

1000075216.jpg
1000075215.jpg
Itchy anular lesion on skin since 1 yrs what is probable diagnosis and treatment in detail
analyse_media
analyse_media
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive answer.
Probable Diagnosis: Lichen Simplex Chronicus (LSC)
(Also called Circumscribed Neurodermatitis)
Note on the Term "Annular"
The lesion in the photos is not a true annular (ring with central clearing) lesion. It is a well-demarcated, hyperpigmented, lichenified plaque on the posterior neck - a classic presentation of LSC. The "annular" appearance may refer to the roughly oval/circumscribed outline of the thickened patch. True annular lesions with central clearing suggest tinea corporis (ringworm), but your images do not show that pattern.
What is Lichen Simplex Chronicus?
LSC results from long-term, repetitive rubbing and scratching of localized skin, causing the epidermis to become thickened and leathery. The normal skin markings become exaggerated, forming a crisscross (mosaic) pattern of flat-topped, shiny quadrilateral facets - this is called lichenification.
"Paroxysmal pruritus is the main symptom" - Andrews' Diseases of the Skin
The posterior neck is one of the most classic sites, fitting this case exactly:
"LSC... predilection for the posterolateral neck, occipital scalp, anogenital region, shins, ankles, and dorsal aspects of the hands and feet" - Dermatology 2-Volume Set 5e
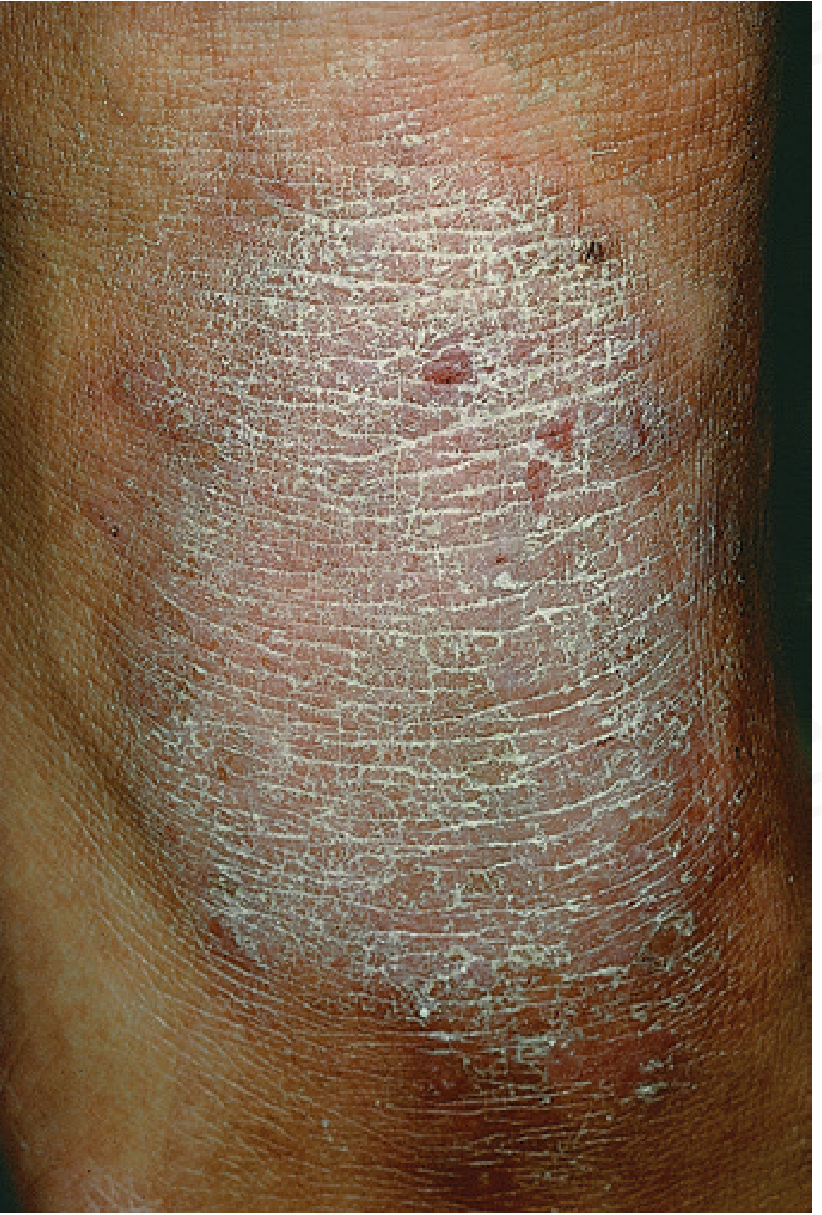
Textbook image of LSC (leg) showing the classic lichenification pattern:
Clinical Features Matching This Case
| Feature | This Patient | LSC |
|---|---|---|
| Location | Posterior neck | Classic site |
| Duration | 1 year | Chronic (insidious onset) |
| Symptom | Itchy | Paroxysmal pruritus |
| Appearance | Hyperpigmented, leathery plaque | Lichenified, hyperpigmented |
| Scaling | Mild fine scaling | Present |
| Border | Ill-defined, circumscribed | Well-demarcated patch |
Pathophysiology: The Itch-Scratch Cycle
The itch triggers scratching → scratching temporarily relieves itch → but perpetuates skin damage → which provokes more itch. This becomes a habitual, often unconscious behavior, especially worse at night and during stress.
