Explain anatomy of inguinal canal with 3d orientation and laparoscopic anatomy
Reading File
Finding Sources
Finding Sources
Searching the Web
inguinal canal 3D anatomy laparoscopic TEP TAPP landmarks 2024
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative textbooks and rich diagrams. Let me compose the full answer.
Anatomy of the Inguinal Canal: 3D Orientation and Laparoscopic Anatomy
Overview
The inguinal canal is an oblique passage in the lower anterior abdominal wall, approximately 4-6 cm long in adults. It transmits the spermatic cord in males and the round ligament of the uterus in females, along with the ilioinguinal nerve and lymphatics in both sexes. Understanding its 3D architecture is fundamental to both open and laparoscopic hernia repair.
1. General 3D Orientation
The canal runs obliquely downward, forward, and medially, parallel to and just above the medial half of the inguinal ligament. Think of it as a slightly flattened tube tilted at about 45° in two planes simultaneously - it angles both anteriorly (deep to superficial) and medially (lateral to medial) as it crosses the abdominal wall.
Two openings (rings):
| Ring | Location | Structure |
|---|---|---|
| Deep (internal) inguinal ring | Midpoint of inguinal ligament, 2-3 cm above femoral artery pulse; lateral to inferior epigastric vessels | Defect in transversalis fascia; marks the internal start of the canal |
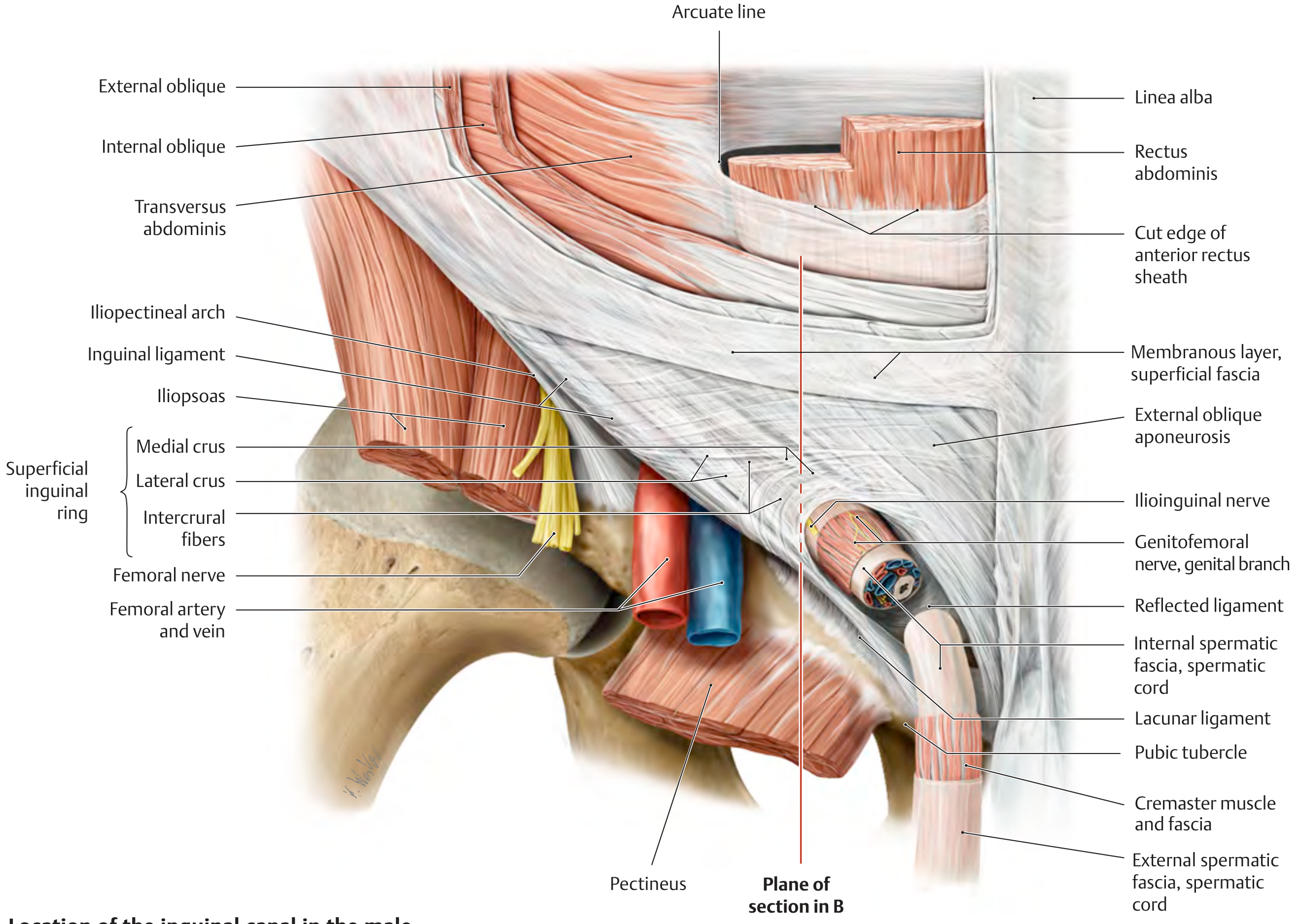
| Superficial (external) inguinal ring | Just superolateral to pubic tubercle | Inverted V-shaped defect in external oblique aponeurosis, bounded by medial crus, lateral crus, intercrural fibers, and reflected ligament |
The deep ring lies in the lateral inguinal fossa. The inferior epigastric vessels run just medial to it - a key surgical landmark dividing indirect from direct hernia territory.
