Explain invasion and metastasis refer robbins pathology
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Excellent - I now have very rich content and both key diagrams. I have all I need to construct a comprehensive, well-structured answer. Let me now compile the full explanation.
Invasion and Metastasis - Robbins Pathology
Invasion and metastasis are the major causes of cancer-related morbidity and mortality and represent the defining hallmarks of malignant tumors. They involve complex interactions between cancer cells, stromal cells, and the extracellular matrix (ECM). The entire process - called the metastatic cascade - is broken into two broad phases:
- Invasion of the ECM
- Vascular dissemination, tissue homing, and colonization
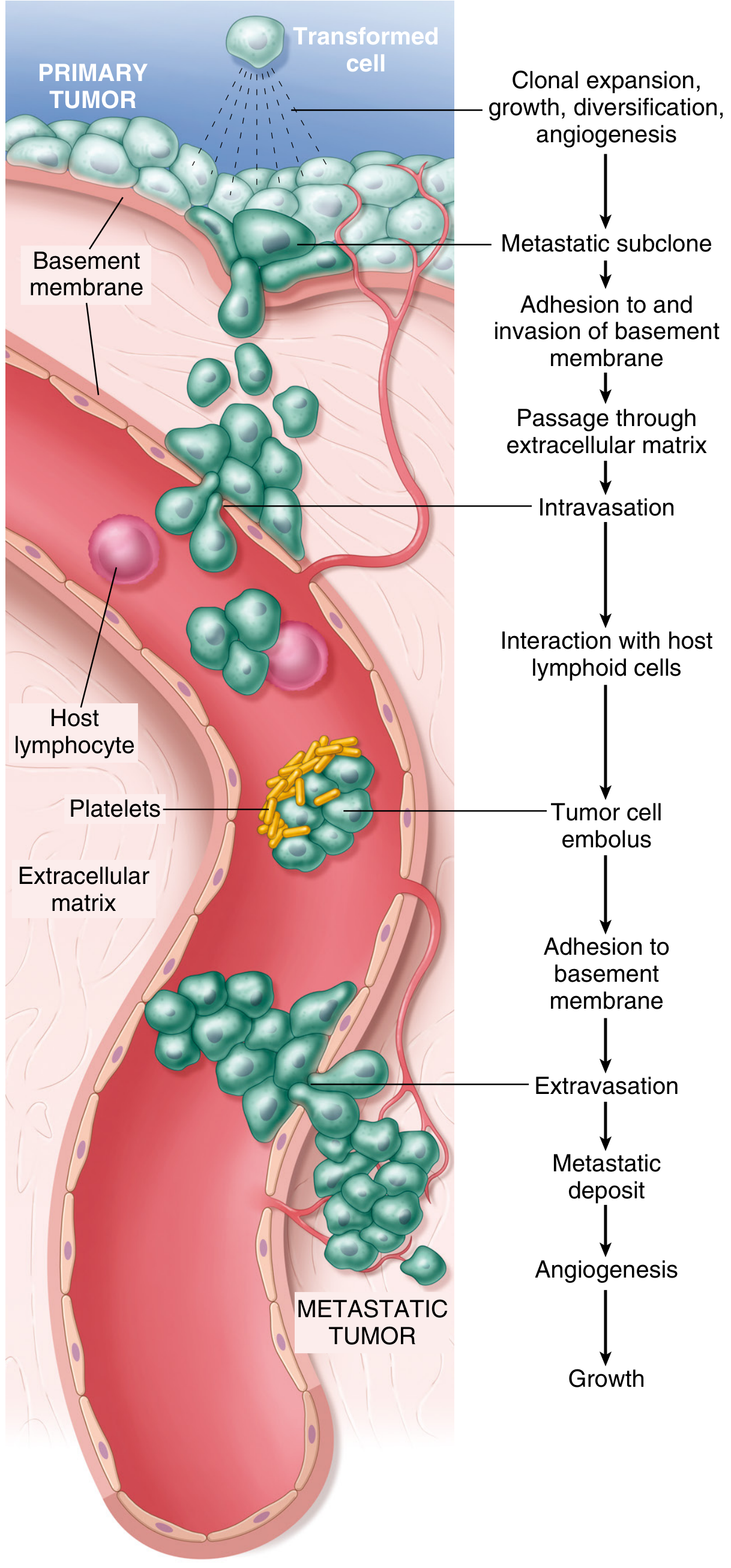
Fig. 7.36 - The metastatic cascade (Robbins, Cotran & Kumar Pathologic Basis of Disease)
Phase 1: Invasion of the Extracellular Matrix
Normal tissues are organized into compartments separated by two types of ECM: basement membranes and interstitial connective tissue, both composed of collagens, glycoproteins, and proteoglycans.
For a carcinoma to metastasize, it must:
- Breach the underlying basement membrane
- Traverse the interstitial connective tissue
- Penetrate the vascular basement membrane to enter circulation
This entire process reverses at the distant site during extravasation.