Predisposing factors include: xerosis, atopy, anxiety, OCD, localized neuropathic itch, and systemic pruritic conditions.
Differential Diagnoses to Consider
- Tinea corporis - would show true annular ring with active, scaly, raised border and central clearing; KOH scraping would be positive
- Hypertrophic lichen planus - violaceous color, Wickham's striae
- Lichen amyloidosis - often on shins, rippled brownish papules
- Chronic atopic dermatitis - history of atopy, other flexural involvement
- Psoriasis - silvery micaceous scale, well-defined border
Treatment in Detail
1. Break the Itch-Scratch Cycle (Most Important)
- Patient education: Explain the itch-scratch-itch perpetuation. The patient must consciously resist scratching even when the itch is felt.
- Behavior modification: Substitute scratching with applying cold compress or pressing the area
- Informal insight-oriented psychotherapy if anxiety/habit is prominent
2. Topical Corticosteroids (First-Line)
- High-potency steroid (e.g., Clobetasol propionate 0.05% cream/ointment) initially - applied twice daily for 2-4 weeks
- Shift to medium-strength (e.g., Betamethasone valerate 0.1%) as lesion improves
- Occlusion (covering with plastic wrap or hydrocolloid dressing after application) significantly increases potency and prevents scratching
- Flurandrenolide tape (Cordran tape) - provides occlusion + anti-inflammatory action simultaneously; cut to fit the lesion
- Do NOT use high-potency steroids indefinitely (risk of skin atrophy, depigmentation)
3. Intralesional Corticosteroids
- Triamcinolone acetonide 2.5-5 mg/mL injected intralesionally for thick, resistant plaques
- Caution: avoid too-superficial injection (risk of atrophy and depigmentation lasting months)
- Do not inject into infected lesions
4. Topical Antipruritic Agents
- Topical doxepin cream - antihistamine/antipruritic
- Capsaicin 0.025-0.075% cream - depletes substance P, reduces itch (burning sensation initially)
- Topical pimecrolimus 1% cream or tacrolimus 0.1% ointment (calcineurin inhibitors) - effective adjuncts, steroid-sparing, safe for long-term use on the neck
5. Oral Antipruritic Agents
- Antihistamines: Hydroxyzine 25 mg at night (sedating, helps nocturnal itch), Diphenhydramine
- Anxiolytics: For anxiety-driven scratching
- Gabapentinoids (gabapentin, pregabalin): Useful for neuropathic itch component
- Antidepressants: Oral doxepin (low dose), amitriptyline - for refractory cases with psychological overlay
- Clonazepam: In severe debilitating cases
6. Physical/Procedural Options
- Hydrocolloid dressings: Repeated application reduces lichenification
- Unna boot (zinc oxide-impregnated bandage): Complete occlusion for the most severe cases to break the cycle
- Phototherapy (NB-UVB): For widespread or refractory cases
- Botulinum toxin A injection: Has been reported as curative in some cases
- Transcutaneous electrical stimulation / focused ultrasound: Emerging options for resistant LSC
7. Treat Underlying Causes
- Look for and treat: atopic dermatitis, contact dermatitis, psoriasis, systemic pruritus (thyroid, renal, liver disease)
- If fungal infection is suspected (do KOH scraping), treat with topical antifungal first
Important Points for Management
- Recurrences are common - even after complete clearance, another site may be affected
- Long-term perspective: Stress that this is a chronic condition; short bursts of treatment are insufficient
- Secondary infection: If excoriation sites show signs of infection, add a topical or oral antibiotic
- Hyperpigmentation: Often persists even after the lichenification resolves; reassure the patient it will fade gradually
Sources: Andrews' Diseases of the Skin (Clinical Dermatology), p. 71 | Dermatology 2-Volume Set 5e, p. 129 | Textbook of Family Medicine 9e, p. 932
Can we use clobetasol plus salicylic acid?
