Pneumonia Vs plural effusion
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Finding Sources
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Here is the full comparison:
Pneumonia vs. Pleural Effusion - A Complete Comparison
1. Definition
| Feature | Pneumonia | Pleural Effusion |
|---|---|---|
| What is it? | Infection/inflammation of lung parenchyma (alveoli) | Abnormal accumulation of fluid in the pleural space |
| Location | Inside the lung (parenchymal) | Outside the lung, between visceral and parietal pleura |
| Primary problem | Alveoli filled with exudate/pus/fluid | Pleural cavity filled with fluid |
2. Pathophysiology
Pneumonia
Microorganisms (bacteria, viruses, fungi, atypicals) infect the lung parenchyma, triggering an inflammatory response that fills alveoli with fluid, cells, and debris. This causes alveolar consolidation and impairs gas exchange.
Pleural Effusion
Under normal conditions, pleural fluid is produced from systemic capillaries at the parietal pleura and absorbed into pulmonary capillaries at the visceral pleura. Effusion forms when this balance is disrupted, as illustrated below:
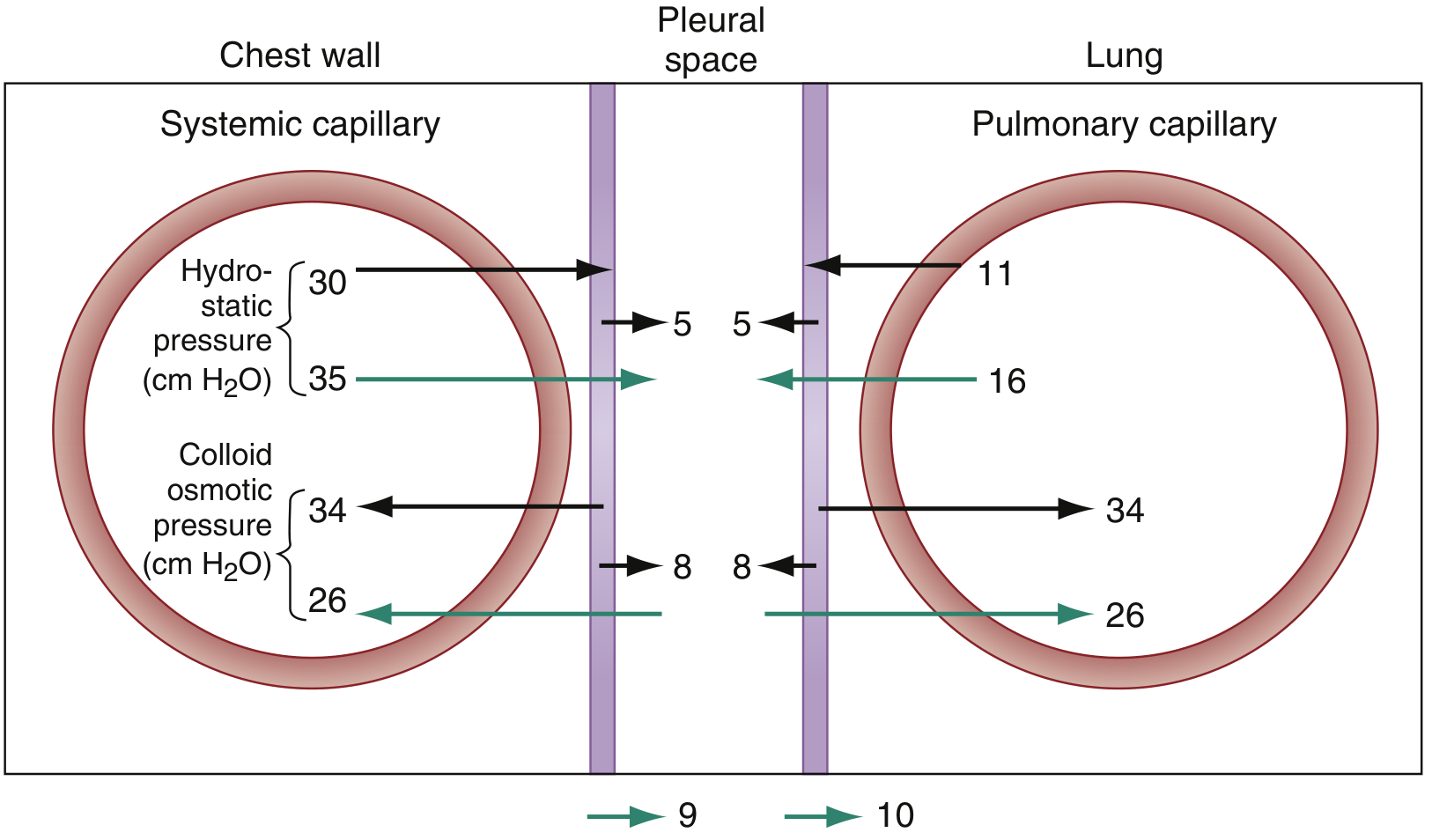
Fig. 63.5 - Pressures involved in formation and absorption of pleural fluid (ROSEN's Emergency Medicine)
Effusions are classified as:
- Transudate - due to altered hydrostatic/oncotic pressure (heart failure, cirrhosis, nephrotic syndrome)
- Exudate - due to increased capillary permeability from inflammation or malignancy (bacterial pneumonia, TB, malignancy)
3. Causes
Pneumonia
- Bacterial: Streptococcus pneumoniae (most common), Haemophilus influenzae, Klebsiella, Staphylococcus aureus, Legionella
- Viral: Influenza, COVID-19, RSV, adenovirus
- Atypical: Mycoplasma pneumoniae, Chlamydophila pneumoniae
- Fungal: Pneumocystis jirovecii (PJP), Aspergillus (immunocompromised)
Pleural Effusion - Causes by Type
Transudates:
- Congestive heart failure (most common in USA)
- Cirrhosis with ascites
- Nephrotic syndrome
- Hypoalbuminemia
- Peritoneal dialysis
Exudates:
- Bacterial pneumonia / parapneumonic effusion
- Tuberculosis
- Malignancy (lung cancer, mesothelioma, lymphoma, metastases)
