What causes the formation of concentration of urine explain the physiology of ccm in very easy word
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I have more than enough information to give a thorough, easy-to-understand answer. Let me now write it up.
Concentration of Urine: Physiology of the Countercurrent Mechanism (CCM)
The Big Picture (Why Does Urine Get Concentrated?)
Your kidney's job is to clean your blood AND control how much water leaves your body. When you're dehydrated, the kidney makes small amounts of very concentrated urine to save water. When you drink too much, it makes large amounts of dilute urine to get rid of the excess.
The process that allows concentration of urine depends on two things working together:
- A special region in the kidney (the renal medulla) that is kept extremely salty/concentrated - up to 1200-1400 mOsm/L (compared to normal blood at 300 mOsm/L)
- A hormone called ADH (antidiuretic hormone) that opens water channels in the collecting duct
The mechanism that builds and maintains this salty medulla is called the Countercurrent Multiplier Mechanism (CCM).
What Does "Countercurrent" Mean?
"Counter" = opposite. "Current" = flow.
Imagine two lanes of traffic next to each other, going in opposite directions. In the kidney, fluid flows down one tube and comes back up the adjacent tube - this is the Loop of Henle, and because fluid flows in opposite directions in the two limbs, it is called "countercurrent."
The Three Players in CCM
1. The Loop of Henle (the Multiplier)
This is the U-shaped part of the nephron that dips deep into the medulla. It has two limbs:
| Part | Water Permeable? | Active Pumping? |
|---|---|---|
| Descending limb | YES - water flows out freely | No |
| Ascending limb (thick) | NO - water cannot escape | YES - pumps Na+, K+, Cl- out |
This asymmetry is the key trick. The thick ascending limb pumps salt OUT into the interstitium but water cannot follow. So the interstitium becomes salty/concentrated.
2. The Vasa Recta (the Exchanger)
These are special hairpin-shaped capillaries that run alongside the Loop of Henle in opposite directions. Their job is to carry away the reabsorbed water without washing away the salt concentration gradient. They act as a countercurrent exchanger - solutes they pick up going down, they deposit going up, preserving the medullary gradient.
3. The Collecting Duct (the Final Concentrator)
The collecting duct runs through the hypertonic medulla. When ADH is present, it opens aquaporin-2 (AQP-2) water channels, allowing water to be sucked out of the urine by the salty medulla. This is the step where urine actually gets concentrated.
How CCM Works Step-by-Step (Very Simple)
Think of it like building a salt mountain layer by layer:
Step 1 - Starting point: Fluid enters the Loop of Henle from the proximal tubule at about 300 mOsm/L (same as blood).
Step 2 - Thick ascending limb pumps salt out: The pump in the thick ascending limb removes Na+, K+, and Cl- from the tubular fluid and dumps them into the medullary interstitium. This creates a concentration difference of about 200 mOsm/L between the tubule and the interstitium.
Step 3 - Descending limb loses water: Because the interstitium is now saltier, water is drawn OUT of the descending limb by osmosis. The fluid going DOWN the loop becomes more and more concentrated as it moves toward the tip.
Step 4 - The multiplying effect: As this more concentrated fluid rounds the bend and comes back UP the ascending limb, the pump again pushes salt out - but now it's starting from a higher concentration. This "multiplies" the effect - each cycle adds to the gradient.
Step 5 - Urea adds to the effect: The inner medullary collecting duct is also permeable to urea (when ADH is present). Urea diffuses out and contributes to the interstitial osmolarity, adding to the concentration gradient.
End result: A progressive osmotic gradient builds from the cortex (~300 mOsm/L) to the deepest part of the medulla (~1200-1400 mOsm/L). Like layers of a pyramid, each deeper layer is saltier.
The Final Step - ADH and Collecting Duct
Once the salty medulla is built, urine concentration actually happens in the collecting duct:
- No ADH present → water channels (AQP-2) stay closed → water cannot leave → dilute urine is produced (like when you drink lots of water)
- ADH present (e.g., dehydration) → AQP-2 channels open → water rushes out of the collecting duct into the salty medulla → small volume of concentrated urine is produced
ADH is released from the posterior pituitary when blood osmolarity rises or blood volume falls.