2. Walls of the Inguinal Canal (4 Walls + 2 Rings)
This is the core of 3D understanding:
| Wall | Structure |
|---|---|
| Anterior wall | External oblique aponeurosis (full length); internal oblique muscle reinforces the lateral third |
| Posterior wall | Transversalis fascia (full length); reinforced medially by the conjoint tendon / interfoveolar ligament |
| Roof (superior wall) | Arching fibers of internal oblique and transversus abdominis, which sweep medially and descend as the conjoint tendon to attach to the pubic crest and tubercle |
| Floor (inferior wall) | Rolled and thickened lower free edge of the external oblique aponeurosis = inguinal (Poupart's) ligament; deepened medially by the lacunar ligament |
Key 3D concept - the "shutter mechanism": When intra-abdominal pressure rises, the arching internal oblique and transversus abdominis fibers contract and descend like a shutter, narrowing the deep ring and reinforcing the posterior wall. This is the physiological protection against hernia.
The area of weakness: Below the arch of the internal oblique/transversus, and medial to the deep ring, there is no muscle layer - only transversalis fascia and external oblique aponeurosis. This is the "Hasselbach's triangle" zone and the anatomical substrate for direct hernias.
3. Contents of the Inguinal Canal
In males:
- Spermatic cord (ductus deferens, testicular artery, pampiniform venous plexus, lymphatics, sympathetic fibers, cremasteric artery, artery of vas)
- Ilioinguinal nerve (runs on the cord surface, not inside it)
- Genital branch of genitofemoral nerve (runs in the cremasteric layer)
In females:
- Round ligament of uterus
- Ilioinguinal nerve
- Lymphatics
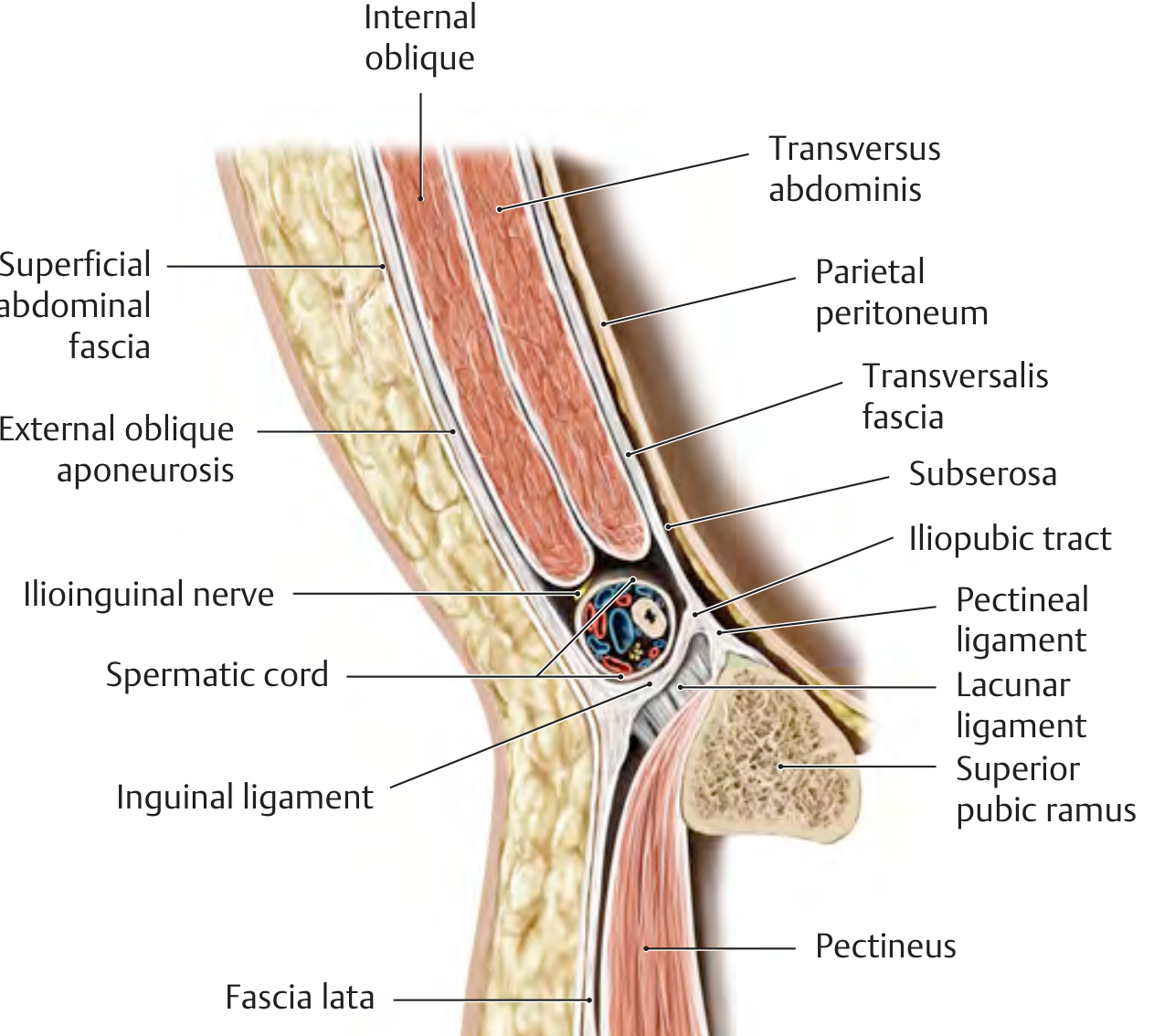
4. Fascial Coverings of the Spermatic Cord (Layers Derived from the Abdominal Wall)
As the testis descended embryologically, it carried layers of abdominal wall with it. These become the coverings of the spermatic cord:
| Abdominal layer | Corresponding spermatic cord layer |
|---|---|
| Transversalis fascia | Internal spermatic fascia (acquired at deep ring) |
| Cremaster muscle (from internal oblique) | Cremasteric fascia and muscle |
