Ascariasis complete microbiology notes for university students exams
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
I now have all the essential content from multiple authoritative textbooks plus 3 high-quality images. Let me now compile the complete, exam-ready notes.
Ascariasis - Complete Microbiology Notes for University Examinations
Sources: Sherris & Ryan's Medical Microbiology (8th ed.), Goldman-Cecil Medicine, Henry's Clinical Diagnosis and Management by Laboratory Methods, Medical Microbiology 9e
1. Classification & Taxonomy
| Feature | Detail |
|---|---|
| Kingdom | Animalia |
| Phylum | Nematoda (roundworms) |
| Class | Chromadorea |
| Order | Ascaridida |
| Family | Ascarididae |
| Genus/Species | Ascaris lumbricoides |
| Common name | Giant intestinal roundworm / human roundworm |
| Type | Intestinal nematode (non-segmented, nonsegmented) |
- A. suum (pig roundworm) is nearly identical morphologically and can infect humans; it is associated with swine farmers and use of pig manure as fertilizer.
2. Morphology
Adult Worm
- Largest nematode infecting the human intestinal tract
- Female: 20-35 cm in length, up to 6 mm in diameter; straight tail
- Male: Smaller; ventrally curved (coiled) tail - key distinguishing feature
- Color: Pinkish/yellowish-white in life; reddish-orange when freshly expelled
- Three prominent lips at the anterior end (a hallmark of ascarid worms)