Summary Table
| Structure | Role in CCM |
|---|---|
| Thick ascending limb | Pumps NaCl out, impermeable to water → builds medullary gradient |
| Thin descending limb | Freely permeable to water → fluid concentrates as it descends |
| Vasa recta | Hairpin capillaries that preserve the gradient while removing reabsorbed water |
| Collecting duct | Final site of water reabsorption (only when ADH opens AQP-2 channels) |
| Urea recycling | Contributes ~40-50% of inner medullary osmolarity |
Simple Analogy
Imagine a salt factory on a hill:
- Workers (the ascending limb) keep throwing salt DOWN the hill into the surrounding ground
- Rain water (descending limb fluid) soaks up the salt as it flows down
- The deeper you go, the saltier the ground
- A final tap (collecting duct) opens when the boss (ADH) gives the order, letting water seep into the salty ground and concentrating the remaining urine
Sources:
- Guyton and Hall Textbook of Medical Physiology, pp. 373-376 (Chapter 29 - Countercurrent Multiplier Mechanism)
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology, p. 1915 (Histophysiology of the Kidney)
H and hv3 ion handling by renal tubules easy words
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Explain the role of the kidney in maintaining acid base balance and explain the mechanism of acidification of urine 5 marks invery easy words
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I have all the content needed. Here is the complete, easy-language answer:
Kidney's Role in Acid-Base Balance + Mechanism of Urine Acidification
First - Why Does the Kidney Need to Do This?
Your body constantly produces acids during normal metabolism (digestion, exercise, breathing). Blood pH must stay very narrow - between 7.35 and 7.45. If it falls below 7.35, you have acidosis. Above 7.45 = alkalosis. Both are dangerous.
- Lungs handle CO₂ (carbonic acid) - fast response (seconds to minutes)
- Kidneys handle the rest - slow but powerful (hours to days), and they are the final defence
Normal blood pH = 7.4, but urine pH can range from 4.5 to 8.0 - meaning the kidney can dump a lot of acid into urine when needed.
The 3 Main Ways the Kidney Controls Acid-Base
1. 🔁 Reclaiming Bicarbonate (HCO₃⁻) - "Save the Base"
HCO₃⁻ is the body's most important buffer (base). The kidney must not let it spill into urine.
How it works (Proximal tubule - 90% happens here):
Step 1: Tubular cell secretes H⁺ into the tubule lumen via the Na⁺/H⁺ exchanger (NHE3) Step 2: This H⁺ meets the filtered HCO₃⁻ in the lumen Step 3: They combine → H₂CO₃ → then carbonic anhydrase breaks it down into CO₂ + H₂O Step 4: CO₂ drifts back INTO the tubular cell Step 5: Inside the cell, carbonic anhydrase converts CO₂ + H₂O → H₂CO₃ → H⁺ + HCO₃⁻ Step 6: HCO₃⁻ goes back into the blood ✅, H⁺ is secreted again ✅
Simple summary: H⁺ is used as a "ferry" to carry bicarbonate back from the urine into the blood. Roughly 4500 mmol/day of bicarbonate is reclaimed this way.
2. 🧪 Ammonia (NH₃) Production - "Make New Bicarbonate"
This is how the kidney actually gets rid of excess acid and makes new HCO₃⁻ to replace what was used up buffering acids.
How it works:
Step 1: Tubular cells break down the amino acid glutamine (from muscles/liver) Step 2: This produces NH₃ (ammonia) + α-ketoglutarate Step 3: NH₃ is a gas - it diffuses into the tubule lumen Step 4: In the acidic urine, NH₃ + H⁺ → NH₄⁺ (ammonium) - which is TRAPPED and excreted Step 5: α-ketoglutarate is converted to new HCO₃⁻ which goes back into blood
This accounts for ~60% of daily H⁺ excretion (~30-60 mmol/day). In acidosis, the kidney ramps up glutamine breakdown dramatically to excrete more H⁺.