- Pulmonary embolism
- Connective tissue disease (SLE, rheumatoid arthritis)
- Pancreatitis, esophageal rupture, subphrenic abscess
Note: Bacterial pneumonia itself can cause a pleural effusion (called a parapneumonic effusion), and if pus accumulates it becomes empyema (pyothorax).
4. Clinical Features
Symptoms
| Symptom | Pneumonia | Pleural Effusion |
|---|---|---|
| Cough | Prominent - usually productive | May be present (dry), less prominent |
| Fever | Common (absent in 30-40% of elderly) | Depends on cause; present if infectious |
| Dyspnea | Common | Usually only when >500 mL of fluid |
| Pleuritic chest pain | Can occur | Classic - sharp, worse with deep breathing |
| Hemoptysis | Can occur | Rare |
| Sputum | Purulent; "rusty" in pneumococcal pneumonia | None |
| Onset | Acute (bacterial) or subacute (viral/atypical) | Variable |
From Murray & Nadel's: "Pneumonia is characterized by fever, malaise, cough, sputum production, dyspnea, pleuritic pain, and hemoptysis. In older and immunocompromised patients, signs and symptoms may be muted."
From ROSEN's: "Symptoms [of pleural effusion] generally depend on the size of the effusion and underlying cause. Small pleural effusions are typically asymptomatic, and generally dyspnea does not develop until the volume reaches at least 500 mL."
5. Physical Examination - Key Differentiating Signs
| Sign | Pneumonia (Consolidation) | Pleural Effusion |
|---|---|---|
| Percussion | Dull | Stony dull |
| Breath sounds | Bronchial/tubular (harsh) | Diminished or absent |
| Tactile fremitus | Increased (consolidation transmits vibration) | Decreased/absent (fluid dampens vibration) |
| Vocal resonance | Increased (bronchophony, aegophony) | Decreased - except at the upper border where egophony may be present |
| Trachea | Central (unless massive collapse) | Shifted away from effusion if large |
| Pleural rub | Possible (if pleuritis) | Possible (pleurisy without effusion) |
| Crepitations | Fine/coarse crackles common | Usually absent |
This is the most clinically tested distinction: Increased fremitus = consolidation (pneumonia); Decreased fremitus = effusion.