- Adult worms do not attach to the mucosa; they maintain position by constant motion
Mass of adult A. lumbricoides worms recovered after mebendazole treatment:

Eggs (Diagnostic Stage)
| Type | Size | Appearance |
|---|---|---|
| Fertilized (unembryonated) | 55-75 x 35-50 µm | Round to slightly oval; yellow-brown, irregular mamillated (bumpy) outer coat; thick shell; single cell inside |
| Decorticated (lost outer coat) | Same size | Smooth, may resemble hookworm eggs - diagnostic pitfall |
| Unfertilized | Up to 90 µm in length | More elongate; thinner shell; irregular internal globules (no organized contents); produced by females without males |
Microscopic appearance of a fertilized, unembryonated A. lumbricoides egg:
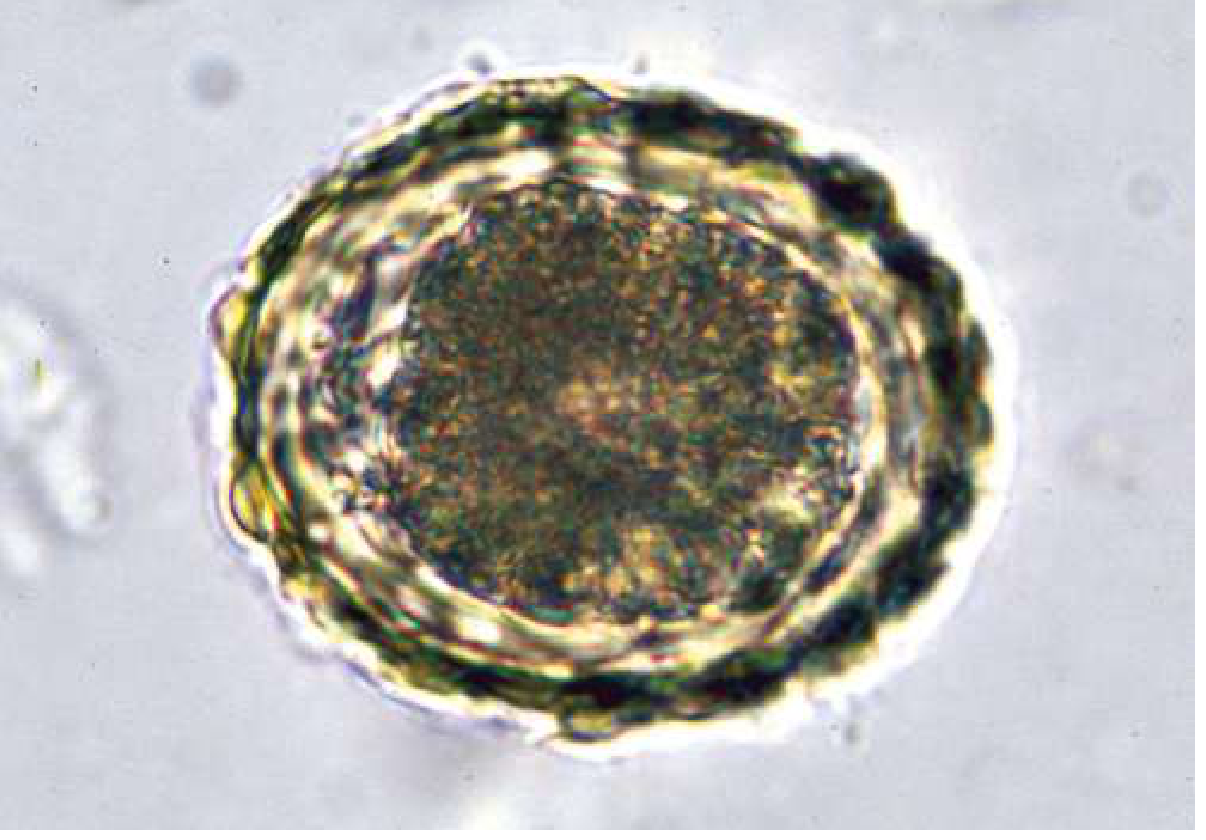
Exam tip: The thick outer mamillated (bumpy, albuminous) coat stained golden-brown by bile is a classic and highly testable egg feature.
3. Life Cycle
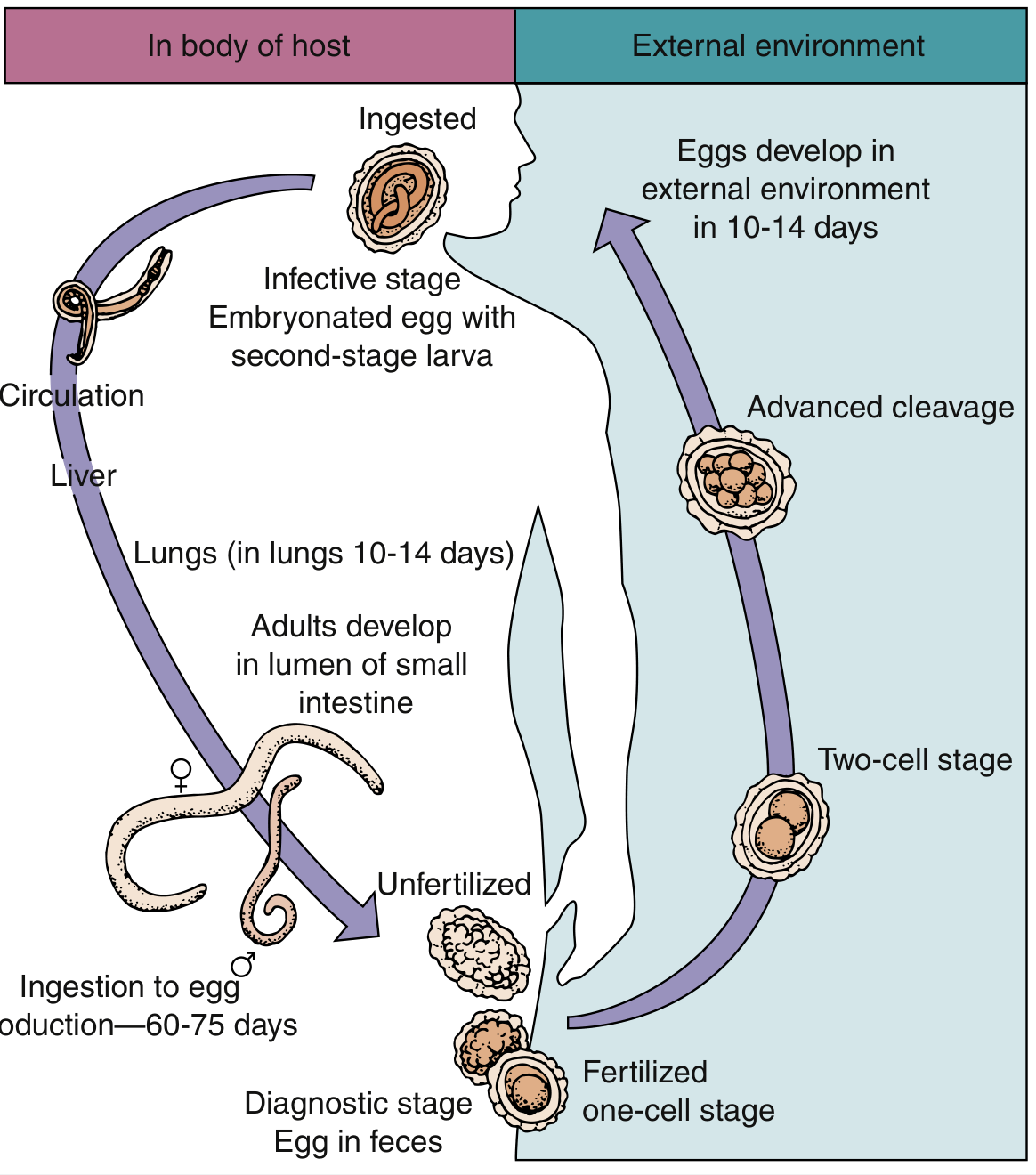
Life cycle diagram of Ascaris lumbricoides:
Step-by-Step Life Cycle
1. Egg Ingestion (Infection)
- Infective stage: embryonated egg containing a 2nd-stage larva
- Route: Feco-oral - ingestion of embryonated eggs via contaminated food, water, or soil (geophagia in children)
- Humans are the only definitive host
2. Gastric Dissolution
- Outer shell dissolved by gastric acid in the stomach
- Larvae released into the small intestine
3. Intestinal Penetration & Migration (Larval Phase)