3. 🧱 Phosphate Buffer - "Titratable Acid"
Some of the secreted H⁺ reacts with the phosphate in the filtrate:
HPO₄²⁻ + H⁺ → H₂PO₄⁻ (excreted in urine)
This accounts for about 30 mmol of H⁺/day. This is called titratable acidity - it directly lowers urine pH.
Mechanism of Acidification of Urine - Step by Step
Here is the textbook diagram showing all three processes together:
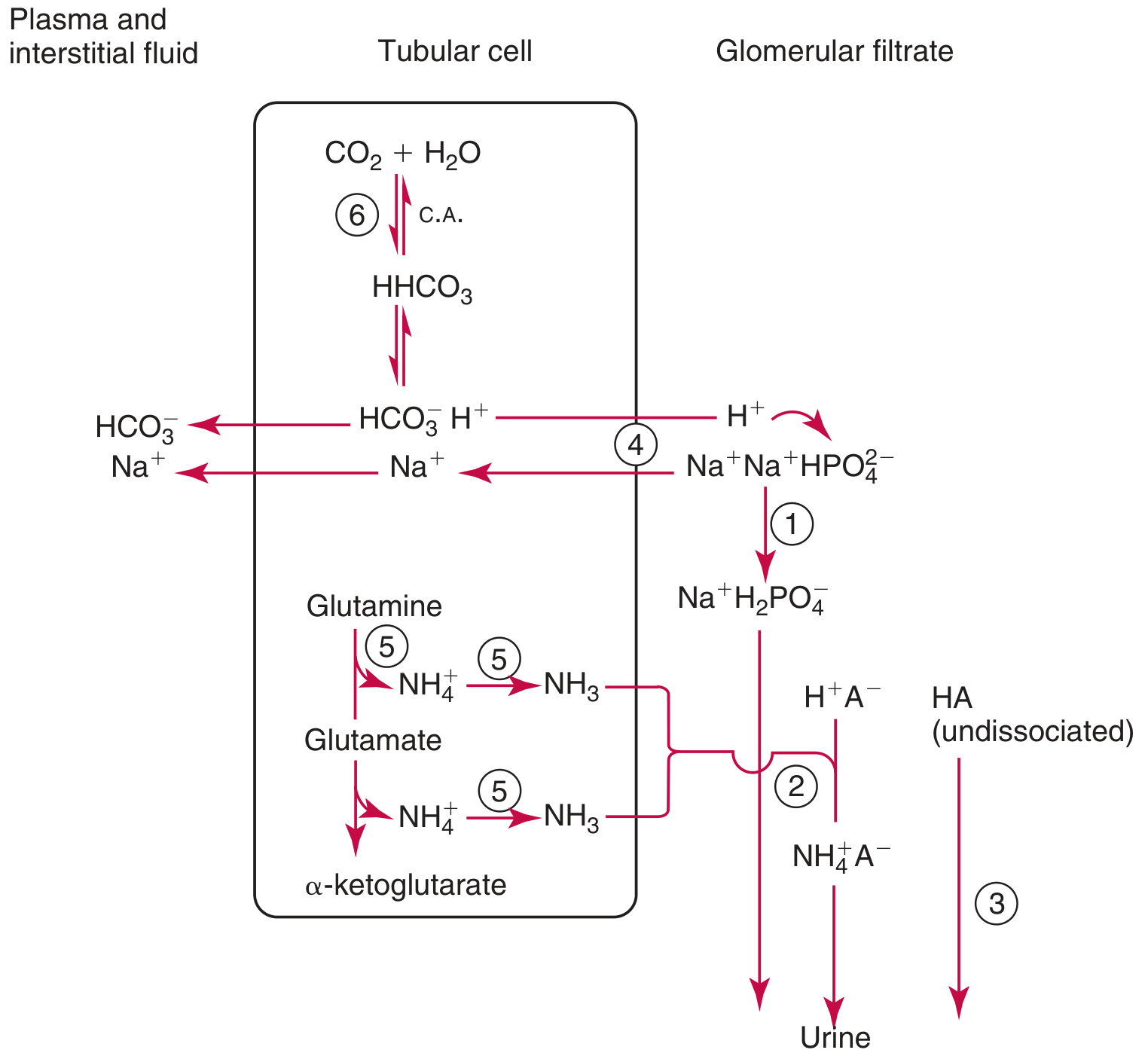
The key steps are:
| Step | What Happens | Where |
|---|---|---|
| 1 | Tubular cells make CO₂ + H₂O → H₂CO₃ → H⁺ + HCO₃⁻ (via carbonic anhydrase) | All tubular cells |
| 2 | H⁺ is pumped OUT into the lumen via NHE3 (Na⁺/H⁺ exchanger) or H⁺-ATPase | Proximal + collecting duct |
| 3 | Luminal H⁺ reacts with HCO₃⁻ → CO₂ (reclaimed) OR with NH₃ → NH₄⁺ (excreted) OR with HPO₄²⁻ → H₂PO₄⁻ (excreted) | Lumen |
| 4 | HCO₃⁻ generated inside cell returns to blood via NBC transporter | Basolateral side |
| 5 | Net result: Urine becomes acidic, blood becomes more alkaline | Final urine pH as low as 4.4 |
Maximum urine pH that can be achieved:
- Proximal tubule: can maintain up to 1 pH unit gradient
- Distal tubule/collecting duct: can maintain up to 3 pH units gradient
- Minimum urine pH ≈ 4.4
Role Segment by Segment
| Tubule Segment | Job |
|---|---|
| Proximal tubule | Reabsorbs 90% of filtered HCO₃⁻, secretes large amounts of H⁺ via NHE3 |
| Thick ascending limb | Reabsorbs some HCO₃⁻ |
| Distal tubule | Secretes H⁺ via H⁺-ATPase, fine-tunes acid secretion |
| Collecting duct (α-intercalated cells) | Major site of final acidification - secretes H⁺ by H⁺-ATPase pump, generates new HCO₃⁻ |
Summary - "What the Kidney Does in Acidosis vs Alkalosis"
| Body State | Kidney Response |
|---|---|
| Acidosis (blood too acidic) | Secretes more H⁺, produces more NH₃, reclaims all HCO₃⁻ → urine becomes very acidic (pH ~4.5) |