| External oblique aponeurosis | External spermatic fascia (acquired at superficial ring) |
5. Key Ligaments and Structures
- Inguinal ligament (Poupart's): Lower free edge of external oblique aponeurosis, from ASIS to pubic tubercle
- Lacunar ligament (Gimbernat's): Medial expansion of inguinal ligament, hooking onto the pecten pubis; forms the sharp medial border of the femoral ring
- Cooper's ligament (pectineal ligament): Strong fibrous band on the pecten (pectineal line) of the superior pubic ramus - the strongest fixation point for mesh in laparoscopic repair
- Iliopubic tract: A thickened band of transversalis fascia running parallel to and posterior to the inguinal ligament, from iliopectineal arch to superior pubic ramus. Critically visible laparoscopically even when the inguinal ligament is not
- Conjoint tendon (inguinal falx): Fusion of internal oblique and transversus abdominis as they insert on the pubic crest; forms the medial posterior wall and protects against direct herniation
6. Nerves of the Inguinal Region
These are crucial to understand and protect during repair:
| Nerve | Origin | Course | Supplies |
|---|---|---|---|
| Ilioinguinal (L1) | L1 | Pierces internal oblique at ASIS level; enters inguinal canal; exits through superficial ring | Scrotum/labia majora, medial thigh, base of penis/mons pubis |
| Iliohypogastric (T12-L1) | T12-L1 | Runs between internal oblique and transversus; pierces internal oblique above deep ring | Lower abdominal skin, inguinal region |
| Genitofemoral (L1-L2) | L1-L2 | Genital branch enters canal lateral to inferior epigastric vessels; runs ventral to iliopubic tract | Cremaster (genital), upper anterior thigh skin (femoral) |
| Lateral femoral cutaneous (L2-L3) | L2-L3 | Passes under inguinal ligament near ASIS | Lateral thigh |
7. Hesselbach's Triangle
The triangle defines the site of direct inguinal hernias:
- Medially: Lateral edge of rectus sheath
- Inferiorly: Inguinal ligament
- Superolaterally: Inferior epigastric vessels
A direct hernia bulges anteromedially through this triangle, medial to the inferior epigastric vessels. An indirect hernia enters lateral to them, through the deep ring.