- Larvae penetrate the duodenal/intestinal wall
- Enter the portal circulation → carried to the liver
- Travel via the heart → enter the pulmonary circulation
- Larvae penetrate the alveolar capillary bed and enter alveoli
- Remain in lungs for approximately 10-14 days, growing and molting
4. Ascent & Return to Intestine (Larval Phase continued)
- Larvae ascend the bronchial tree via ciliary action
- Reach the epiglottis - coughed up and swallowed
- Return to the small intestine (primarily jejunum)
- Develop into adult male and female worms
5. Maturation & Egg Production (Intestinal Phase)
- Adult development complete: 9-11 weeks after initial egg ingestion (60-75 days total for egg to appear in feces)
- Female produces over 200,000 eggs per day
- Adult worms survive approximately 18 months in the host
- Unfertilized eggs can be produced by females in the absence of males
6. Egg Development in Soil (External Phase)
- Passed eggs are unembryonated at time of excretion
- Require warm, moist, shady soil for embryonation
- Become infective in 2-4 weeks (some sources say 2 weeks in optimal conditions, 4-6 weeks typically)
- Eggs are extremely hardy: resist extreme temperatures, desiccation; viable in soil for up to 15 years
Key distinction: There is NO intermediate host in the A. lumbricoides life cycle. Humans are both the definitive host and the route of transmission. Autoinfection does NOT occur (unlike Strongyloides stercoralis).
