Pathology of TB , in easy way and in 1 paper only from robbins with best memorizing trick
tuberculosis granuloma caseating necrosis histology
🫁 Pathology of Tuberculosis — Robbins (One Page)
Robbins & Kumar Basic Pathology, Chapter 11
THE BIG PICTURE (One-Line Memory Anchor)
"MTB enters → MAC responds → Granuloma forms → Caseous CENTER → Fate depends on IMMUNITY"
1. The Bug
2. The Core Lesion — GRANULOMA
| Layer (outside → in) | Cell/Component | Trick |
|---|---|---|
| Outer rim | Lymphocytes (CD4 T cells) | "L for Last defense" |
| Middle | Epithelioid macrophages | "E for Engulfers" |
| Giant cells | Langhans giant cells (nuclei at periphery in horseshoe) | "Langhans = nuclei at Lanes/edges" |
| Center | Caseous necrosis (cheese-like, pink-white, structureless) | "Cheese in the middle" |
3. How the Granuloma Forms — Immunopathology
MTB inhaled → macrophage engulfs it (phagocytosis)
↓
MTB survives inside phagosome (blocks phagolysosome fusion)
↓
Macrophage presents antigen → activates CD4 T cells (Th1)
↓
Th1 releases IFN-γ → activates macrophages fully
↓
Activated macrophages → become Epithelioid cells + fuse → Langhans giant cells
↓
TNF recruits more cells → GRANULOMA WALL forms
↓
Center gets necrotic (hypoxia + toxic macrophage products) → CASEOUS NECROSIS
4. Primary vs Secondary TB
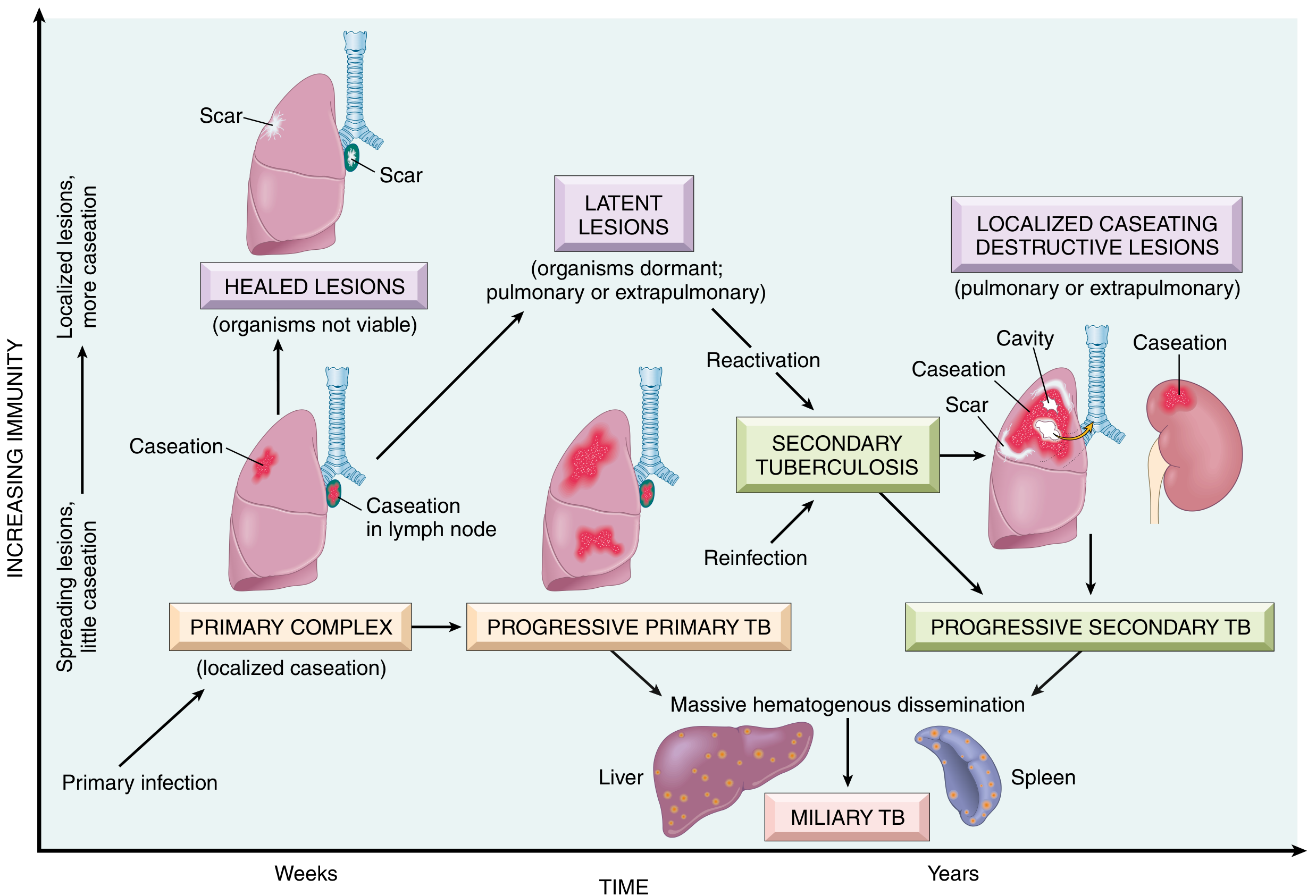
PRIMARY TB (First Infection)
- Inhaled droplet → lower/mid lung (better ventilated zones)
- Ghon focus = small subpleural granuloma (usually right lung, lower lobe)
- Spreads to hilar lymph nodes → lymph node caseates
- Ghon focus + hilar node = Ghon Complex (also called Primary Complex / Ranke Complex)
- In 95% of immunocompetent people: heals with fibrosis + calcification → becomes the Ghon complex scar visible on CXR
- Bacilli may remain dormant for decades → latent TB
SECONDARY TB (Reactivation / Reinfection)
- Occurs years later when immunity drops (HIV, steroids, diabetes, malnutrition, age)
- Always in the apex of the upper lobe (Simon's focus — seeded during primary bacteremia)