8. Laparoscopic Anatomy (Posterior Perspective)
Laparoscopic repair views the inguinal region from inside, looking at the posterior abdominal wall - an entirely different perspective from open surgery.
8a. The Five Peritoneal Folds (Laparoscopic Landmarks)
Seen from the laparoscope looking inferiorly at the anterior wall:
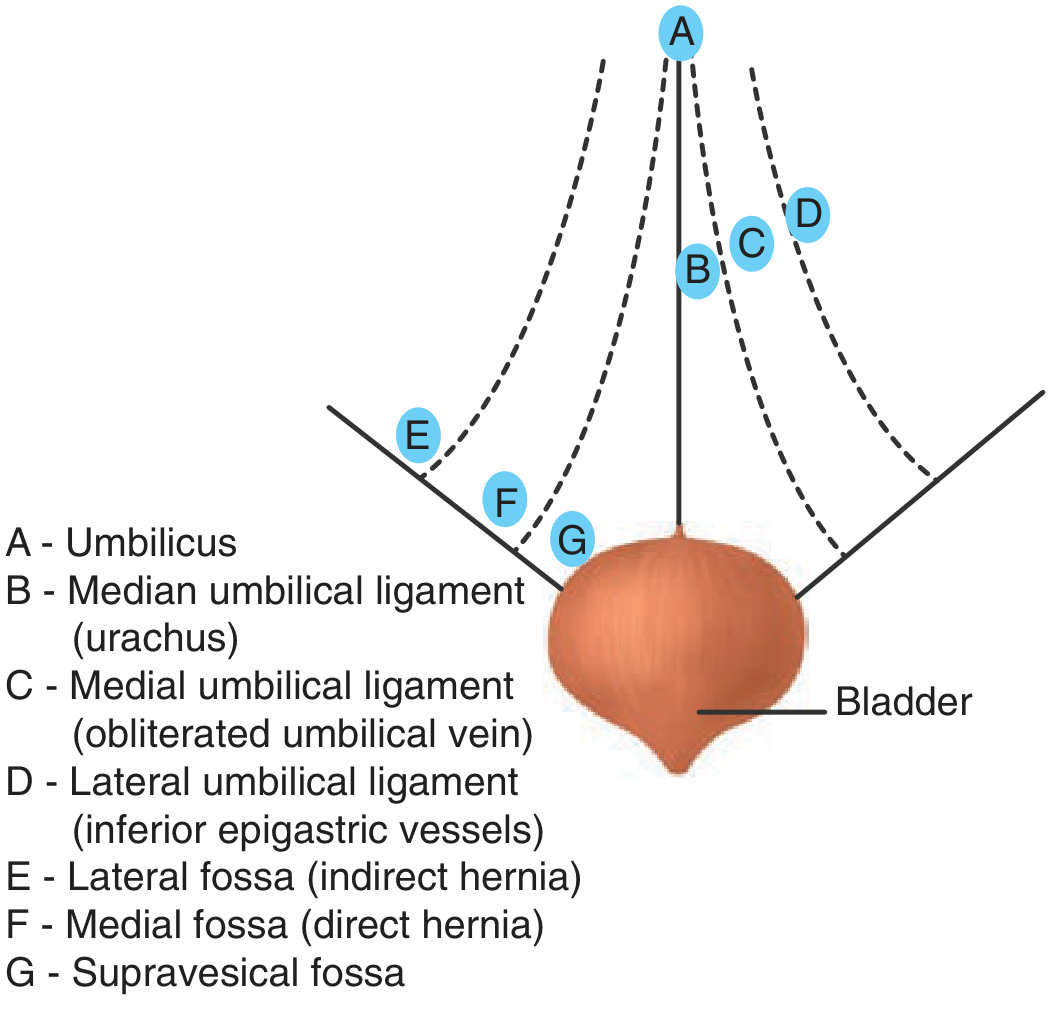
- Median umbilical fold - midline, over obliterated urachus
- Medial umbilical folds (x2) - obliterated umbilical arteries
- Lateral umbilical folds (x2) - inferior epigastric vessels - the most important surgical landmark, separating direct from indirect hernia sites
Three fossae between folds:
- Lateral fossa (lateral to inferior epigastric fold) - where indirect hernias emerge
- Medial fossa (between medial and lateral folds) - Hesselbach's triangle territory, direct hernias
- Supravesical fossa (between median and medial folds) - rare supravesical hernias
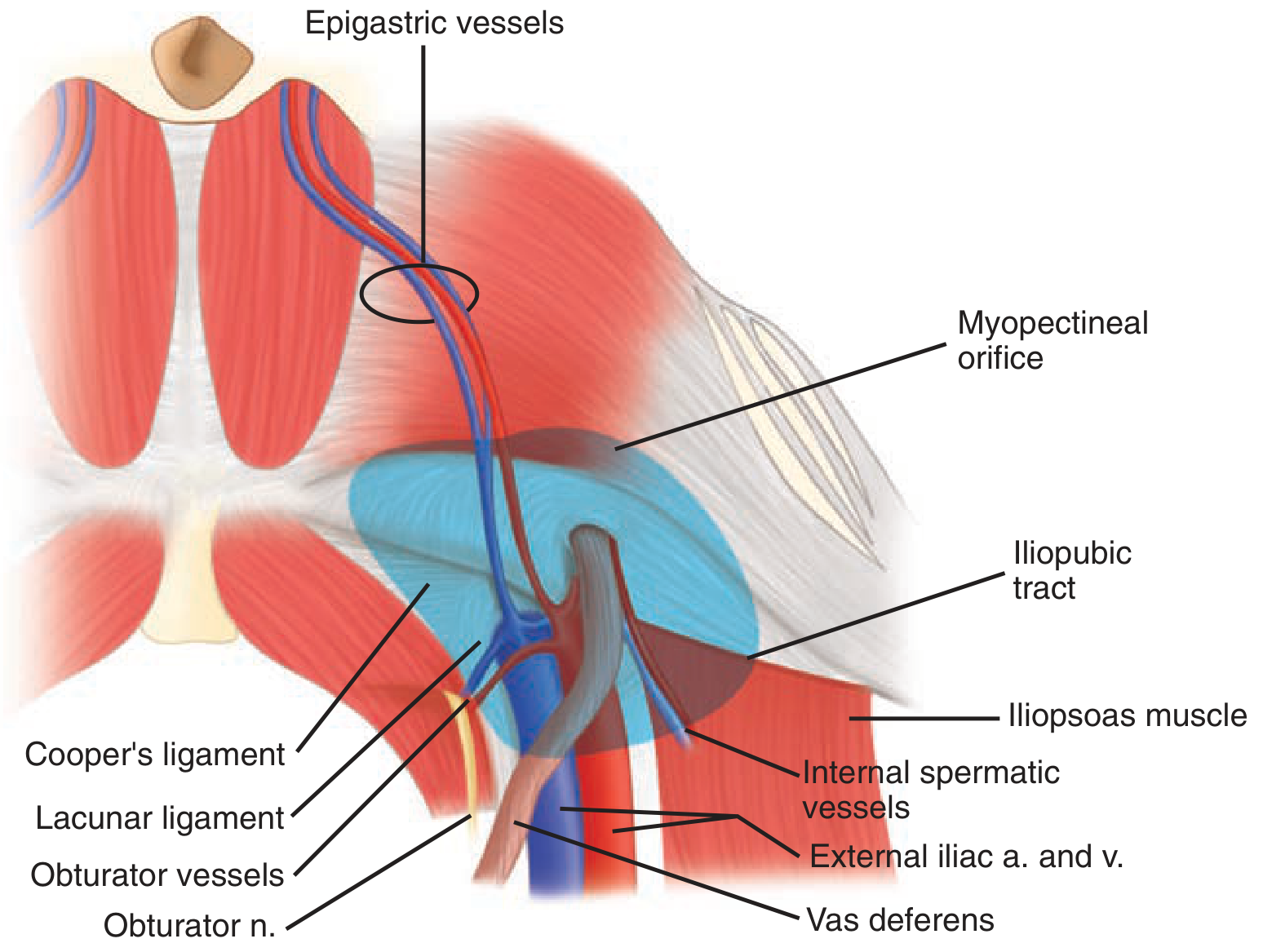
8b. Posterior Perspective - What You Actually See
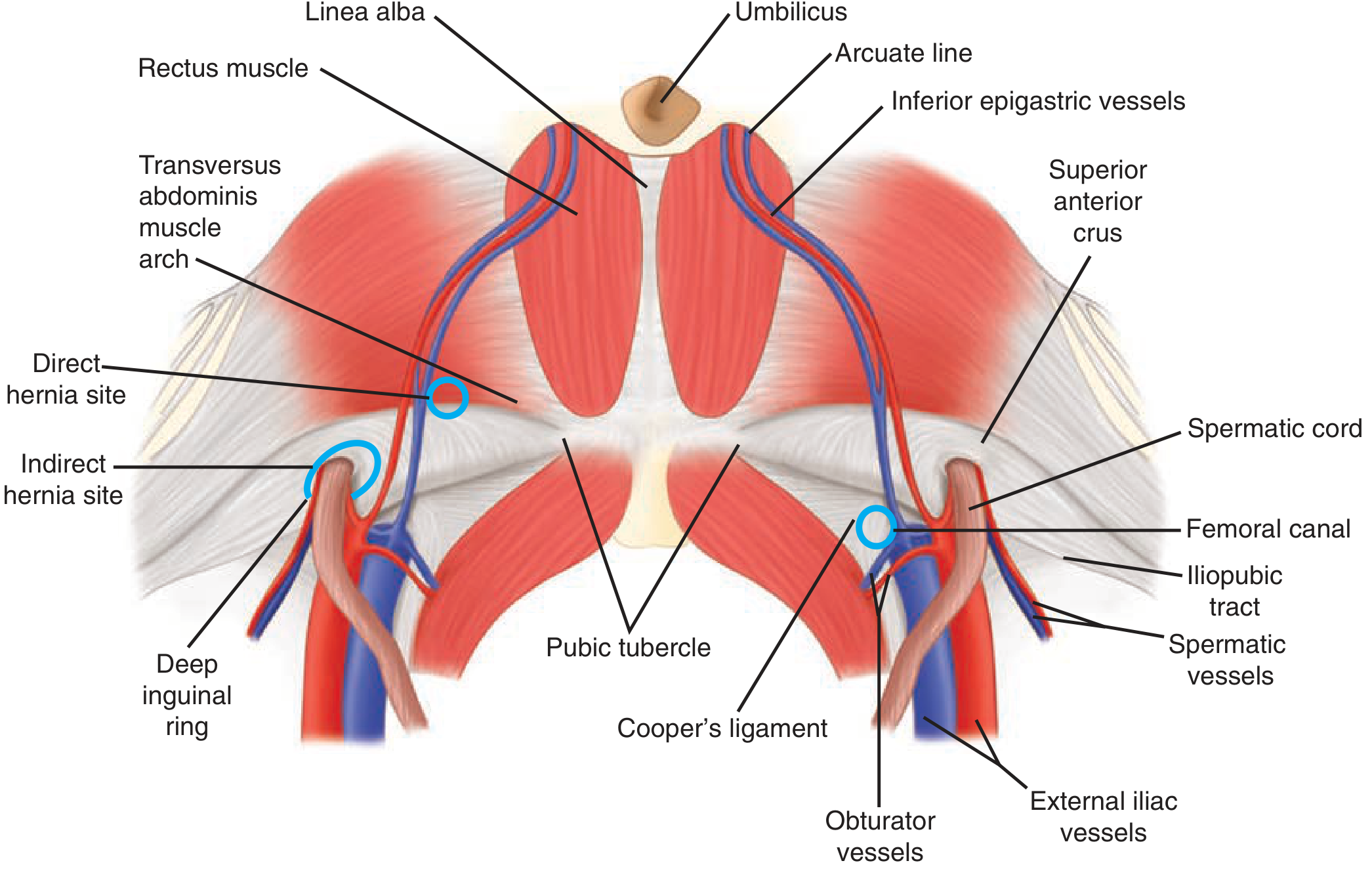
After peritoneal flap reflection (TAPP) or in the preperitoneal space (TEP), the key structures visible are:
- Inferior epigastric vessels (medial border of deep ring)
- Cooper's ligament (landmark for mesh fixation)
- Iliopubic tract (parallel and deep to inguinal ligament)
- Vas deferens (running medially)
- Internal spermatic vessels (running laterally)
- External iliac vessels
- Pubic symphysis and Cooper's ligament
8c. Myopectineal Orifice of Fruchaud
A fundamental laparoscopic concept - this is a single large oval region of weakness in the lower abdominal wall, divided by the inguinal ligament into:
- Upper half: Sites for indirect and direct inguinal hernias
- Lower half: Site for femoral hernias
The laparoscopic approach (TEP/TAPP) places a single large mesh (at least 10x15 cm) to cover the entire myopectineal orifice, simultaneously repairing all potential hernia sites on that side.
