AP projections can all falsely enlarge the cardiac shadow. - Frameworks for Internal Medicine
Types of Cardiac Enlargement
1. Concentric Hypertrophy (Pressure Overload)
- Wall thickness increases disproportionately; chamber size decreases
- Results from chronic pressure overload (e.g., hypertension, aortic stenosis)
- Diastolic dysfunction predominates
- May NOT appear cardiomegalic on CXR early on
2. Eccentric Hypertrophy (Volume Overload)
- Ventricular dilation with wall thinning; chamber size increases
- Results from volume overload (e.g., aortic/mitral regurgitation, dilated cardiomyopathy)
- The heart becomes "big and floppy" - systolic dysfunction predominates
- This manifests as cardiomegaly on CXR - Frameworks for Internal Medicine
Causes of Cardiomegaly
Primary (True Myocardial Enlargement)
| Cause | Mechanism |
|---|---|
| Dilated cardiomyopathy (DCM) | All-chamber dilation, systolic dysfunction |
| Hypertensive heart disease | LV hypertrophy -> eventual dilation |
| Ischemic heart disease / MI | LV remodeling and dilation post-infarct |
| Valvular disease | Volume overload (AR, MR) or pressure overload (AS, MS) |
| Alcoholic cardiomyopathy | Toxic myocardial damage |
| Peripartum cardiomyopathy | Unknown etiology; late gestation to months postpartum |
| Hemochromatosis | Iron overload - myocardial injury |
| Doxorubicin toxicity | Anthracycline-induced DCM |
| Viral myocarditis | Coxsackievirus B, parvovirus B-19, HHV-6 |
| Genetic DCM | Titin, dystrophin, desmin, lamin A/C mutations |
From Goldman-Cecil Medicine: "If an enlarged cardiac silhouette is present, it is generally indicative of a previous MI with LV dilation and cardiac remodeling. Other causes of cardiomegaly include long-standing hypertension, concomitant valvular heart disease, pericardial effusion..."
Pseudo-cardiomegaly (Apparent Enlargement Without True Myocardial Hypertrophy)
- Pericardial effusion - fluid accumulation around the heart
- AP chest radiograph (as opposed to PA) magnifies the cardiac silhouette
- Poor inspiratory effort on CXR
Genetics of Dilated Cardiomyopathy (the most common cause)
DCM is hereditary in 20-50% of cases, with autosomal dominant inheritance predominating. Over 50 mutations are known:
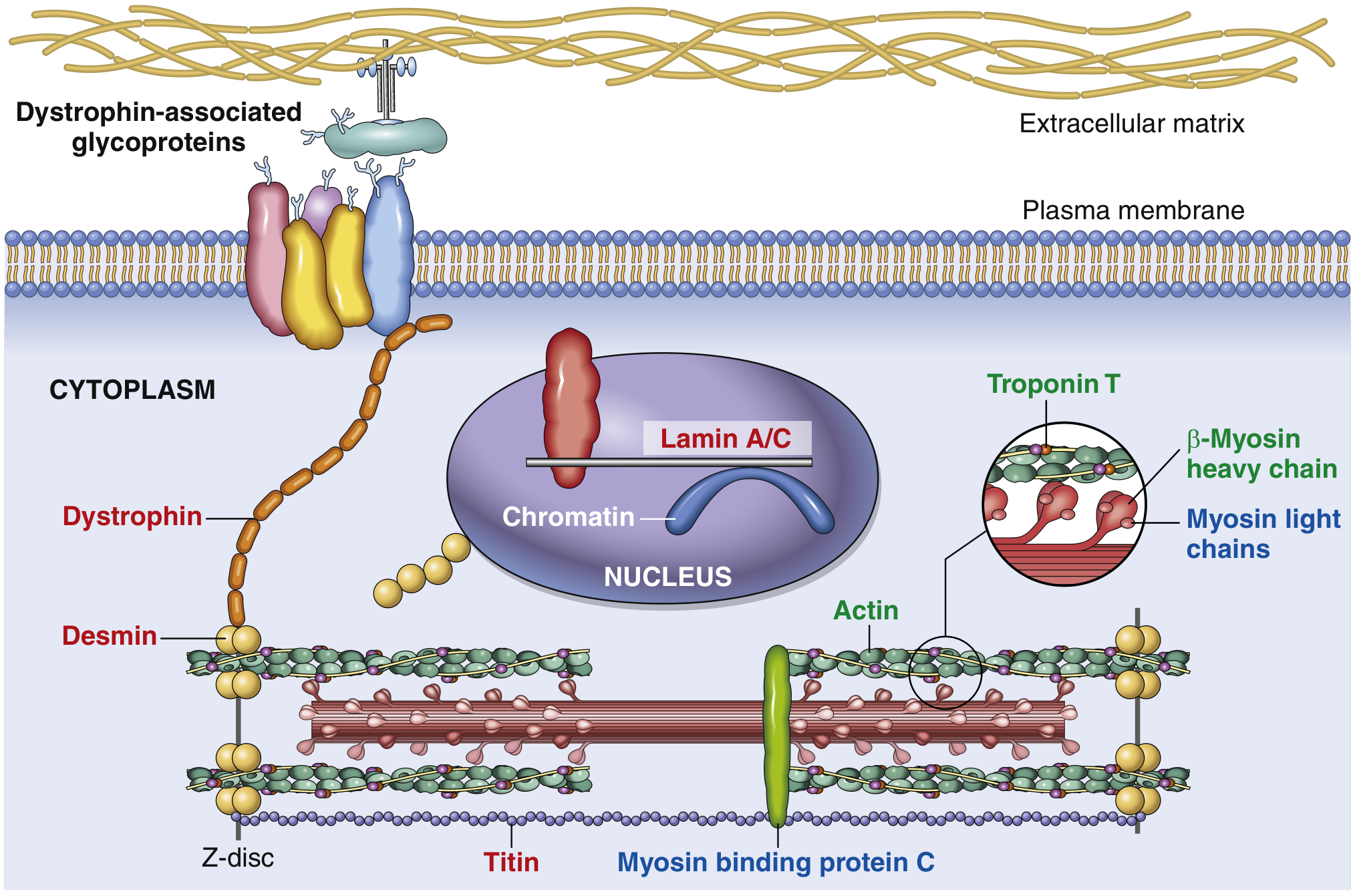
Key proteins mutated in DCM (red labels above):
- Titin - most common (~20% of all DCM); spans the sarcomere
- Dystrophin - X-linked DCM; links cytoskeleton to ECM
- Desmin - intermediate filament protein in cardiac myocytes
- Lamin A/C - nuclear structural protein
- β-myosin heavy chain, Troponin T - sarcomere proteins
- Robbins & Kumar Basic Pathology
Cardiomyopathy Functional Patterns (Differential for Cardiomegaly)
| Pattern | EF | Mechanism | Common Causes |
|---|---|---|---|
| Dilated | <40% | Systolic dysfunction | Genetic, alcohol, peripartum, myocarditis, hemochromatosis, doxorubicin |
