Basis of babinski sign
Reading File
Finding Sources
Searching the Web
Babinski sign basis neurological mechanism corticospinal tract
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from the textbooks. Here is a full answer:
Basis of the Babinski Sign
What It Is
The Babinski sign (described by Joseph Babinski in 1896 and 1903) is the abnormal extensor plantar response: stroking the lateral sole of the foot from heel toward the toes produces dorsiflexion (extension/upgoing) of the great toe, often with fanning (abduction) of the other toes.
- The normal (negative) response in adults: the toes plantar flex (curl downward).
- A positive Babinski sign in any adult is always abnormal.
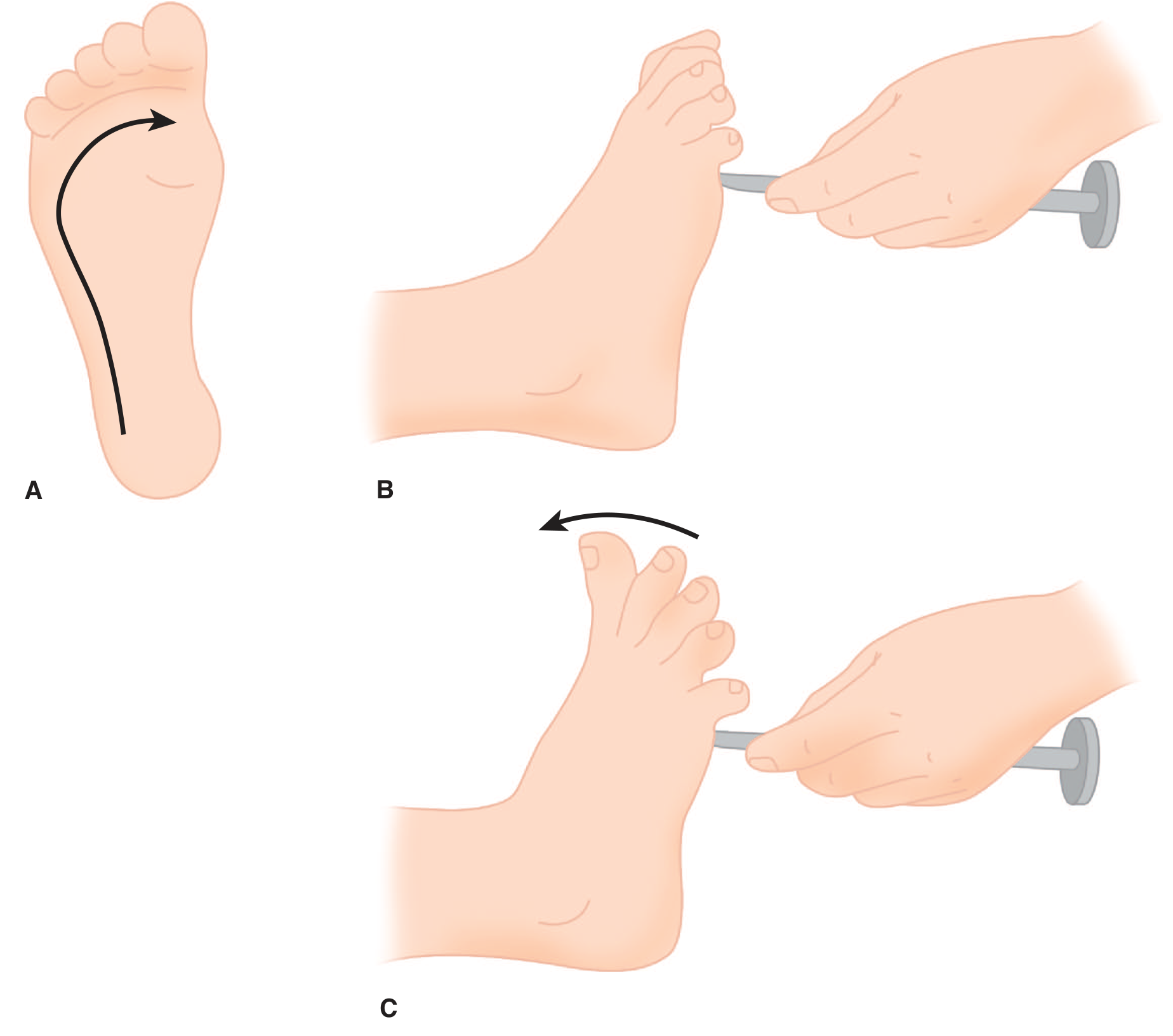
Figure: A - Stimulus path along lateral sole; B - Normal flexor plantar response; C - Extensor plantar response (Babinski sign). (Adams & Victor's Principles of Neurology)
The Neural Basis
1. Normal Plantar Reflex Circuit
In a healthy adult, stroking the sole activates cutaneous afferents (predominantly from the S1 dermatome) that synapse in the spinal cord. The response is plantar flexion of the toes, mediated through lower motor neurons. This normal flexor response is actively maintained by tonic descending corticospinal (pyramidal) tract inhibition on spinal cord interneurons.