- Much more destructive — larger cavities, more caseation
5. Morphological Spectrum — What Happens to the Granuloma?
| Outcome | Pathology | Condition |
|---|---|---|
| Healing | Fibrosis → calcification | Good immunity |
| Latent | Walled-off, organisms dormant | Adequate immunity |
| Caseation + Cavity | Center liquefies, wall erodes into bronchus → cavity | Immunity weakened |
| Miliary TB | Hematogenous spread → millet-seed lesions in liver, spleen, marrow, brain | Poor immunity |
6. Cavitary TB (The Dangerous Phase)
- Caseous center liquefies (lots of bacteria, ideal for MTB growth)
- Erodes into bronchus → cavitation → organisms enter airway → patient becomes infectious
- Cavity walls: inner layer (necrotic debris) + middle (epithelioid granuloma) + outer (fibrosis)
- Rasmussen aneurysm = erosion into pulmonary artery → massive hemoptysis
7. Miliary TB
- Hematogenous spread → 1–2 mm yellow-white granulomas scattered like millet seeds in:
- Lungs, liver, spleen, bone marrow, meninges, kidneys, adrenals
- Seen in immunocompromised or untreated primary TB
- On CXR: "snowstorm" pattern
8. Histology — What You See Under the Microscope
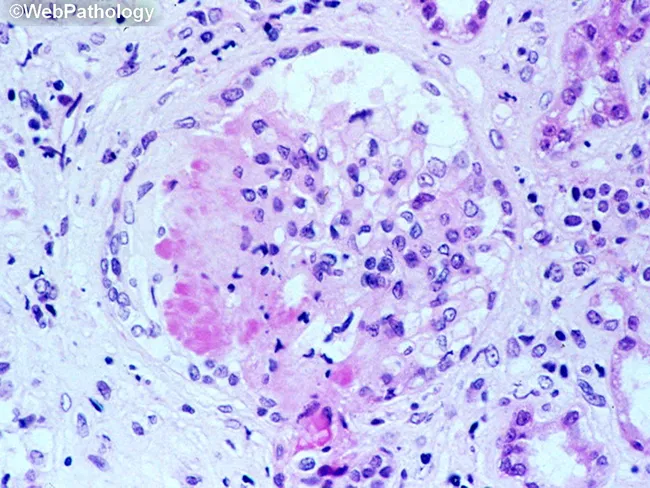
- Caseating granuloma: Pale pink (eosinophilic) structureless center = caseous necrosis
- Surrounded by epithelioid macrophages (elongated, pink, footprint-shaped nuclei)
- Langhans giant cells: multinucleated, nuclei arranged at periphery in horseshoe/crescent pattern
- Outer lymphocytic cuff
- Ziehl-Neelsen stain: bacilli appear as red rods on blue background (acid-fast)
9. Special Situations
| Scenario | Key Pathology |
|---|---|
| HIV + TB | Granulomas are poorly formed or absent (can't mount Th1 response); sheets of macrophages filled with bacilli |
| Lupus vulgaris | TB of the skin — "apple jelly" nodules |
| Pott disease | TB of the spine — vertebral body destruction |
| Addison disease | TB destroying adrenal glands |
| Long-standing TB | Risk of amyloidosis (secondary/AA amyloid) |
10. The MASTER MNEMONIC — TB Pathology in One Shot
"A MAC GIRL Lives in a CAVE"
| Letter | Meaning |
|---|---|
| A | Acid-fast bacillus (ZN stain) |
| M | Macrophage engulfs → can't kill (blocks phagolysosome) |
| A | Activated by IFN-γ (Th1 response) |
| C | Caseating necrosis in center |
| G | Ghon complex (primary TB) |
| I | Immunity determines fate |
| R | Reactivation = Secondary TB (Apex) |
| L | Langhans giant cells (horseshoe nuclei) |
| Lives in a CAVE | Cavitary TB (infectious phase) |
Quick Summary Table
| Feature | Primary TB | Secondary TB |
|---|---|---|
| Location | Lower/mid lung | Apex upper lobe |
| Lesion | Ghon focus + hilar node | Cavity, large caseation |
| Immunity | Present (heals) | Waning (reactivates) |
| Infectivity | Usually NOT infectious | INFECTIOUS |
| Spread | Lymphatic/hematogenous possible | Local + bronchial |
Pathology of malignant mesothelioma
🫁 Pathology of Malignant Mesothelioma — Robbins (One Page)
Robbins & Kumar Basic Pathology + Robbins, Cotran & Kumar Pathologic Basis of Disease
THE ONE-LINE ANCHOR
"Asbestos → 25–40 years → Pleural RIND → Epithelial / Sarcomatoid / Biphasic → Uniformly Fatal"
1. What Is It?
- Pleura (most common — 90%)
- Peritoneum
- Pericardium
- Tunica vaginalis (rare)
2. Cause — Asbestos (The Star)
| Fact | Detail |
|---|---|
| Association | 80–90% of cases have asbestos exposure history |
| Risk occupations | Shipyard workers, miners, insulators, construction |
| Even indirect exposure matters | Living near a factory / washing an asbestos worker's clothes |
| Latency period | 25–45 years (among the longest of any carcinogen) |
| Smoking link | Smoking does NOT increase mesothelioma risk (unlike lung carcinoma — key distinction!) |
| Asbestos fibers | Remain in body for life — risk never decreases after exposure |
| Lifetime risk | Up to 7–10% in heavily exposed individuals |
3. Pathogenesis — How Asbestos Causes It
Asbestos fibers inhaled
↓
Fibers accumulate near mesothelial cell layer
↓
Generate Reactive Oxygen Species (ROS)
↓
DNA damage → driver mutations accumulate over decades
↓
Key mutations:
• CDKN2A deletion (chr 9p) — ~80% of cases → loss of cell cycle control
• NF2 mutation → disrupts cell signaling
• BAP1 mutation → disrupts DNA repair (also germline = familial mesothelioma)
↓
Malignant transformation of mesothelial cells
4. Gross Morphology (Macroscopic)
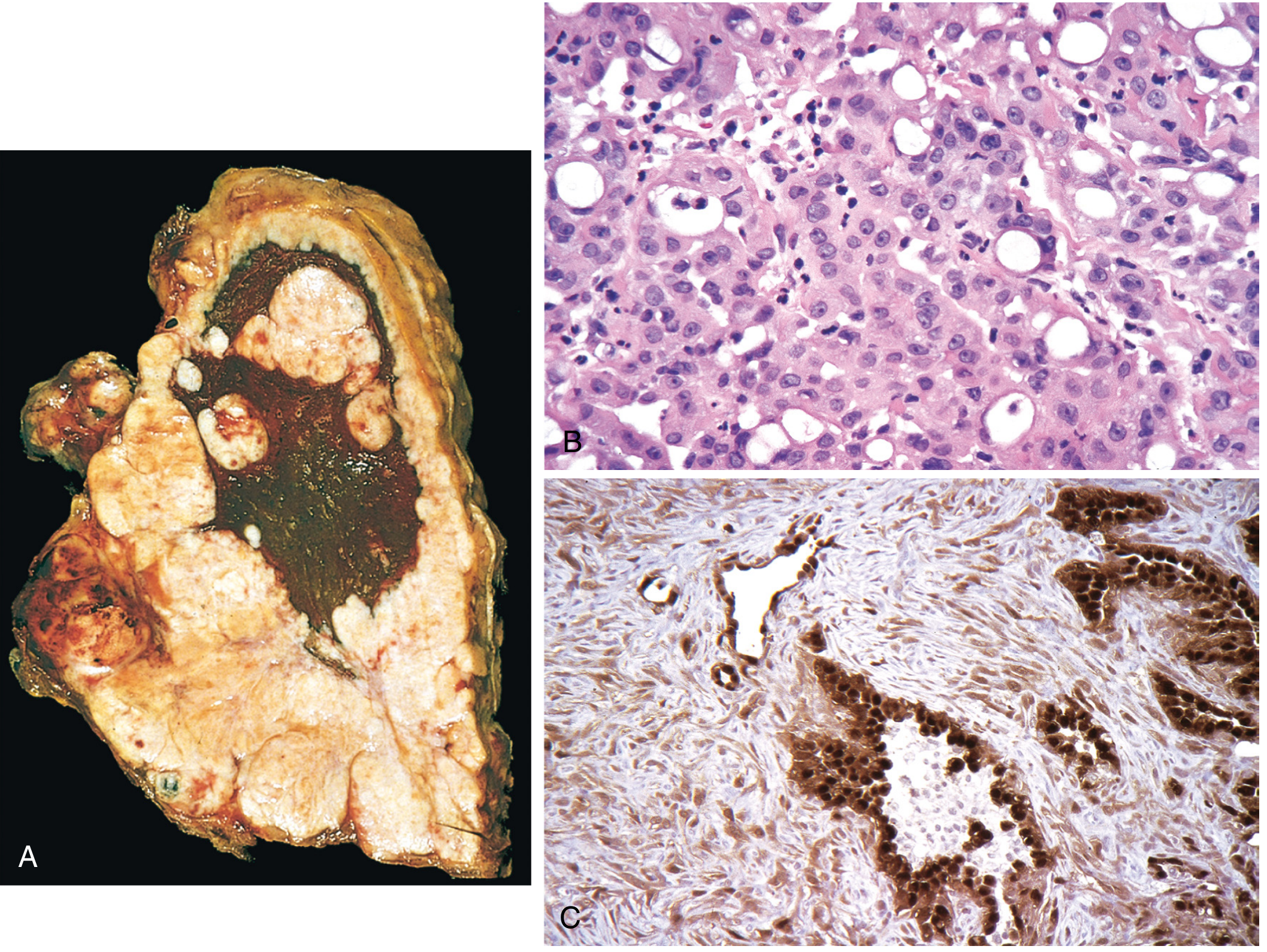
- Begins localized → spreads by contiguous growth OR diffuse pleural seeding
- Affected lung becomes ensheathed by a thick layer of yellow-white, firm, gelatinous tumor = the classic "pleural rind"
- Obliterates the pleural space
- May directly invade thoracic wall or subpleural lung tissue
- Distant metastases are uncommon (this is a local disease)
- Often preceded by pleural fibrosis and plaques (visible on CT)
- Pleural effusion almost always present (often massive, recurrent, hemorrhagic)