6. Investigations
Chest X-Ray
| Feature | Pneumonia | Pleural Effusion |
|---|---|---|
| Finding | Lobar/segmental consolidation with air bronchograms | Blunting of costophrenic angle; meniscus sign |
| Opacity | Fluffy, non-homogeneous; air bronchograms visible | Homogeneous; lower lung field; upward concave border |
| Fissure | May show lobar boundaries | Fluid may extend up a fissure |
| Tracheal shift | Towards lesion (if collapse) | Away from effusion (if large) |
| Amount needed to detect | Any infiltrate visible | ~200 mL on upright PA CXR; ~3-5 mL on CT |
From ROSEN's: "The classic radiographic appearance of a pleural effusion is blunting of the costophrenic angle. With larger pleural effusions, the hemidiaphragm may be obscured with an upward concave appearance."
Lobar consolidation strongly suggests bacterial pneumonia over PJP or TB (sensitivity 54%, specificity 90%, LR+ 5.6).
CT Scan
- Pneumonia: Ground-glass or consolidative opacities; air bronchograms; identifies location and complications
- Pleural Effusion: Gold standard; can detect as little as 3-5 mL; distinguishes parenchymal from pleural disease; identifies underlying cause
Ultrasound
- Pneumonia: Can show consolidation with hepatization pattern
- Pleural Effusion: More sensitive than CXR; identifies as little as 50 mL; classifies as simple (hypoechoic/transudative) vs. complex (septations, loculations = exudative/empyema)
Lab Tests
| Test | Pneumonia | Pleural Effusion |
|---|---|---|
| WBC | Leukocytosis (bacterial); normal/low (viral) | Depends on cause |
| CRP/PCT | Elevated | Elevated if infective cause |
| Sputum/BAL culture | Key for pathogen ID | Not applicable |
| Blood cultures | Positive in ~10-15% of bacteremic pneumonia | Not applicable |
| Thoracentesis fluid | N/A | Light's criteria to differentiate exudate vs. transudate |
| Pleural fluid pH | N/A | <7.2 suggests empyema needing drainage |
| Pleural LDH/protein | N/A | Exudate: protein >0.5 of serum; LDH >0.6 of serum |
7. Complications
| Pneumonia | Pleural Effusion |
|---|---|
| Parapneumonic effusion / Empyema | Trapped lung / Pleural fibrosis |
| Lung abscess | Tension hydrothorax (rare) |
| Bacteremia / Sepsis | Empyema (if infected) |
| ARDS | Respiratory failure (massive effusion) |