4. Epidemiology
| Factor | Detail |
|---|---|
| Global burden | ~730 million to 1.3 billion people infected worldwide - most common helminthic infection |
| Distribution | Sub-Saharan Africa, South and Southeast Asia, Latin America; rural areas with poor sanitation |
| Age group | Children 4-15 years have highest prevalence and intensity; adults less affected |
| Risk factors | Inadequate sanitation; use of human feces ("night soil") as fertilizer; geophagia (eating soil); lack of clean water |
| Climate | Warm, humid climates favor egg embryonation |
| Reservoir | Humans are the only host for A. lumbricoides; pigs for A. suum |
- Eggs can remain viable in contaminated soil for 3 years or more (some sources cite up to 15 years)
- In endemic areas, transmission is often seasonal (e.g., Arabian Peninsula - rainy season triggers outbreaks)
5. Pathogenesis & Pathology
Phase 1: Pulmonary (Larval Migration)
- Larvae cause physical disruption of alveolar walls
- Hypersensitivity reaction to secreted larval antigens
- More severe on re-exposure (sensitized individuals)
- Results in: Loeffler syndrome (see Clinical Manifestations)
- Accompanied by peripheral eosinophilia (hallmark of tissue-invasive helminths)
Phase 2: Intestinal (Adult Worm)
- Adult worms compete for host nutrition (protein, carbohydrate, vitamins)
- In children: growth retardation, malnutrition, impaired cognitive development
- Heavy worm burdens → tangled bolus → intestinal obstruction (more common in children due to smaller bowel lumen)
- Worms do NOT secrete anticoagulants; they do NOT cause blood-loss anemia (unlike hookworm)
Ectopic Migration (Dangerous Complications)
Worms can migrate out of the small intestine, especially triggered by:
- Fever
- Inappropriate drug use (drugs other than anti-helmintics)
- Some anesthetics
- Mixed infections
Ectopic sites include:
- Common bile duct - biliary colic, obstructive jaundice, cholangitis
- Pancreatic duct - pancreatitis
- Liver - recurrent pyogenic cholangiohepatitis, hepatic abscess
- Appendix - appendicitis
- Stomach - rarely, gastric outlet obstruction
- Perforation of the intestinal wall → peritonitis with secondary bacterial infection (e.g., Klebsiella pneumoniae)
Exam tip: Before elective surgery under anesthesia in endemic areas, anthelmintics are routinely given to prevent anesthetic-triggered worm migration.
6. Clinical Manifestations
A. Pulmonary Phase (Loeffler Syndrome)
- Occurs ~1-2 weeks after heavy ingestion of eggs
- Wheezing, dyspnea, paroxysmal non-productive cough
- High fever - may last 2-3 weeks then resolve spontaneously
- Urticarial rash, angioedema
- Abdominal pain, vomiting (may coincide)
- CXR: bilateral diffuse mottled (migratory) pulmonary infiltrates
- Peripheral eosinophilia (key laboratory finding)
- More common in areas with seasonal transmission (re-exposure phenomenon)
B. Intestinal Phase
| Worm Burden | Manifestations |
|---|---|
| Light (few worms) | Usually asymptomatic |
| Moderate | Abdominal pain, nausea, diarrhea, abdominal distension |
| Heavy | Intestinal obstruction (colicky pain, vomiting, constipation), malnutrition, growth retardation in children |
C. Ectopic / Complicated Ascariasis
- Biliary ascariasis: RUQ pain, jaundice, cholangitis, cholecystitis
- Pancreatic ascariasis: Acute pancreatitis
- Hepatic ascariasis: Recurrent pyogenic cholangiohepatitis (classic association with Klebsiella co-infection)
- Appendiceal ascariasis: Acute appendicitis
- Intestinal perforation: Peritonitis
7. Diagnosis
1. Stool Microscopy (Gold Standard)
- Ova and parasite (O&P) examination of fresh stool
- Fertilized eggs highly characteristic - identify by mamillated outer coat
- Female produces 200,000 eggs/day: even a single worm is likely detectable
- Quantitative assessment:
- <20 eggs per slide (2 mg feces) = light infection
-
100 eggs per slide = heavy infection
- Unfertilized eggs may be missed if only fertilized eggs are expected
2. Macroscopic / Clinical
- Recovery of adult worms passed in feces or vomited
- Worms may be visible in stool with naked eye
3. Imaging
- Ultrasound / X-ray / CT: Can detect adult worms as filling defects ("double-tube sign" in bile ducts)
- Chest X-ray: Loeffler syndrome - bilateral transient eosinophilic infiltrates (during larval migration)
4. Serology / Other
- Not routinely used; eosinophilia on CBC is a supportive finding (especially during larval migration phase)
- ELISA-based serological tests exist but are not standard
Exam tip: During the pulmonary (larval migration) phase, stool examination will be negative for eggs (too early - prepatent period). Eosinophilia + pulmonary symptoms + travel history should raise suspicion even with negative stool.