5. Microscopic Types (Histology)
| Type | Frequency | Appearance | Behavior |
|---|---|---|---|
| Epithelioid | 60–80% | Cuboidal/columnar cells forming tubular or papillary structures — mimics adenocarcinoma | Best prognosis (relatively) |
| Sarcomatoid | 10–12% | Spindle/fibroblastic cells in sheets, resembles fibrosarcoma; paucicellular, fibrotic | Worst prognosis |
| Biphasic | 10–15% | Both epithelioid + sarcomatoid areas | Behaves like sarcomatoid |
6. The BIG Diagnostic Challenge — Mesothelioma vs Adenocarcinoma
| Marker | Mesothelioma | Adenocarcinoma |
|---|---|---|
| Calretinin | ✅ Strongly positive | ❌ Negative |
| WT-1 (Wilms tumor 1) | ✅ Positive | ❌ Negative |
| Cytokeratin 5/6 | ✅ Positive | ❌ Negative |
| Podoplanin (D2-40) | ✅ Positive | ❌ Negative |
| Claudin-4 | ❌ Negative | ✅ Positive |
| BerEp4 | ❌ Negative | ✅ Positive |
| CEA / TTF-1 | ❌ Negative | ✅ Positive |
Rule of thumb: Calretinin = mesothelioma's signature stain (nuclear + cytoplasmic positivity)
7. Clinical Features
| Feature | Detail |
|---|---|
| Symptoms | Chest pain, dyspnea, recurrent pleural effusion |
| Imaging | Pleural thickening, pleural effusion, mediastinal shift toward affected lung |
| Concurrent asbestosis | Present in only 20% of cases (so no fibrosis ≠ no mesothelioma) |
| Spread | Direct invasion → lung, chest wall; hilar nodes → liver |
| Prognosis | Uniformly fatal — 50% die within 12 months; few survive >2 years |
| Treatment | Extrapleural pneumonectomy + chemo + RT (modestly improves survival) |
| Amyloidosis risk | Can complicate persistent cases |
8. Peritoneal Mesothelioma (Quick Note)
- Related to heavy asbestos exposure in 60% of males
- Causes intestinal involvement → death from obstruction or inanition
- Half of cases remain confined to abdominal cavity
9. MASTER MNEMONIC — Everything in One
"ASBESTOS KILLS PLEURA — CAP the Diagnosis"
| Letter | Meaning |
|---|---|
| A | Asbestos = cause (80–90%) |
| S | Smoking does NOT increase risk (unlike lung Ca) |
| B | BAP1 / CDKN2A / NF2 = driver mutations |
| E | Epithelioid (most common type, best prognosis) |
| S | Spreads as pleural RIND (ensheathing the lung) |
| T | Time lag = 25–45 years |
| O | Obliterates pleural space (±effusion) |
| S | Sarcomatoid = worst type |
| C | Calretinin+ (IHC marker) |
| A | AdenoCa mimicry (diagnostic pitfall) |
| P | Poor prognosis — 12–18 months median survival |
Quick Comparison Card
| Feature | Mesothelioma | Lung Adenocarcinoma |
|---|---|---|
| Origin | Mesothelial cells (pleura) | Bronchial epithelium |
| Cause | Asbestos | Smoking |
| Smoking | No synergy | Major risk factor |
| Calretinin IHC | ✅ Positive | ❌ Negative |
| BerEp4 / CEA | ❌ Negative | ✅ Positive |
| Metastasis | Uncommon | Common |
| Prognosis | Worse | Slightly better |
Make a visual poster of the asbestos → mesothelioma pathogenesis timeline
A detailed medical education poster titled "Asbestos to Malignant Mesothelioma: Pathogenesis Timeline". The poster has a dark navy blue background with clean white and colored text. It shows a left-to-right horizontal timeline with the following stages connected by arrows: Stage 1 (Year 0) - labeled "ASBESTOS EXPOSURE": Icon of asbestos fibers (thin needle-like fibers), text says "Occupational inhalation - Shipyard / Mining / Insulation workers", fiber illustration in grey Stage 2 (Weeks-Months) - labeled "FIBER DEPOSITION": Shows fibers traveling down airways, accumulating near the mesothelial cell layer of the pleura, illustrated with a cross-section of lung and pleura Stage 3 (Months-Years) - labeled "ROS GENERATION & DNA DAMAGE": Shows reactive oxygen species (red sparks/lightning bolts) around a cell nucleus, DNA double helix with breaks/mutations marked in red Stage 4 (Years) - labeled "DRIVER MUTATIONS": Three gene boxes in bright colors: - CDKN2A deletion (orange) - "80% of cases - loss of cell cycle control" - NF2 mutation (yellow) - "disrupts cell signaling" - BAP1 mutation (teal) - "DNA repair failure" Stage 5 (25-45 YEARS LATENCY - shown as a long wide arrow spanning below the timeline) - labeled "SILENT INCUBATION - No symptoms for decades" Stage 6 (Year 25-45) - labeled "MALIGNANT MESOTHELIOMA": Shows three histology type boxes: - Epithelioid 60-80% (green box) - Sarcomatoid 10-12% (red box) - Biphasic 10-15% (purple box) Below the histology types: "Pleural RIND ensheathing the lung • Bloody effusion • Chest pain • Dyspnea" Stage 7 (Year 25-47) - labeled "OUTCOME": Red text "MEDIAN SURVIVAL: 12-18 months", "Uniformly fatal" At the bottom, a yellow warning banner: "KEY FACT: Smoking does NOT increase mesothelioma risk (unlike lung carcinoma)" Bottom right corner: Source: Robbins Pathology The poster uses a color scheme of dark navy background, white main text, with orange/red/yellow/teal accent colors for different stages. Clean, professional medical infographic style with icons and minimal illustrations.