Invasion of the ECM proceeds through four sequential steps:
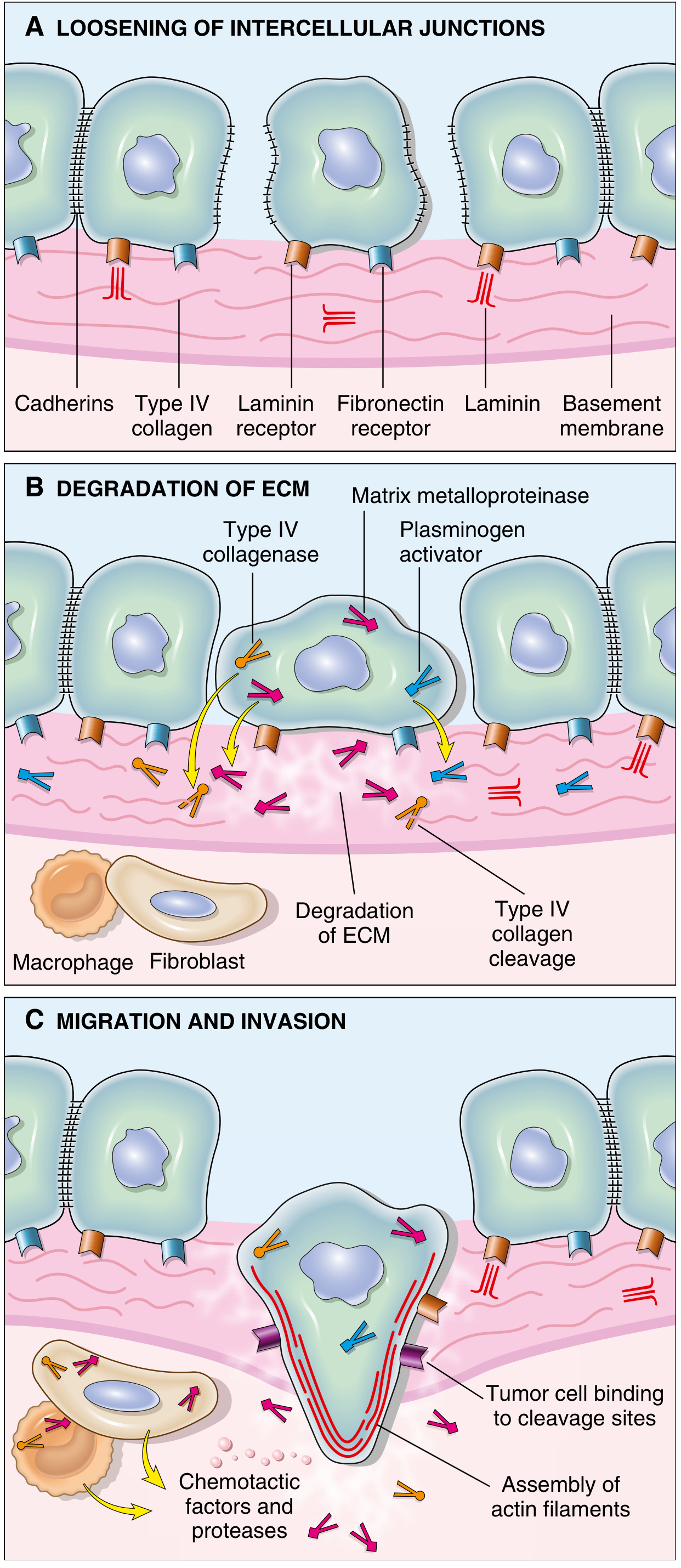
Fig. 7.37 - Invasion of epithelial basement membranes by tumor cells (Robbins, Cotran & Kumar)
Step 1 - Loosening of Tumor Cell-Tumor Cell Interactions
Normal epithelial cells are glued together by E-cadherin, a transmembrane glycoprotein that mediates homotypic adhesion. E-cadherin also relays antigrowth signals by sequestering beta-catenin.
In cancer, E-cadherin function is lost by:
- Mutational inactivation of E-cadherin genes
- Activation of beta-catenin genes
- Epithelial-Mesenchymal Transition (EMT) - controlled by transcription factors SNAIL and TWIST, which suppress E-cadherin expression
EMT is defined not only by downregulation of epithelial markers (E-cadherin) but also by upregulation of mesenchymal markers (vimentin, smooth muscle actin), promoting a pro-migratory phenotype. EMT is especially implicated in breast and prostate cancer metastasis.
Step 2 - Degradation of the Basement Membrane and Interstitial Matrix
Tumor cells accomplish ECM degradation either by secreting proteolytic enzymes themselves, or by inducing stromal cells (fibroblasts, inflammatory cells) to do so.
Key proteases involved:
- Matrix Metalloproteinases (MMPs) - especially MMP-9 (gelatinase), which cleaves Type IV collagen of the basement membrane
- Cathepsin D
- Urokinase plasminogen activator
MMPs do more than just degrade - they also:
- Release VEGF sequestered within the ECM (promoting angiogenesis)
- Generate chemotactic fragments from ECM glycoproteins
- Create angiogenic and growth-promoting cleavage products
Benign tumors have little MMP-9 activity, while their malignant counterparts overexpress it. Simultaneously, concentrations of metalloproteinase inhibitors (TIMPs) are reduced in many cancers, further tilting the balance toward tissue degradation.