Finding Sources
Finding Sources
Searching the Web
clobetasol propionate salicylic acid combination lichen simplex chronicus lichenification treatment
Yes - Clobetasol + Salicylic Acid is a Valid and Rational Combination for LSC
Why This Combination Works
The two agents work synergistically in lichenified skin:
| Agent | Action | Benefit in LSC |
|---|---|---|
| Clobetasol propionate 0.05% | Superpotent corticosteroid - suppresses inflammation, reduces pruritus | Breaks the itch component of the itch-scratch cycle |
| Salicylic acid 3-6% | Keratolytic - softens and breaks down thickened stratum corneum | Removes the hyperkeratotic layer, allowing clobetasol to penetrate deeper into the lichenified plaque |
In lichenified skin like this posterior neck LSC plaque, the epidermis is significantly thickened. Clobetasol alone may have limited penetration through this hyperkeratotic barrier. Salicylic acid physically loosens the compacted keratin layer first, making the clobetasol far more effective.
Standard Formulation
The commercially available and pharmacy-compounded combination is:
- Clobetasol propionate 0.05% + Salicylic acid 3-6% in an ointment base
- Ointment base is preferred over cream for dry, lichenified plaques (better occlusion and penetration)
How to Use It
- Apply once or twice daily to the lichenified plaque only
- Limit use to 2-4 weeks continuously (superpotent steroid restriction)
- Can be used with occlusion (covering with plastic wrap or hydrocolloid dressing at night) for maximum effect on thick plaques
- After initial response, step down to a medium-potency steroid alone (without salicylic acid) for maintenance
Cautions Specific to This Combination
- Neck skin is thin - the posterior neck is relatively thinner than palms/soles. Salicylic acid increases clobetasol absorption, so the risk of systemic absorption and local atrophy is higher than with clobetasol alone. Limit use strictly to 2 weeks.
- Do not apply to broken or excoriated skin - salicylic acid on open skin causes stinging/pain and can cause systemic salicylism if applied over large areas.
- Avoid near the hairline scalp extensively - salicylic acid can cause hair shaft damage if applied repeatedly to the scalp.
- Salicylism risk is low when used on a small localized plaque, but relevant if applied widely.
- Children: Use with caution; salicylic acid systemic absorption is proportionally higher in children.
Practical Recommendation for This Patient
Phase 1 (Weeks 1-2): Clobetasol 0.05% + Salicylic acid 3-6% ointment - apply thinly once daily at night with light occlusion (bandage or hydrocolloid patch) to break down the lichenification.
Phase 2 (Weeks 3-6): Switch to Mometasone furoate 0.1% or Betamethasone valerate 0.1% cream - twice daily without the salicylic acid, as the plaque is now thinner and better penetrated.
Phase 3 (Maintenance): Tacrolimus 0.1% ointment or Pimecrolimus 1% cream - steroid-sparing, safe for longer use on the neck. Add oral hydroxyzine 25 mg at bedtime for nocturnal itch.
Throughout all phases: Reinforce habit-breaking - no scratching, apply cold compress when itch is felt.
Bottom line: This is a well-established, rational combination widely used by dermatologists for thick, lichenified plaques. Just keep the duration short (2 weeks) given the superpotent steroid on neck skin, then step down promptly.
This is a shared conversation. Sign in to Orris to start your own chat.