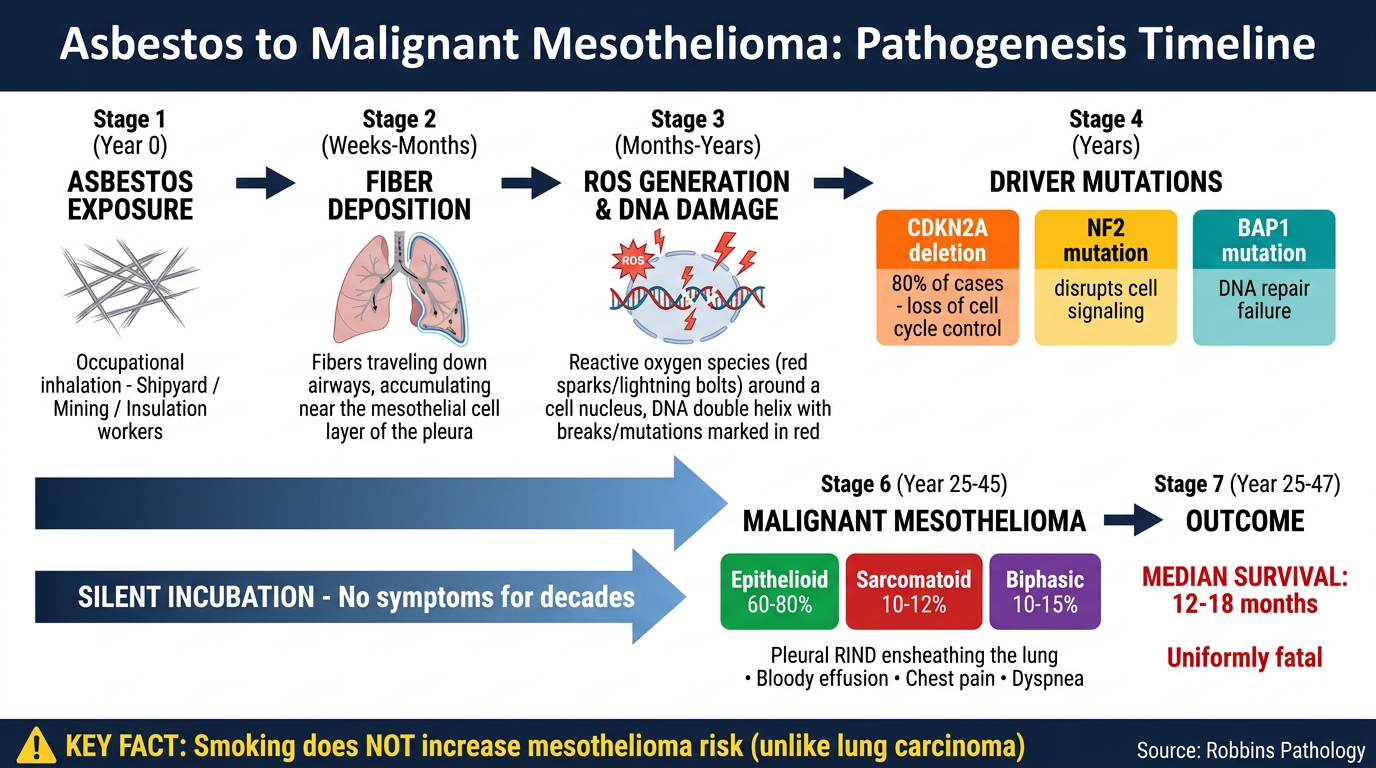
- Year 0 → Asbestos fiber inhalation (occupational exposure)
- Weeks–Months → Fibers deposit near the mesothelial cell layer (never cleared)
- Months–Years → ROS generation → DNA strand breaks
- Years → Driver mutations accumulate: CDKN2A (80%), NF2, BAP1
- 25–45 year silent latency → No symptoms while mutations build up
- Year 25–45 → Malignant Mesothelioma emerges (Epithelioid / Sarcomatoid / Biphasic)
- Outcome → Median survival 12–18 months
Physiology of vomiting
🤢 Physiology of Vomiting — Easy & Complete
Sources: Guyton & Hall Medical Physiology + Ganong's Review of Medical Physiology
THE ONE-LINE ANCHOR
"Stimulus → Afferents → CTZ / Vomiting Center → Motor Output → Squeeze & Expel"
1. Definition
- Excessively irritated
- Overdistended
- Exposed to toxic substances in blood
2. The Two Command Centers
🧠 The "Vomiting Center" (VC)
- Location: Reticular formation of the medulla oblongata (multiple scattered neuron groups — not one discrete nucleus)
- Key components: Nucleus tractus solitarius (NTS), dorsal motor nucleus of vagus
- Receives inputs from all sources (CTZ, gut, vestibular, cortex)
- Sends outputs via cranial nerves V, VII, IX, X, XII + spinal motor nerves → executes the act
🔴 Chemoreceptor Trigger Zone (CTZ)
- Location: Area postrema — floor of 4th ventricle, lateral walls
- Outside the blood-brain barrier → can be directly reached by circulating toxins, drugs, hormones
- CTZ cannot cause vomiting directly — it relays to the Vomiting Center
- Destruction of CTZ blocks drug/toxin-induced vomiting but not GI irritation-induced vomiting
3. Inputs to the Vomiting Center
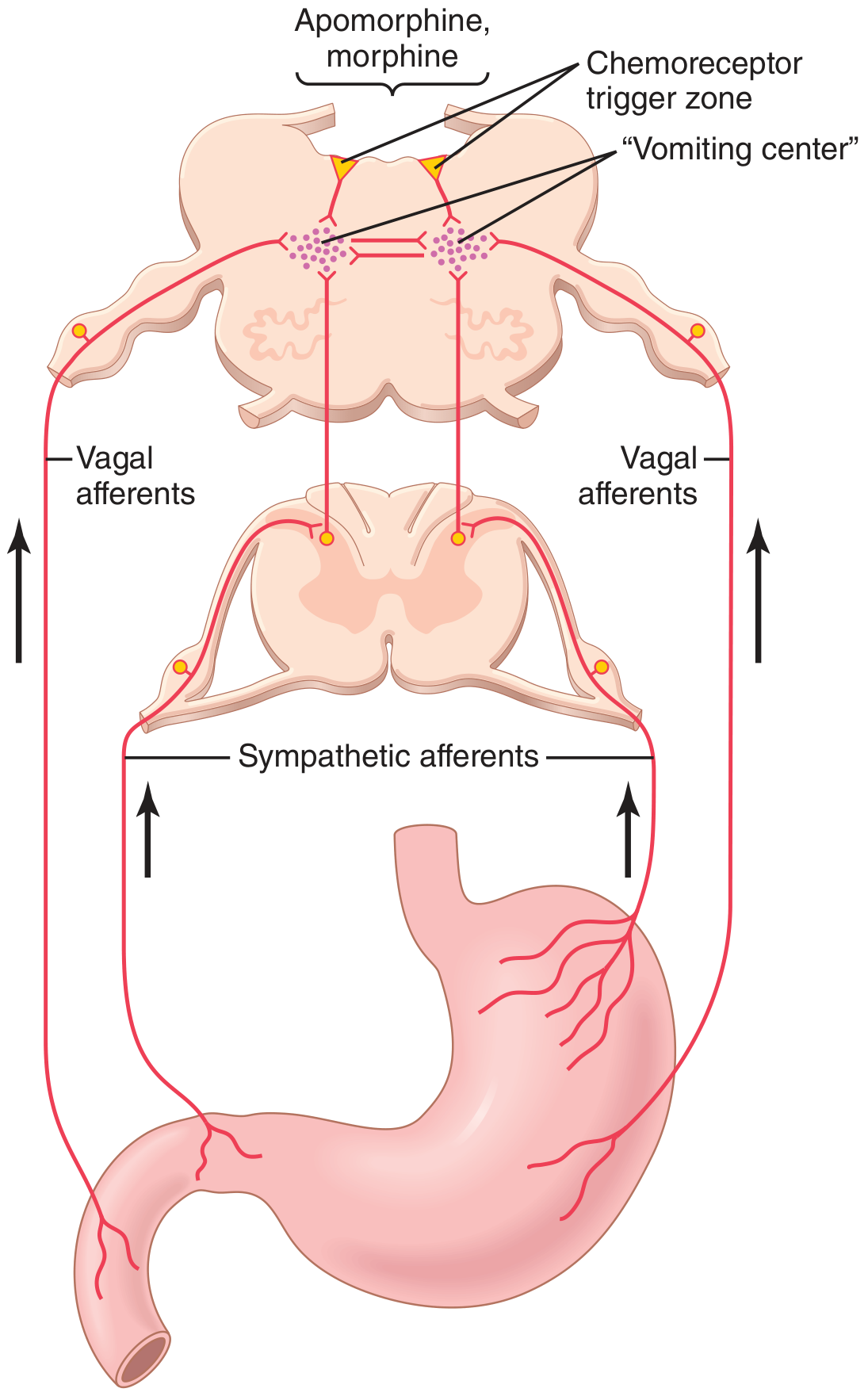
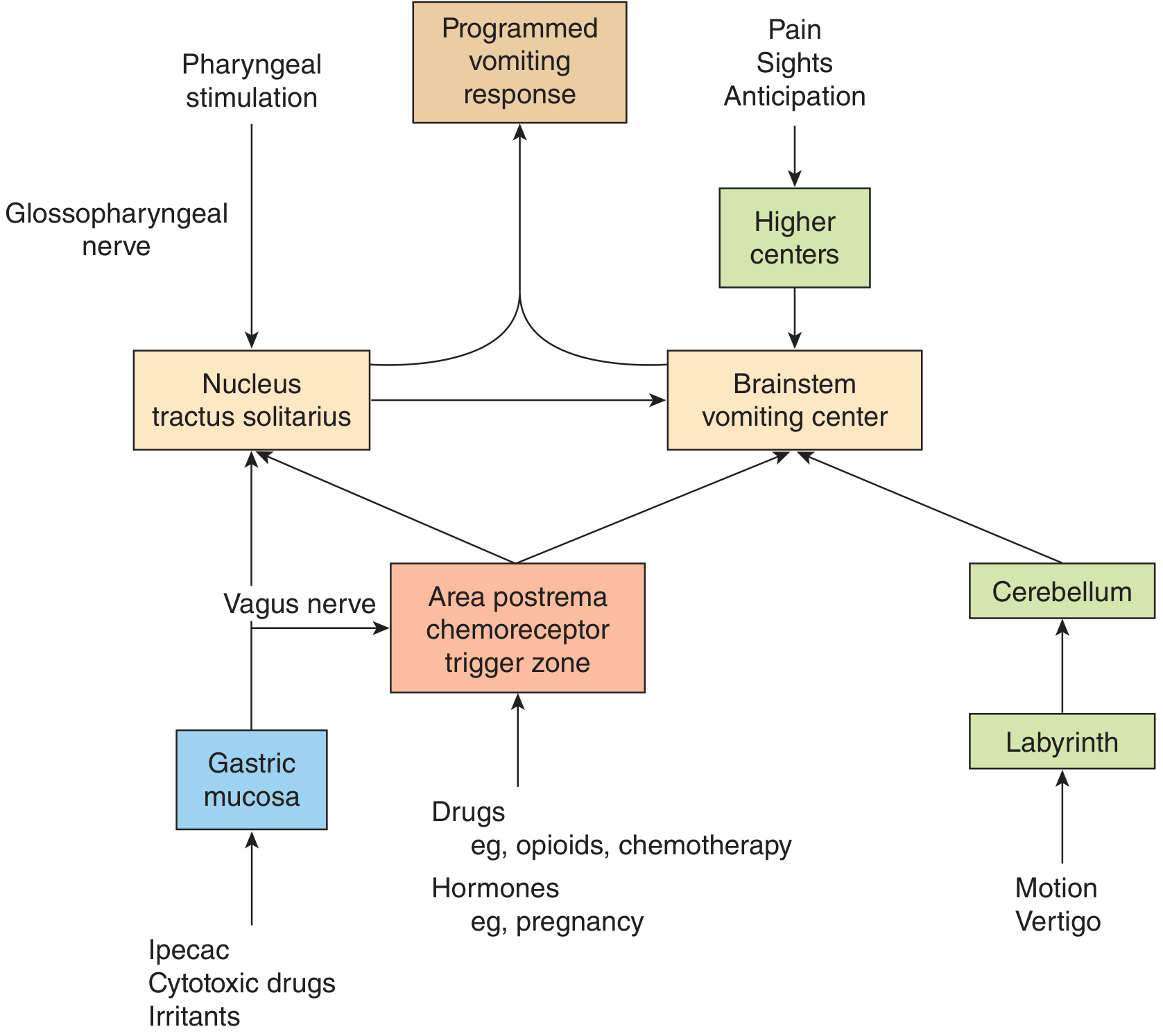
| Source | Pathway | Trigger | Examples |
|---|---|---|---|
| GI mucosa (pharynx, esophagus, stomach, duodenum) | Vagal + sympathetic afferents → NTS → VC | Irritation, distension | Gastroenteritis, pyloric obstruction, ipecac, cytotoxics |
| CTZ (Area postrema) | Blood-borne → CTZ → VC | Drugs, toxins, hormones | Morphine, opioids, digoxin, apomorphine, chemotherapy, pregnancy (HCG) |
| Vestibular labyrinth | CN VIII → vestibular nuclei → cerebellum → CTZ → VC | Motion | Motion sickness, vertigo, labyrinthitis |
| Higher cortical centers (diencephalon + limbic) | Cortex → VC | Emotions, sight, smell, pain, anticipation | Anxiety, disgusting sights, anticipatory nausea |
| Pharyngeal stimulation | CN IX (glossopharyngeal) → NTS → VC | Gag reflex | Finger in throat, post-nasal drip |
4. The Sequence of Events (Step-by-Step)
Phase 1 — Prodrome / Pre-vomiting
- Nausea — conscious recognition of subconscious medullary excitation
- Hypersalivation — to protect dental enamel from acid
- Antiperistalsis begins — peristalsis reverses direction, moving intestinal contents upward at 2–3 cm/sec
- Contents travel from ileum → duodenum → stomach within 3–5 minutes
- Overdistension of duodenum & stomach now triggers the actual vomiting act
Phase 2 — The Vomiting Act (Perfectly Coordinated)
Step 1: DEEP BREATH taken
Step 2: Hyoid bone + larynx RISE → upper esophageal sphincter OPENS
Step 3: GLOTTIS CLOSES → prevents aspiration into lungs
Step 4: SOFT PALATE rises → closes posterior nares (prevents nasal entry)
Step 5: DIAPHRAGM contracts DOWNWARD forcefully
Step 6: ABDOMINAL WALL MUSCLES contract simultaneously
→ stomach squeezed between diaphragm and abdominal wall