Step 3 - Attachment to Novel ECM Components
After degradation, new ECM components are exposed. Tumor cells show complex changes in integrin expression - shifting from integrins that maintain normal tissue architecture to integrins that favor migration.
Key attachment interactions:
- Laminin receptors on tumor cells bind to laminin in the basement membrane - these are overexpressed in many aggressive carcinomas
- Fibronectin receptors facilitate attachment to interstitial matrix
The newly cleaved ECM fragments serve as binding tracks that guide tumor cell movement.
Step 4 - Migration and Invasion of Tumor Cells
Tumor cell locomotion is propelled by:
- Autocrine motility factors secreted by tumor cells themselves
- Paracrine factors from stromal/inflammatory cells (chemotactic gradients)
- Cleavage products of ECM components (collagen, laminin fragments) which are chemotactic
- Growth factors like IGF-I and IGF-II released from degraded ECM
Movement requires assembly of actin filaments at the leading edge of the migrating cell. Cells track along binding sites created by ECM cleavage.
Phase 2: Vascular Dissemination, Tissue Homing, and Colonization
Once tumor cells invade through the ECM, they enter the vasculature and face a new set of challenges.
Intravasation and Circulation
- Tumor cells enter blood vessels or lymphatics
- In the circulation, they are vulnerable to immune destruction (NK cells, T cells)
- They may form tumor cell emboli protected by aggregates of platelets and fibrin - this shields them from immune attack
- Most circulating tumor cells are destroyed; only rare cells produce metastases, explaining why the metastatic process is highly inefficient
Arrest and Extravasation
- Tumor cells arrest in the first capillary bed encountered - most commonly lungs and liver
- Liver is the first capillary bed for portal venous drainage
- Lungs are the first capillary bed for systemic venous drainage
- Once arrested, cells adhere to the vascular endothelium (via adhesion molecules) and then extravasate using the same mechanisms as intravasation
Organ Tropism
Some tumors show non-anatomic organ tropism not explained by circulatory patterns alone. This is explained by:
- Expression of chemokine receptors on tumor cells whose ligands are expressed by endothelial cells at the target site
- Example: Breast cancer cells express CXCR4, whose ligand CXCL12 (SDF-1) is abundantly expressed in lungs, liver, and bone marrow
- Expression of specific adhesion molecules on target organ endothelium
Classic examples of organ tropism:
- Prostate cancer - bone
- Breast cancer - lung, liver, bone, brain
- Colon cancer - liver
- Neuroblastoma - adrenal/liver
Colonization - Formation of Macroscopic Metastases
This is arguably the most difficult step and explains why many circulating tumor cells fail to produce overt metastases:
- Tumor cells first form micrometastases
- To grow into macroscopic tumors, they must adapt to a foreign microenvironment
- This requires:
- Evasion of local immune responses
- Induction of angiogenesis at the new site
- Modulation of stromal cells in the new niche
- Possible dormancy - micrometastases may remain dormant for years before reactivating
The reason individual "metastasis genes" have not been found is that the metastatic phenotype likely requires accumulation of multiple genetic and epigenetic changes. Evidence also suggests that metastases may arise from cells that migrate as cohesive groups (collective migration), with each subclone providing complementary functions.
Summary Table
| Phase | Step | Key Molecules |
|---|---|---|
| ECM Invasion | Loosening of cell-cell contacts | E-cadherin loss, SNAIL, TWIST, EMT |
| ECM Invasion | ECM degradation | MMPs (MMP-9), cathepsin D, urokinase |
| ECM Invasion | Attachment to remodeled ECM | Integrins, laminin receptors, fibronectin receptors |
| ECM Invasion | Migration | Autocrine motility factors, chemotactic ECM fragments, actin assembly |
| Vascular Spread | Intravasation | Platelet-fibrin emboli protection |
| Vascular Spread | Organ tropism | CXCR4/CXCL12, tissue-specific adhesion molecules |
| Vascular Spread | Colonization | Angiogenesis (VEGF), microenvironment adaptation |
Why is Metastasis so Inefficient?
Despite millions of tumor cells entering the bloodstream daily, very few produce metastases. The barriers include:
- Mechanical destruction in the circulation
- Immune attack by NK cells and CTLs
- Failure to adhere and extravasate successfully
- Inability to adapt to a foreign microenvironment
- Failure to induce angiogenesis at the new site
Each step in the cascade must be successfully completed - and most breakaway cells fail at one or more of these checkpoints.
Sources:
- Robbins & Kumar Basic Pathology (Robbins Pathology), Chapter 6 - Neoplasia
- Robbins, Cotran & Kumar Pathologic Basis of Disease, Chapter 7 - Neoplasia
This is a shared conversation. Sign in to Orris to start your own chat.