8. Treatment
Drugs of Choice
| Drug | Mechanism | Notes |
|---|---|---|
| Albendazole (1st line) | Inhibits microtubule polymerization (binds β-tubulin) → impairs glucose uptake → worm paralysis/death | Single dose effective; drug of choice |
| Mebendazole (1st line) | Same as albendazole (benzimidazole class) | Alternative first-line |
| Ivermectin | Activates glutamate-gated Cl⁻ channels → hyperpolarization → paralysis | Alternative |
| Pyrantel pamoate | Nicotinic acetylcholine receptor agonist → spastic paralysis | Effective alternative |
| Piperazine | GABA-A agonist → flaccid paralysis | Older alternative; less used |
Important Treatment Note
- In patients with mixed infections (Ascaris + other helminths + Giardia + Entamoeba), treat ascariasis FIRST
- Rationale: Treating other organisms first may cause worm migration, intestinal perforation, or biliary obstruction
9. Prevention & Control
| Strategy | Details |
|---|---|
| Sanitation | Proper sewage disposal; avoid use of human feces as fertilizer |
| Personal hygiene | Handwashing, nail clipping, food washing |
| Water treatment | Clean drinking water; avoid irrigation of vegetables with untreated sewage |
| Mass drug administration (MDA) | WHO-recommended deworming of school-age children in endemic areas |
| Education | Community awareness programs |
| Food handling | Thorough washing of raw vegetables; avoiding contaminated water |
- Eggs are resistant to chlorination at normal concentrations - chemical disinfection alone is insufficient
- Reinfection is very common after treatment without environmental remediation
10. Key Distinguishing Features (Exam Comparison Table)
| Feature | A. lumbricoides | Hookworm (Ancylostoma/Necator) | Enterobius vermicularis | Trichuris trichiura |
|---|---|---|---|---|
| Size | Largest (20-35 cm) | Small (1-1.5 cm) | Small (1 cm) | Medium (4 cm) |
| Infection route | Ingestion of egg | Skin penetration of larva | Ingestion of egg | Ingestion of egg |
| Pulmonary migration | Yes (Loeffler) | Yes | No | No |
| Anemia | No | Yes (blood-sucking) | No | Yes (mild) |
| Key complication | Obstruction, biliary migration | Iron-deficiency anemia | Perianal pruritus | Rectal prolapse (heavy) |
| Diagnostic test | Stool O&P | Stool O&P | Scotch tape test | Stool O&P |
| Egg characteristics | Mamillated coat | Thin shell, segmented larva | Flattened on one side | Barrel-shaped, bipolar plugs |
11. High-Yield Exam Summary
| Topic | Key Fact |
|---|---|
| Most common helminthic infection worldwide | Ascaris lumbricoides |
| Infective stage | Embryonated egg (2nd-stage larva inside) |
| Diagnostic stage | Fertilized egg in feces |
| Egg production | ~200,000/day per female |
| Prepatent period | 60-75 days (egg to detectable egg in stool) |
| Pulmonary syndrome | Loeffler syndrome - eosinophilia + migratory infiltrates |
| Most dangerous complication | Ectopic migration to biliary/pancreatic ducts |
| Drug of choice | Albendazole or Mebendazole |
| Key lab finding | Peripheral eosinophilia (tissue-invasive stage) |
| Egg viability in soil | Up to 15 years |
| No intermediate host | Transmission: human feces → soil → ingestion |
| Trigger for ectopic migration | Fever, anesthetics, non-anthelminthic drugs |
| Treat ascariasis BEFORE | Other mixed intestinal parasites |
12. Quick Mnemonics
- "Ascaris = A Serious Giant" - it is the largest intestinal nematode
- "LAMP" for Loeffler syndrome features: Larvae in lungs, Asthma-like cough, Mottled CXR infiltrates, Peripaeral eosinophilia
- "MAD PIPE" for treatment alternatives: Mebendazole, Albendazole, Drug of choice - Pyrantel, Ivermectin, Piperazine, Effective alternatives
- "BBC" for ectopic complications: Biliary, Biliary pancreatic, Colonic obstruction
Sources: Sherris & Ryan's Medical Microbiology 8th ed. | Goldman-Cecil Medicine International Edition | Henry's Clinical Diagnosis & Management by Laboratory Methods | Medical Microbiology 9e
This is a shared conversation. Sign in to Orris to start your own chat.