| Respiratory failure | Mediastinal shift |
8. Management
Pneumonia
- Antibiotics (bacterial): Empiric broad-spectrum - adjusted based on setting (CAP, HAP, VAP), severity, and pathogen
- CAP (outpatient): Amoxicillin ± macrolide, or doxycycline
- CAP (inpatient): Beta-lactam + macrolide, or fluoroquinolone monotherapy
- HAP/VAP: Broad-spectrum (piperacillin-tazobactam, carbapenems ± MRSA coverage)
- Antivirals (influenza: oseltamivir; COVID-19: antivirals, dexamethasone)
- Supportive care: O2, fluids, physiotherapy
Pleural Effusion
- Treat the underlying cause (diuretics for heart failure; antibiotics for parapneumonic effusion)
- Diagnostic thoracentesis - for any unexplained effusion
- Therapeutic thoracentesis - for symptomatic relief (large effusions causing dyspnea)
- Chest tube drainage - for empyema, large parapneumonic effusion with pH <7.2
- Pleurodesis (chemical/VATS) - for recurrent malignant effusions
- Indwelling pleural catheter (IPC) - for trapped lung or poor performance status
Management algorithm for malignant pleural effusion (MPE):
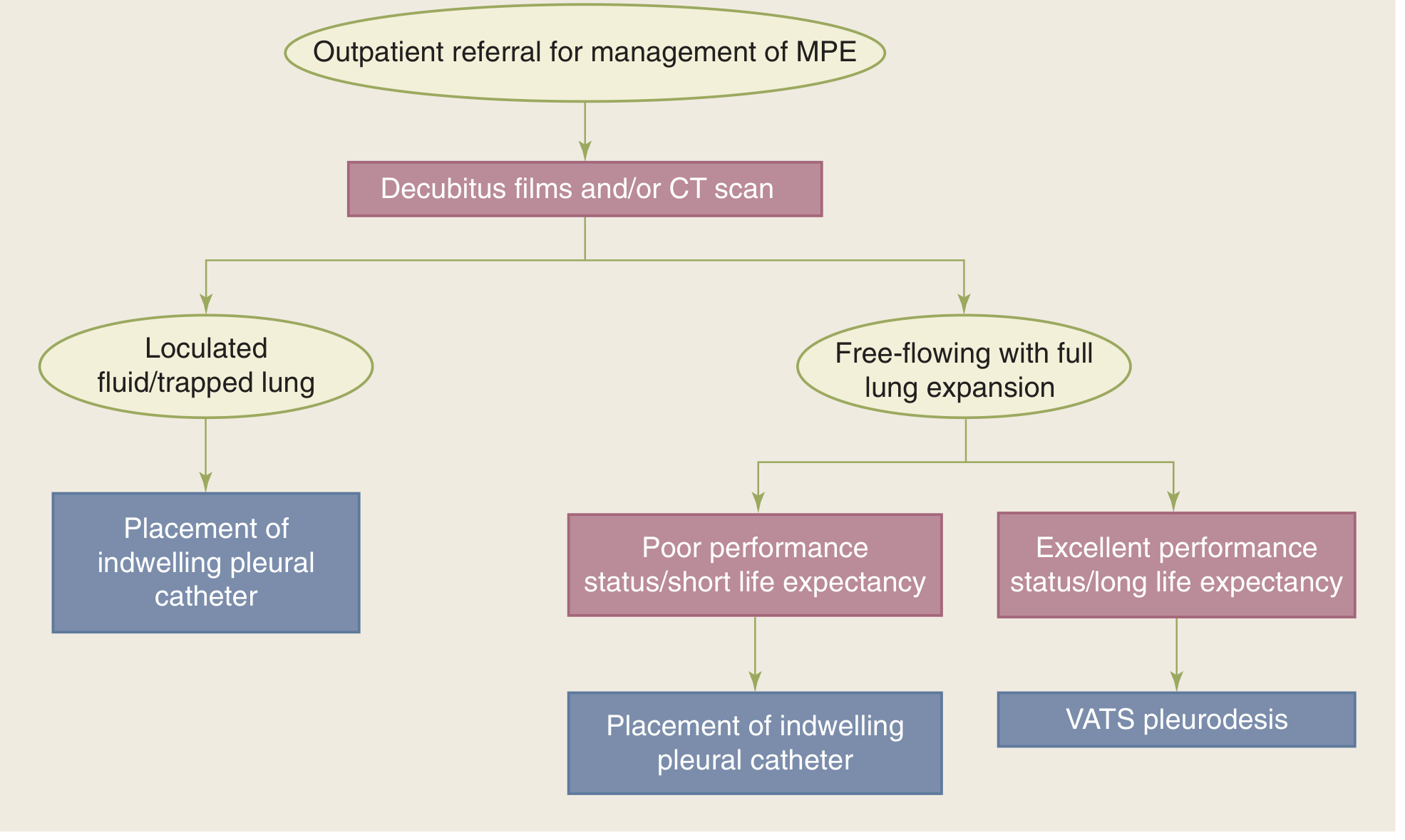
Figure 19-51 - Treatment decision algorithm for malignant pleural effusion (Schwartz's Principles of Surgery, 11e)
9. Quick Summary Comparison Table
| Feature | Pneumonia | Pleural Effusion |
|---|---|---|
| Pathology location | Lung parenchyma (alveoli) | Pleural space |
| Mechanism | Infection/inflammation of alveoli | Fluid accumulation between pleural layers |
| Cough | Prominent, productive | Mild or absent |
| Fever | Common | Only if infective cause |
| Percussion | Dull | Stony dull |
| Fremitus | Increased | Decreased |
| Breath sounds | Bronchial | Absent/diminished |
| CXR finding | Consolidation + air bronchograms | Blunted CP angle + meniscus sign |
| Tracheal shift | Towards (if collapse) | Away (if large) |
| Key test | CXR + sputum culture | Thoracentesis (Light's criteria) |
| Treatment | Antibiotics/antivirals | Thoracentesis, treat cause |
Sources: ROSEN's Emergency Medicine, 9e | Murray & Nadel's Textbook of Respiratory Medicine | Schwartz's Principles of Surgery, 11e | Goldman-Cecil Medicine | Fishman's Pulmonary Diseases and Disorders
This is a shared conversation. Sign in to Orris to start your own chat.