8d. Preperitoneal Spaces
Two spaces are developed during laparoscopic hernia repair:
- Space of Retzius (retropubic space): Midline, between bladder and pubic symphysis - medial working space in TEP
- Space of Bogros: Lateral preperitoneal space, bounded anteriorly by transversalis fascia, medially by inferior epigastric vessels, laterally by pelvic wall, posteriorly by psoas and external iliac vessels - lateral working space for mesh placement
9. The "Dangerous Zones" in Laparoscopic Repair
Three regions where injury causes catastrophic complications:
Triangle of Doom
- Borders: Vas deferens (medially) and gonadal/spermatic vessels (laterally)
- Contents: External iliac artery and vein, deep circumflex iliac vein, femoral nerve, genital branch of genitofemoral nerve
- Rule: Never staple, clip, or dissect within this triangle
Triangle of Pain
- Borders: Iliopubic tract (superiorly) and gonadal vessels (medially)
- Contents: Lateral femoral cutaneous nerve, femoral branch of genitofemoral nerve, femoral nerve
- Rule: Avoid any fixation device lateral to the spermatic vessels and below the iliopubic tract - this causes chronic pain/dysesthesia
Circle of Death
- Vascular anastomotic ring formed by: common iliac → internal iliac → obturator → pubic branch → inferior epigastric → external iliac
- An anomalous obturator artery ("corona mortis") replacing the normal obturator artery passes directly over Cooper's ligament in ~30% of people - dangerous during lacunar ligament incision for femoral hernia or mesh fixation to Cooper's ligament
10. TEP vs TAPP - Anatomical Approach Summary
| Feature | TEP | TAPP |
|---|---|---|
| Entry | Extraperitoneal from outset (balloon/blunt dissection in retrorectus space) | Intraperitoneal first, then peritoneal incision above hernia |
| Landmarks first seen | Posterior rectus sheath → pubic symphysis → Space of Retzius | Five peritoneal folds → peritoneal incision above lateral umbilical fold |
| Risk of visceral injury | Lower (never enters peritoneal cavity) | Higher (intraperitoneal access required) |
| Learning curve | Steeper | Slightly gentler |
| Bilateral hernias | Excellent - same preperitoneal space | Also good |
| Mesh | 10x15 cm placed over entire myopectineal orifice | Same |
| Advantage | No peritoneal closure needed | Better view for large/complex hernias |
Quick Reference: 3D Summary
ANTERIOR → External oblique aponeurosis
POSTERIOR → Transversalis fascia (+conjoint tendon medially)
ROOF → Internal oblique + transversus abdominis (arch)
FLOOR → Inguinal ligament
DEEP END (lateral) → Deep ring (transversalis fascia defect, lateral to inferior epigastric vessels)
SUPERFICIAL END (medial) → Superficial ring (external oblique aponeurosis defect, above pubic tubercle)
DIRECTION → Oblique, anteromedial, 4-6 cm
Sources: - Bailey and Love's Short Practice of Surgery 28th Ed., pp. 1087-1091 | - Schwartz's Principles of Surgery 11th Ed., pp. 1628-1630 | - THIEME Atlas of General Anatomy and Musculoskeletal System, pp. 231 | - Fischer's Mastery of Surgery 8th Ed., pp. 6093-6094 | - Maingot's Abdominal Operations
This is a shared conversation. Sign in to Orris to start your own chat.