→ intragastric pressure skyrockets
Step 7: LOWER ESOPHAGEAL SPHINCTER relaxes completely
Step 8: GASTRIC CONTENTS expelled upward through esophagus and out
5. Motor Output — Which Nerves Execute the Act?
| Nerve | Action |
|---|---|
| CN V (Trigeminal) | Jaw & facial movements |
| CN VII (Facial) | Facial expression changes |
| CN IX (Glossopharyngeal) | Pharyngeal muscles |
| CN X (Vagus) | Esophagus + stomach relaxation + gut motility changes |
| CN XII (Hypoglossal) | Tongue movements |
| Phrenic nerve (C3-C5) | Diaphragm contraction |
| Spinal somatic nerves (T6-L1) | Abdominal wall muscle contraction |
6. Neurotransmitters & Receptors Involved
| Receptor | Location | Relevance |
|---|---|---|
| D₂ (Dopamine) | CTZ (area postrema) | Key target: blocked by metoclopramide, domperidone, haloperidol |
| 5-HT₃ (Serotonin) | Gut enterochromaffin cells + CTZ | Released by chemotherapy → blocked by ondansetron, granisetron |
| H₁ (Histamine) | Vestibular nuclei | Motion sickness → blocked by cyclizine, promethazine |
| M₁ (Muscarinic) | Vestibular-cerebellar pathway | Motion sickness → blocked by hyoscine (scopolamine) |
| NK₁ (Substance P) | Vomiting center | Delayed chemo-vomiting → blocked by aprepitant |
- D₂ blocker → metoclopramide
- 5-HT₃ blocker → ondansetron
- H₁ blocker → cyclizine
- M₁ blocker → hyoscine
- NK₁ blocker → aprepitant
7. Nausea
- Nausea = conscious awareness of subconscious excitation in medullary areas near/part of the vomiting center
- Three main causes: GI irritation, lower brain (motion sickness), cerebral cortex (emotional)
- Vomiting can occur without nausea (projectile vomiting in raised ICP) → only certain parts of VC generate nausea
8. Metabolic Consequences of Vomiting
| Site of Obstruction | What's Lost | Metabolic Effect |
|---|---|---|
| Pyloric (e.g. pyloric stenosis) | HCl + H⁺ from stomach only | Metabolic alkalosis + hypochloremia + hypokalemia |
| Below pylorus (small bowel) | Stomach acid + intestinal base (approximately equal) | Minimal acid-base change, severe dehydration |
| Distal colon | Fecal vomiting — late sign | Profound dehydration |
9. Summary Flow Diagram
STIMULI
├── GI irritation/distension ──→ Vagal/sympathetic afferents
├── Drugs/toxins/hormones ─────→ CTZ (Area Postrema)
├── Motion/vertigo ────────────→ Vestibular → Cerebellum → CTZ
└── Emotions/sight/pain ───────→ Cortex/Limbic system
↓ ↓ ↓
VOMITING CENTER (Medulla — NTS + reticular formation)
↓
MOTOR OUTPUT (CN V, VII, IX, X, XII + phrenic + spinal)
↓
ANTIPERISTALSIS → DISTENSION → VOMITING ACT
(Deep breath → Glottis closed → Abs squeeze → LES open → EXPULSION)
10. MASTER MNEMONIC
"Never Vomit Again Completely — Go Deep, Close All Sphincters"
| Meaning | |
|---|---|
| Never | Nausea = prodrome |
| Vomit | Vomiting center in medulla |
| Again | Antiperistalsis starts first |
| Completely | CTZ = drug/toxin gateway |
| Go | Glottis closes (protection) |
| Deep | Diaphragm + abdominals squeeze |
| Close | Cranial nerves V VII IX X XII |
| All | Alkalosis if pyloric loss |
| Sphincters | Spincter LES relaxes to expel |
Pathology of portal hypertension
🫀 Pathology of Portal Hypertension — Robbins (One Page)
Robbins, Cotran & Kumar Pathologic Basis of Disease, Chapter 18
THE ONE-LINE ANCHOR
"Resistance ↑ + Flow ↑ → Pressure ↑ → 4 Big Consequences: ASHES" Ascites · Shunts (varices) · Hepatic encephalopathy · Enlarged spleen · Syndromic lung complications