2. Why It Becomes Extensor: Corticospinal Tract Damage
When the corticospinal (pyramidal) tract is damaged anywhere along its course - from the motor cortex, through the internal capsule, brainstem, or spinal cord - descending inhibitory control over spinal cord circuits is lost. The result is disinhibition (release) of a primitive spinal reflex program.
The key mechanism, as described in Adams & Victor's, is:
"The extension movement of the great toe is a component of a larger synergistic flexion or shortening reflex of the leg - toe extension when viewed from a physiologic perspective is a protective (nocifensive, or defensive) response... These spinal flexion reflexes are present because of disinhibition or release of motor programs of spinal origin."
So paradoxically, the upgoing toe is actually part of a spinal flexor withdrawal reflex - from the leg's perspective, dorsiflexion of the foot and extension of the great toe are components of limb withdrawal (hip flexion, knee flexion, ankle dorsiflexion - "triple flexion"). The normal corticospinal tract suppresses this primitive program; when it is lost, the reflex is released.
- Adams and Victor's Principles of Neurology, 12th Edition
3. Role of Reticulospinal Tracts
The corticospinal tract is not the only player. Two other descending systems contribute:
| Tract | Effect |
|---|---|
| Dorsal reticulospinal tract | Inhibits stretch reflexes - normally suppresses the extensor response |
| Medial reticulospinal + vestibulospinal | Facilitate extensor tone |
When the corticospinal tract is damaged but the dorsal reticulospinal tract is spared, only paresis and release of flexor reflexes (including the Babinski sign) occur - without spasticity. If both are damaged, full spasticity develops.
- Adams and Victor's Principles of Neurology, 12th Edition
Why It's Present in Infants (Up to ~12-18 months)
In infants, the corticospinal tract is not yet fully myelinated. Without effective descending corticospinal control, the primitive spinal flexor reflex is unmasked, producing a "physiologic" Babinski sign. As myelination completes over the first 1-2 years of life, the sign disappears and the normal adult flexor plantar response takes over.
"Its persistence or emergence in late infancy and childhood or later in life is an indicator of a lesion at some level of the corticospinal tract." - Adams & Victor's
Clinical Significance
| Finding | Implication |
|---|---|
| Positive in an adult | Upper motor neuron (UMN) lesion - corticospinal tract damage |
| Positive in infant <12-18 months | Normal (incomplete myelination) |
| Unilateral positive | Ipsilateral corticospinal tract lesion (above decussation = contralateral brain/brainstem; below decussation = ipsilateral spinal cord) |
| Bilateral positive | Bilateral corticospinal tract involvement |
The lesion can be anywhere along the corticospinal tract: cortex → internal capsule → cerebral peduncle → pons → medullary pyramid → lateral funiculus of spinal cord.
- Neuroanatomy through Clinical Cases, 3rd Edition
- Gray's Anatomy for Students
Equivalent Signs (Same Basis)
Several other maneuvers release the same spinal reflex program and produce the same upgoing toe:
- Chaddock sign - stroke lateral dorsum of foot
- Oppenheim sign - stroke tibia downward
- Gordon sign - squeeze calf muscles
- Bing sign - pinprick to dorsum of foot
All have the same pathological basis: corticospinal tract disruption releasing the spinal nocifensive flexor reflex.
Summary in one sentence: The Babinski sign is a release phenomenon - damage to the corticospinal tract removes descending inhibition, unmasking a primitive spinal cord flexor (nocifensive) reflex in which the great toe extends as part of the limb withdrawal synergy, a response normally present in unmyelinated infant nervous systems and suppressed in healthy adults.
This is a shared conversation. Sign in to Orris to start your own chat.