Acrt and avnrt
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Loading Image
Avrt and avnrt
I have all the information needed from the previous research. Here is a comprehensive comparison of AVRT and AVNRT.
AVNRT and AVRT - Supraventricular Tachycardias
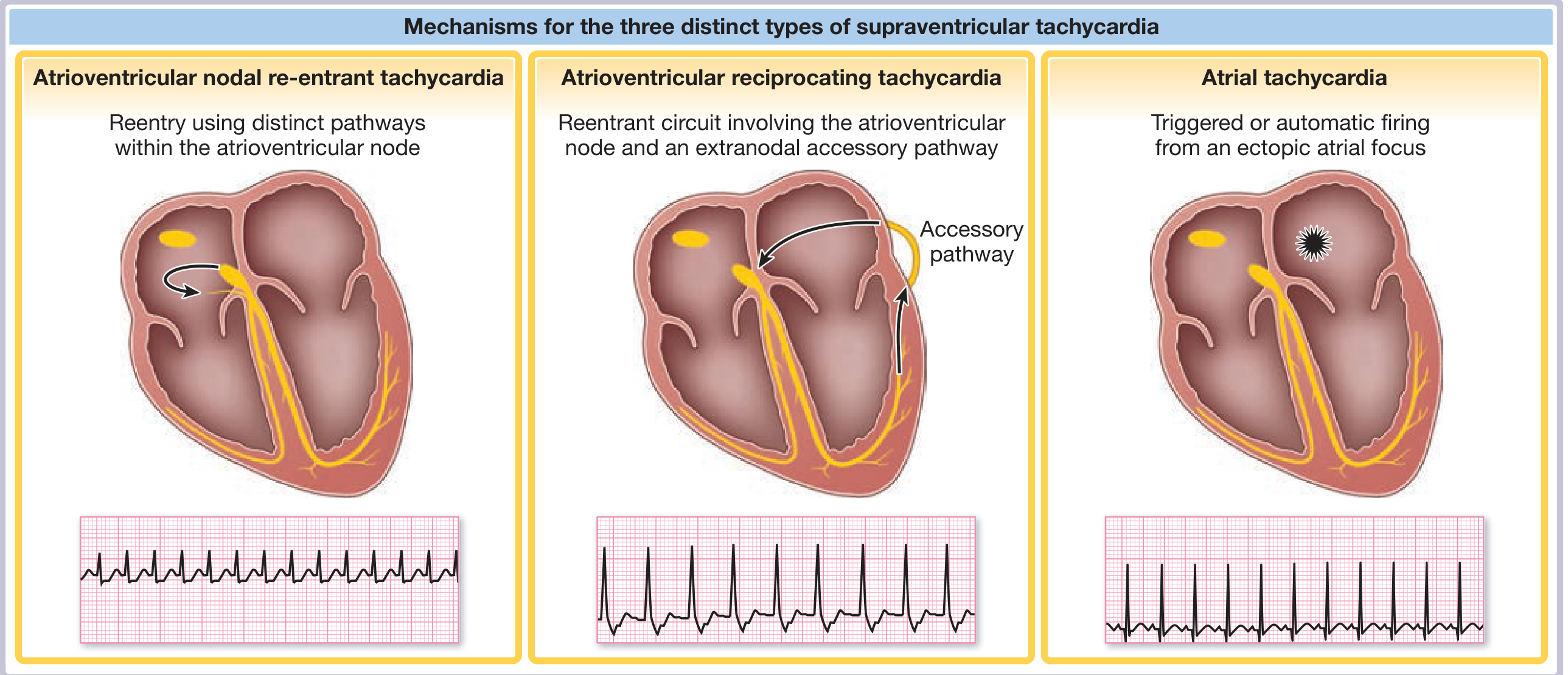
Three mechanisms of SVT: AVNRT (left), AVRT (center), Atrial Tachycardia (right) - Fuster and Hurst's The Heart, 15th Ed.
Overview
Both AVNRT and AVRT are reentrant paroxysmal SVTs (PSVT). Together they account for ~95% of all PSVT cases.