1. What Is It?
2. Causes — Three Levels
| Level | Site of Block | Causes |
|---|---|---|
| PREHEPATIC (before liver) | Portal vein itself | Portal vein thrombosis/narrowing; Massive splenomegaly (↑ splenic vein flow) |
| INTRAHEPATIC (inside liver) | Sinusoids | Cirrhosis (commonest cause overall); Schistosomiasis; Massive fatty change; Sarcoidosis; Nodular regenerative hyperplasia; Primary biliary cholangitis; Infiltrative malignancy; Amyloidosis |
| POSTHEPATIC (after liver) | Hepatic veins / heart | Severe right heart failure; Constrictive pericarditis; Budd-Chiari syndrome (hepatic vein outflow obstruction) |
Cirrhosis = dominant cause — accounts for the vast majority of cases
3. Pathophysiology — Two Mechanisms Working Together
┌─────────────────────────────────────────────────────┐
│ PORTAL HYPERTENSION = RESISTANCE ↑ + FLOW ↑ │
└─────────────────────────────────────────────────────┘
Mechanism 1 — Increased Resistance (at sinusoids)
- Contraction of vascular smooth muscle cells & myofibroblasts in sinusoidal walls
- Scarring (fibrosis) distorts and compresses sinusoids
- Parenchymal regenerative nodules physically block blood flow
- ↓ Nitric oxide (NO) production by sinusoidal endothelial cells → vasoconstriction
- ↑ Endothelin-1, angiotensinogen, eicosanoids → further vasoconstriction
- Arterial–portal anastomoses in fibrous septa impose high arterial pressure onto low-pressure portal system
Mechanism 2 — Increased Portal Blood Flow (hyperdynamic circulation)
- Splanchnic arterial vasodilation (gut arteries dilate)
- Key mediator: Nitric Oxide (NO) — paradoxically, NO is ↓ intrahepatic but ↑ in splanchnic vessels
- Also: prostacyclin, TNF-α
- More blood flows into intestines → more venous return → ↑ portal venous inflow
4. The Four Major Consequences
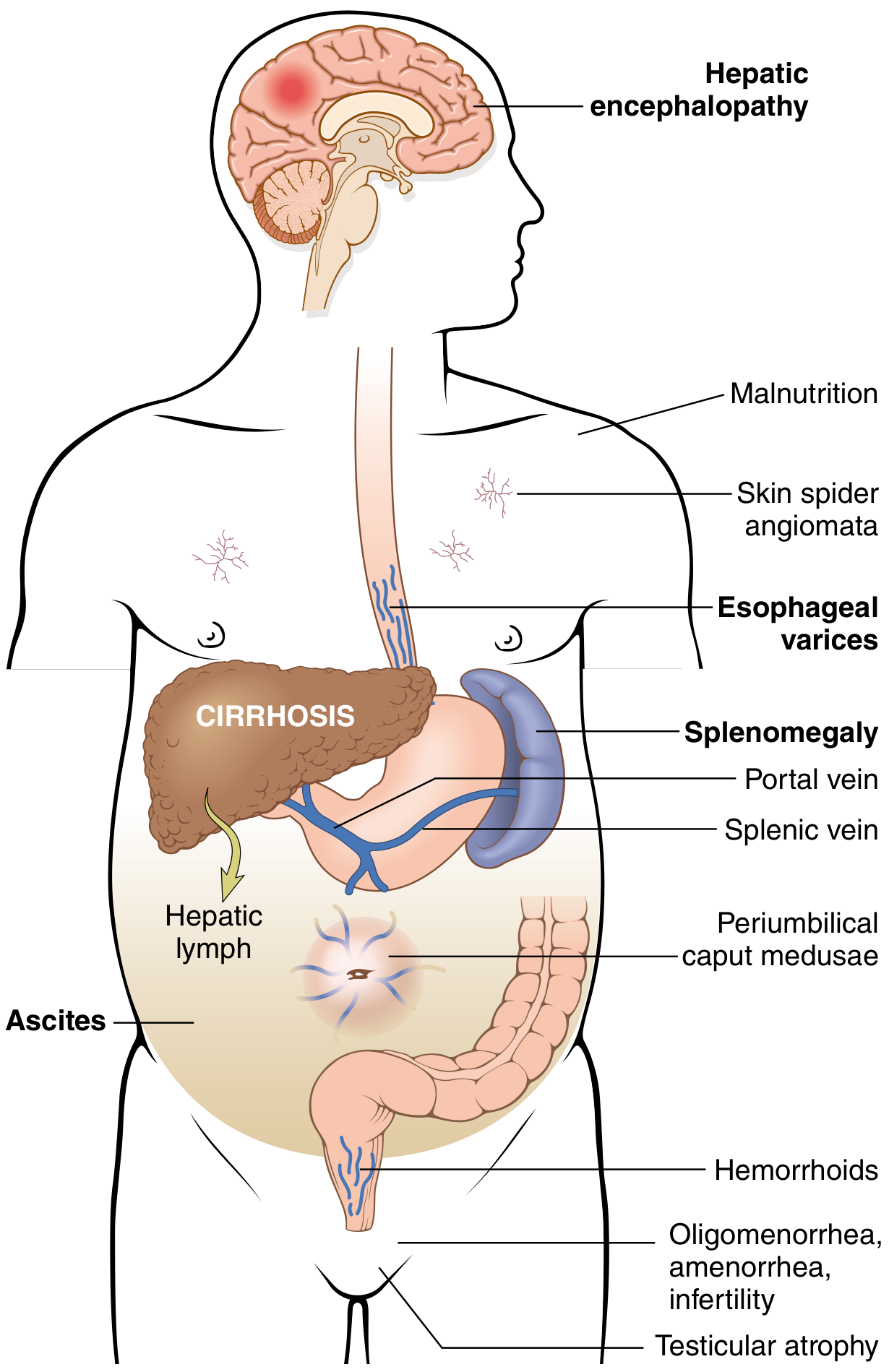
① ASCITES
- Definition: Accumulation of serous fluid in the peritoneal cavity
- Detectable clinically when ≥ 500 mL has accumulated
- 85% caused by cirrhosis
- Fluid characteristics: protein < 3 g/dL, mostly albumin; SAAG ≥ 1.1 g/dL (serum-ascites albumin gradient)
- SAAG ≥ 1.1 = portal hypertension; SAAG < 1.1 = other cause (malignancy, TB)
- Cell content: scant mesothelial cells + mononuclear leukocytes
- Neutrophils → spontaneous bacterial peritonitis (SBP)
- Red cells → intraabdominal malignancy
- Long-standing ascites → seepage through diaphragmatic lymphatics → right-sided hydrothorax
Sinusoidal hypertension
↓
↑ Hepatic lymph formation
↓
↓ Oncotic pressure (hypoalbuminemia — liver can't make albumin)
↓
Splanchnic vasodilation → ↓ effective circulating volume
↓
RAAS activated → Na+ and water retention
↓
ASCITES
② PORTOSYSTEMIC VENOUS SHUNTS (Varices)
| Site | Anastomosis | Clinical Manifestation |
|---|---|---|
| Esophagogastric junction | Left gastric vein ↔ azygos vein | Esophageal varices ⚠️ |
| Periumbilical / anterior abdominal wall | Paraumbilical vein ↔ epigastric veins | Caput medusae (dilated veins radiating from umbilicus) |
| Rectum | Superior rectal vein ↔ middle/inferior rectal veins | Hemorrhoids |
| Retroperitoneum | Retroperitoneal collaterals | Usually clinically silent |
- Present in ~40% of patients with advanced cirrhosis
- Cause massive hematemesis (vomiting blood)
- Death in ~50% of those affected
- Each bleeding episode = 30% mortality
- Varices are thin-walled, high-pressure, submucosal — rupture causes exsanguinating hemorrhage
③ HEPATIC ENCEPHALOPATHY
- Brain dysfunction due to liver failure + portosystemic shunting
- Shunted blood bypasses hepatic detoxification → ammonia, mercaptans, false neurotransmitters reach brain
- Spectrum: mild confusion → stupor → hepatic coma
- Asterixis (flapping tremor) = classic sign
- Precipitants: GI bleed, infection, dehydration, high protein intake, sedatives
- (Detailed discussion under Liver Failure — Robbins)
④ CONGESTIVE SPLENOMEGALY
- Longstanding portal HTN → back-pressure in splenic vein → splenic congestion
- Spleen can reach up to 1000 g (normal ~150 g = 5–6× normal)
- Hypersplenism = enlarged spleen sequesters blood elements
- Thrombocytopenia (most common) — platelet destruction
- Pancytopenia in severe cases — anemia + leukopenia + thrombocytopenia
- Degree of splenomegaly does NOT correlate directly with severity of portal HTN
5. Pulmonary Complications (Bonus — Robbins Adds These)
Hepatopulmonary Syndrome (HPS)
- Occurs in up to 30% of cirrhosis + portal HTN patients
- Dilation of intrapulmonary capillaries and precapillary vessels (up to 500 μm!)