| Hypertrophic | 50-80% | Diastolic dysfunction | Genetic, Friedreich ataxia |
| Restrictive | 25-50% | Diastolic dysfunction | Amyloidosis, radiation fibrosis |
- Robbins Basic Pathology, Table 9.5
Clinical Features
- Symptoms: Dyspnea on exertion, orthopnea, PND, fatigue, ankle edema (features of heart failure)
- Signs:
- Displaced apex beat (lateral and downward)
- S3 gallop - highly specific for reduced systolic function (HFrEF)
- Raised JVP, peripheral edema, basal crackles
- Murmurs if valvular etiology
- ECG findings:
- Left atrial abnormality (broad, notched P waves; biphasic P in V1)
- LVH criteria
- Right ventricular hypertrophy signs (tall R in V1, right axis deviation) if right-sided cause
- Tachycardia, LBBB pattern in DCM
- CXR: CT ratio >0.5, pulmonary vascular congestion, Kerley B lines if heart failure present
Diagnosis
| Investigation | Finding |
|---|---|
| CXR | CT ratio ≥ 0.5 |
| Echocardiography | Gold standard - chamber dimensions, wall motion, EF, valvular function |
| ECG | LVH, LAE, arrhythmias |
| Cardiac MRI | Structural detail, myocardial fibrosis (late gadolinium enhancement) |
| BNP / NT-proBNP | Elevated in heart failure |
| Troponin | Elevated in myocarditis or ischemic cause |
| Endomyocardial biopsy | For myocarditis or infiltrative causes |
Treatment
Treatment is directed at the underlying cause, not the cardiomegaly itself:
- HFrEF (systolic dysfunction):
- ACE inhibitors/ARBs or ARNI (sacubitril/valsartan)
- Beta-blockers (carvedilol, metoprolol succinate, bisoprolol)
- Mineralocorticoid receptor antagonists (spironolactone, eplerenone)
- SGLT2 inhibitors (dapagliflozin, empagliflozin)
- Diuretics for fluid overload
- ICD / CRT if EF <35% with LBBB
- Hypertension: Antihypertensive therapy
- Valvular disease: Surgical or transcatheter repair/replacement
- Alcohol: Abstinence - DCM may partially reverse
- Peripartum cardiomyopathy: ~50% recover normal function spontaneously
- Pericardial effusion (pseudo-cardiomegaly): Pericardiocentesis if tamponade
- Hemochromatosis: Phlebotomy, chelation
Key Points to Remember
- Cardiomegaly on CXR = CT ratio >0.5 on a PA film
- It is a sign, not a diagnosis - always seek the underlying cause
- Pericardial effusion can mimic cardiomegaly ("water bottle heart")
- DCM is the classic cause - heart up to 2-3x normal weight, all chambers dilated
- Titin mutations are the single most common genetic cause of DCM (~20%)
- S3 gallop + cardiomegaly strongly suggests HFrEF
- Echo is the key investigation to assess structure and function
Sources: Harrison's Principles of Internal Medicine 22E; Robbins & Kumar Basic Pathology; Goldman-Cecil Medicine; Frameworks for Internal Medicine
This is a shared conversation. Sign in to Orris to start your own chat.