| Feature | AVNRT | AVRT |
|---|---|---|
| Proportion of PSVT | ~65-70% | ~25-30% |
| Mechanism | Reentry within the AV node (dual pathways) | Macro-reentry using AV node + accessory pathway |
| Gender | Women 2x > men | No strong sex predilection |
| Age of onset | Typically after 4th decade | Earlier than AVNRT |
| Structural heart disease | Not correlated | Not typically correlated |
AVNRT - AV Nodal Reentrant Tachycardia
Mechanism
The reentrant circuit is entirely within or perinodal tissue of the AV node, which has two functionally distinct pathways:
- Slow pathway - slower conduction, shorter refractory period (posterior)
- Fast pathway - faster conduction, longer refractory period (anterior)
Types
Typical AVNRT ("slow-fast") - Most common
- Antegrade conduction: down the slow pathway
- Retrograde conduction: up the fast pathway
- Atrial and ventricular activation occur nearly simultaneously
- Result: Short RP tachycardia
ECG features:
- P wave buried in or at the terminal end of the QRS
- Pseudo-r' in V1 (most characteristic sign - ~45% of cases)
- Pseudo-S wave in inferior leads (II, III, aVF)
- RP interval < 70 ms (often < 1/2 of the RR interval)
- Rate: typically 150-250 bpm, regular
Atypical AVNRT ("fast-slow") - Less common
- Antegrade: down the fast pathway; Retrograde: up the slow pathway
- Long RP tachycardia
- Retrograde P wave inscribed well after the QRS in the second half of the RR interval
AVRT - AV Reentrant Tachycardia
Mechanism
A macro-reentrant circuit involving:
- The atrium
- The AV node and His-Purkinje system
- The ventricle
- An accessory pathway (AP) / bypass tract connecting atria to ventricles outside the AV node
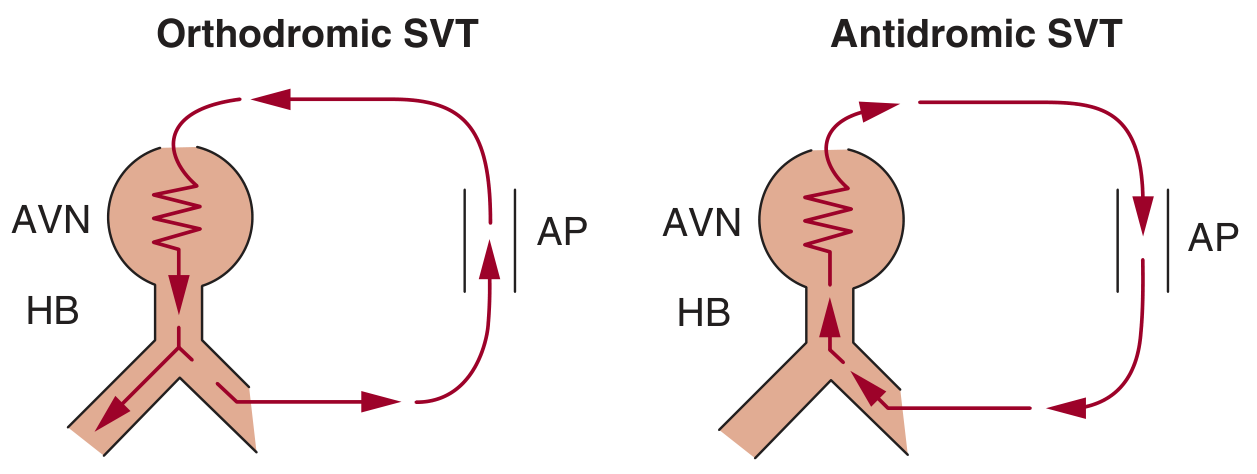
Orthodromic vs Antidromic AVRT circuit - Fuster and Hurst's The Heart, 15th Ed.
Types
Orthodromic AVRT (~95% of AVRT)
- Antegrade: down the AV node → narrow QRS
- Retrograde: up the accessory pathway
- Short RP tachycardia (RP > 70 ms, P visible after QRS, usually separated from it)
- Most common SVT in patients with WPW syndrome
- Can occur with a concealed AP (no preexcitation on resting ECG - retrograde conduction only)
Antidromic AVRT (<5% of AVRT)
- Antegrade: down the accessory pathway
- Retrograde: up the AV node (or second AP)
- Produces a wide, fully preexcited QRS - can mimic VT
- Seen only in patients with WPW syndrome (manifest AP)
Wolff-Parkinson-White Syndrome
- Defined by preexcitation + tachyarrhythmia
- Resting ECG: short PR interval + delta wave (slurred QRS upstroke)
- Risk: AF with rapid conduction through AP → ventricular fibrillation (if AP has short refractory period)
ECG Comparison: Key Differentiating Features
| ECG Feature | Typical AVNRT | Orthodromic AVRT |
|---|---|---|
| QRS | Narrow | Narrow (wide if BBB) |
| RP interval | Very short (<70 ms); P in/at tail of QRS | Short but longer (>70 ms); P after QRS |
| P wave location | Pseudo-r' in V1, pseudo-S in inferior leads | Retrograde P visible in ST segment |
| Preexcitation on SR ECG | Absent | Present in manifest AP (WPW); absent in concealed AP |
| BBB effect on rate | No change | Slows rate if BBB ipsilateral to AP (Coumel's sign) |
| R-P variability | Fixed (constant VA time) | Fixed (constant VA time) |
Key differentiator from AT: Both AVNRT and AVRT have a fixed, non-varying RP relationship. Variability in the RP interval points to AT instead.
Acute Management (both conditions)
- Vagal maneuvers (Valsalva, carotid sinus massage) - first-line
- IV Adenosine 6 mg rapid bolus (can repeat 12 mg x2) - terminates most cases by blocking AV node
- IV Beta-blockers or non-dihydropyridine CCBs (diltiazem, verapamil) - if adenosine fails
- Synchronized DC cardioversion - if hemodynamically unstable
Caution: Avoid AV nodal blockers (adenosine, verapamil, digoxin) in antidromic AVRT or AF with WPW - they can accelerate conduction through the AP and precipitate VF. Use procainamide or ibutilide instead.
Long-Term / Definitive Management
| AVNRT | AVRT | |
|---|---|---|
| Curative | RF catheter ablation of slow pathway (success >95%, AV block risk <1%) | RF catheter ablation of accessory pathway (success ~95%) |
| Medical suppression | Beta-blockers, verapamil, diltiazem, flecainide | Beta-blockers, flecainide, propafenone |
| Cryoablation | Used near His bundle to reduce AV block risk | Used for septal pathways |
Catheter ablation is preferred for symptomatic, recurrent, or medication-refractory cases in both conditions. Success rates exceed 95% with low complication rates.
Sources: Fuster and Hurst's The Heart, 15th Ed. | Braunwald's Heart Disease | The Washington Manual of Medical Therapeutics
Create an ECG interpretation guide comparing AVNRT vs AVRT
Asking for Preferences
Reading File
Finding Sources
Reading File
Reading File
Running Command
node /home/daytona/skills/shared/scripts/fetch_images.js \ "https://cdn.orris.…
Finding Sources
This is a shared conversation. Sign in to Orris to start your own chat.