- Blood shunts right-to-left through dilated vessels → ventilation-perfusion mismatch → hypoxemia
- Orthodeoxia = hypoxemia worsens in upright position (gravity pulls blood to dilated lower lobe vessels)
- Mechanism: diseased liver fails to clear endothelin-1 → stimulates endothelial NO production → pulmonary vasodilation
Portopulmonary Hypertension
- Portal HTN → ↑ pressure in pulmonary arterial system
- Mechanism: vasoactive substances bypass the liver, reach pulmonary circulation
- Causes pulmonary arterial hypertension → right heart failure
6. Other Systemic Features of Chronic Liver Disease / Portal HTN
| Feature | Mechanism |
|---|---|
| Spider angiomata | ↑ Estrogens (liver can't metabolize them) → cutaneous arteriolar dilation |
| Gynecomastia / testicular atrophy | ↑ Estrogens |
| Oligomenorrhea / amenorrhea / infertility (females) | Hypogonadism from hormonal imbalance |
| Malnutrition | Poor hepatic synthetic function |
| Jaundice | Hepatocellular failure |
| Coagulopathy | ↓ Clotting factors (liver makes all except vWF) |
7. Summary Flow Diagram
CAUSE (Cirrhosis > Prehepatic > Posthepatic)
↓
↑ Resistance at sinusoids + ↑ Splanchnic flow (NO ↑)
↓
PORTAL PRESSURE ↑ (> 10–12 mmHg = clinically significant)
↓
┌─────┬──────┬──────┬────────────┐
↓ ↓ ↓ ↓ ↓
ASCITES SHUNTS SPLENO- HEPATIC PULMONARY
↓ MEGALY ENCEPHALO- (HPS / PPH)
Varices → ↓ PATHY
BLEED Hypersplenism
(30% mortality
per episode)
8. MASTER MNEMONIC
"CIRRHOSIS CAUSES A VASH"
| Letter | Meaning |
|---|---|
| CIRRHOSIS | Commonest cause (intrahepatic) |
| CAUSES | |
| Ascites | SAAG ≥ 1.1, < 3g/dL protein |
| Varices | Esophageal = most dangerous, 30% mortality/bleed |
| Astenixis | Hepatic encephalopathy |
| Splenomegaly | → Hypersplenism → thrombocytopenia |
| Hyperdynamic | Splanchnic vasodilation (NO↑) drives flow up |
Provide me pathogenensis of calculous and acalculous acute cholecystitis in flowchart form in easy language
🫙 Pathogenesis of Acute Cholecystitis — Flowcharts
Source: Robbins & Kumar Basic Pathology + Robbins, Cotran & Kumar Pathologic Basis of Disease
PART 1 — ACUTE CALCULOUS CHOLECYSTITIS (90% of cases)
Cause = Gallstone blocking the exit of the gallbladder
┌─────────────────────────────────────────────────────────┐
│ GALLSTONE forms in gallbladder (due to supersaturated │
│ bile — too much cholesterol, too little bile salts) │
└──────────────────────┬──────────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────────────┐
│ Stone LODGES in the gallbladder NECK or CYSTIC DUCT │
│ ➜ Bile CANNOT flow out │
│ ➜ Gallbladder becomes DISTENDED (blown up like balloon)│
└──────────────────────┬──────────────────────────────────┘
│
▼
╔══════ 4 CHEMICAL INJURY MECHANISMS ══════╗
║ ║
║ 1. PHOSPHOLIPASES activated ║
║ ➜ Mucosal enzymes break down ║
║ lecithin (a bile component) ║
║ ➜ Toxic LYSOLECITHIN is produced ║
║ ➜ Poisons gallbladder lining ║
║ ║
║ 2. MUCOUS LAYER DESTROYED ║
║ ➜ Normally, a protective mucus ║
║ coat lines the gallbladder wall ║
║ ➜ Bile salts (normally safe) ║
║ now directly attack exposed ║
║ mucosal cells (detergent effect) ║
║ ║
║ 3. PROSTAGLANDINS released ║
║ ➜ Distension triggers PG release ║
║ ➜ Amplify inflammation in the wall ║
║ ║
║ 4. ISCHEMIA (blood flow cut off) ║
║ ➜ High intraluminal pressure ║
║ compresses mucosal blood vessels ║
║ ➜ Mucosa gets starved of oxygen ║
╚══════════════════════════════════════════╝
│
│ ⚠️ NOTE: Bacteria NOT involved yet
│ (this is purely chemical inflammation)
▼
┌─────────────────────────────────────────────────────────┐
│ ACUTE INFLAMMATION of gallbladder wall │
│ • Wall becomes thickened, edematous, red │
│ • Fibrinous exudate on outer surface │
│ • Bile inside becomes turbid / pus-filled │
└──────────────────────┬──────────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────────────┐
│ BACTERIA (E. coli, Klebsiella) may SECONDARILY INVADE │
│ ➜ Makes inflammation much worse │
│ ➜ Pus fills the gallbladder = EMPYEMA │
└──────────────────────┬──────────────────────────────────┘
│
▼
┌────────────┴────────────┐
│ │
▼ ▼
If wall dies If it perforates
= GANGRENOUS = PERFORATION
CHOLECYSTITIS ➜ Bile peritonitis
(green-black wall) (surgical emergency!)
PART 2 — ACUTE ACALCULOUS CHOLECYSTITIS (5–12% of cases)
Cause = NO stone — instead, ISCHEMIA + STASIS kills the gallbladder Typical patient = severely ill, ICU patient
┌─────────────────────────────────────────────────────────────┐
│ PREDISPOSING CONDITIONS (patient is already critically ill)│
│ │
│ • Major surgery (e.g., cardiac, abdominal) │
│ • Severe trauma (car accident, polytrauma) │
│ • Severe burns │
│ • Sepsis with hypotension / multi-organ failure │
│ • Diabetes mellitus │
│ • Immunosuppression │
└──────────────────────┬──────────────────────────────────────┘
│
┌───────────┴────────────┐
▼ ▼
┌──────────────────┐ ┌──────────────────────────────┐
│ ISCHEMIA │ │ GALLBLADDER STASIS │
│ │ │ │
│ Cystic artery = │ │ No food intake (NPO) │
│ END ARTERY │ │ ➜ Gallbladder never empties │
│ (no backup │ │ ➜ Bile thickens into SLUDGE │
│ blood supply!) │ │ (microcrystals of │
│ │ │ cholesterol + viscous bile)│
│ + Low BP/sepsis │ │ ➜ Sludge BLOCKS cystic duct │
│ ➜ Blood flow │ │ (obstruction without stone)│
│ drops to zero │ │ │
└────────┬─────────┘ └────────────┬─────────────────┘
│ │
└─────────────┬───────────────┘
│
▼
┌─────────────────────────────────────────────────────────────┐
│ Gallbladder wall INFLAMED and EDEMATOUS │
│ ➜ Edema further compresses blood vessels in wall │
│ ➜ WORSENS ischemia (vicious cycle!) │
└──────────────────────┬──────────────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────────────────┐
│ ACUTE ACALCULOUS CHOLECYSTITIS │
│ (same morphology as calculous — just NO stone!) │
│ • Thickened, red, edematous wall │
│ • Turbid bile │
│ • Fibrinous exudate │
└──────────────────────┬──────────────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────────────────┐
│ ⚠️ HIGH MORTALITY — because underlying illness is severe │
│ Complications: Gangrene, Perforation, Empyema │
│ Bacteria (Clostridia, Coliforms) → Emphysematous │
│ cholecystitis (gas in wall — seen on imaging!) │
└─────────────────────────────────────────────────────────────┘
SIDE-BY-SIDE COMPARISON TABLE
| Feature | Calculous | Acalculous |
|---|---|---|
| Frequency | 90% of acute cholecystitis | 5–12% |
| Stone present? | ✅ Yes — blocks cystic duct/neck | ❌ No stone |
| Primary mechanism | Chemical injury from trapped bile | Ischemia + stasis |
| Who gets it? | Anyone with gallstones | Critically ill ICU patients |
| Key trigger | Stone obstruction | Low BP / sepsis / major surgery |
| Bacteria involved? | Secondary (late) | Secondary (late) |
| Cystic artery | Not the main issue | Key — it's an END artery, no backup |
| Morphology | Same (stone present) | Same (no stone) |
| Prognosis | Usually good with surgery | HIGH mortality |
THE ONE-PAGE MEMORY TRICK
Calculous = "BLOCK then BURN"
Stone BLOCKS the exit → Bile BURNS the wall (lysolecithin + bile salts)
Acalculous = "SICK + STARVE"
Patient is SICK (ICU) → Gallbladder STARVES (ischemia from end artery) + STAGNATES (sludge from NPO)
Morphology Quick Summary (Both Types Look the Same!)
| Finding | What It Means |
|---|---|
| Enlarged, tense, red GB | Acute inflammation + distension |
| Violaceous / green-black color | Subserosal hemorrhage → Gangrene |
| Fibrinous exudate on outer wall | Inflammation extending to serosa |
| Turbid / pus-filled bile | Empyema of gallbladder |
| Gas in the wall (on X-ray/CT) | Emphysematous cholecystitis (Clostridia) |
| Perforation | Bile peritonitis — surgical emergency |
athogenesis: The obstruction causes chemical irritation when mucosal phospholipases hydrolyze luminal lecithins into toxic lysolecithins, which disrupt the protective glycoprotein mucus layer. This exposes the mucosal epithelium to the detergent action of bile salts. Subsequent distension and increased intraluminal pressure compromise blood flow to the mucosa ... make this in flowchart
🫙 Pathogenesis of Acute Calculous Cholecystitis — Flowchart
┌──────────────────────────────────────────────────────┐
│ GALLSTONE blocks Cystic Duct / GB Neck │
│ ➜ Bile CANNOT flow out │
└─────────────────────┬────────────────────────────────┘
│
▼
┌──────────────────────────────────────────────────────┐
│ BILE TRAPPED inside gallbladder │
│ ➜ Stagnant bile activates mucosal enzymes │
└─────────────────────┬────────────────────────────────┘
│
▼
┌──────────────────────────────────────────────────────┐
│ STEP 1 — PHOSPHOLIPASE ACTIVATION │
│ │
│ Mucosal phospholipases (mucosal enzymes) are │
│ activated by the stagnant bile │
│ ↓ │
│ They hydrolyze LECITHIN (a normal bile component) │
│ ↓ │
│ Produce LYSOLECITHIN — a TOXIC compound │
└─────────────────────┬────────────────────────────────┘
│
▼
┌──────────────────────────────────────────────────────┐
│ STEP 2 — MUCUS LAYER DESTROYED │
│ │
│ Lysolecithin attacks and DISRUPTS the protective │
│ glycoprotein MUCUS LAYER lining the GB wall │
│ ↓ │
│ The mucosal epithelium is now BARE and EXPOSED │
└─────────────────────┬────────────────────────────────┘
│
▼
┌──────────────────────────────────────────────────────┐
│ STEP 3 — BILE SALTS ATTACK DIRECTLY │
│ │
│ Normally, the mucus coat shields the wall from │
│ bile salts (which are detergents / soaps) │
│ ↓ │
│ With the mucus GONE, bile salts now act directly │
│ on the naked epithelial cells │
│ ➜ DETERGENT ACTION = dissolves cell membranes │
│ ➜ Direct chemical injury to mucosa │
└─────────────────────┬────────────────────────────────┘
│
▼
┌──────────────────────────────────────────────────────┐
│ STEP 4 — DISTENSION & PRESSURE BUILD-UP │
│ │
│ Trapped bile accumulates │
│ ➜ Gallbladder DISTENDS (swells up) │
│ ➜ Intraluminal pressure RISES │
│ ↓ │
│ High pressure COMPRESSES blood vessels │
│ in the gallbladder wall mucosa │
│ ➜ Blood flow to the mucosa is COMPROMISED │
│ ➜ Mucosal ISCHEMIA begins │
└─────────────────────┬────────────────────────────────┘
│
▼
┌──────────────────────────────────────────────────────┐
│ STEP 5 — PROSTAGLANDINS AMPLIFY INFLAMMATION │
│ │
│ Distension of the wall triggers release of │
│ PROSTAGLANDINS (inflammatory mediators) │
│ ➜ Further amplify mucosal & mural inflammation │
│ ➜ Pain, fever, tenderness worsen │
└─────────────────────┬────────────────────────────────┘
│
│ ⚠️ All steps above are CHEMICAL —
│ NO BACTERIA yet at this stage
▼
┌──────────────────────────────────────────────────────┐
│ ACUTE CHEMICAL CHOLECYSTITIS │
│ • GB wall: thickened, edematous, hyperemic (red) │
│ • Bile: turbid / cloudy │
│ • Serosa: fibrinous exudate │
└─────────────────────┬────────────────────────────────┘
│
▼
┌──────────────────────────────────────────────────────┐
│ STEP 6 — SECONDARY BACTERIAL SUPERINFECTION │
│ (happens LATER in the course) │
│ │
│ E. coli, Klebsiella, Enterococcus invade │
│ the already-damaged wall │
│ ➜ Superimposed bacterial inflammation │
│ ➜ Exacerbates the process │
└─────────────────────┬────────────────────────────────┘
│
┌───────┴────────┐
▼ ▼
┌─────────────────┐ ┌─────────────────────────┐
│ EMPYEMA │ │ GANGRENOUS/EMPHYSEMA- │
│ GB lumen full │ │ TOUS CHOLECYSTITIS │
│ of pus │ │ Wall necrosis, gas │
└─────────────────┘ │ (Clostridia) → risk of │
│ PERFORATION │
└─────────────────────────-┘
Summary in 6 Words Per Step
| Step | What Happens |
|---|---|
| 1 | Phospholipase converts lecithin → lysolecithin (toxic) |
| 2 | Lysolecithin destroys the protective mucus layer |
| 3 | Bile salts attack exposed epithelium (detergent effect) |
| 4 | Distension → ↑ pressure → mucosal ischemia |
| 5 | Prostaglandins released → amplify inflammation |
| 6 | Bacteria invade secondarily → empyema / gangrene |
Key Robbins Point: Steps 1–5 are entirely chemical — bacteria play no role until later. This is why the disease can start and progress even in a sterile environment.
https://youtu.be/00jgSl0FHNE?si=CjXDXBifgRsUb8wS
- 📝 If it's a medical lecture — tell me the topic and I'll give you a full Robbins-based summary with flowcharts and mnemonics
- 🔍 If you want me to look up the video topic — share the title or subject and I'll research it
- 📖 If you have notes from the video — paste them and I'll organize/expand them
I want prper flowchart of development of respiratory system
Generate a comprehensive flowchart of respiratory system development