| Alkalosis (blood too basic) | Stops secreting H⁺, lets HCO₃⁻ spill into urine → urine becomes alkaline (pH ~8.0) |
One-Line Memory Aid
"The kidney saves base (HCO₃⁻), dumps acid (H⁺ via phosphate and ammonia), and is the LAST and most powerful controller of blood pH."
Sources:
- Tietz Textbook of Laboratory Medicine, 7th Edition, pp. 1950-1951 (Renal Mechanisms in Acid-Base Balance)
- Brenner and Rector's The Kidney, p. 365 (Bicarbonate Reabsorption and H⁺ Secretion)
Describe the physiological of micturtion also mention the significance of cytometrogram easyyyy word
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I have everything needed. Here is the complete, easy-word answer:
Physiology of Micturition + Significance of Cystometrogram
What is Micturition?
Micturition = urination = passing urine. It is the process by which urine stored in the bladder is expelled out of the body. It is NOT just a simple squeeze - it involves a beautifully coordinated reflex involving the nervous system, bladder muscles, and two sphincters.
Parts of the Bladder You Need to Know
| Structure | Job |
|---|---|
| Detrusor muscle | Smooth muscle of the bladder wall - contracts to push urine out |
| Internal urethral sphincter | Smooth muscle, involuntary - normally CLOSED |
| External urethral sphincter | Skeletal muscle, voluntary - you control this one |
| Stretch receptors | Sensors in the bladder wall that feel how full it is |
Phase 1: FILLING (Storage Phase)
Think of this as "filling a water balloon quietly".
- Urine drips into the bladder from the ureters continuously
- The bladder wall is elastic - it stretches and relaxes to accommodate more urine without much rise in pressure (this is called "compliance")
- Up to about 150 mL - you feel a slight urge
- At 300-400 mL - you feel a definite urge
- At >400 mL - pressure rises sharply and the urge becomes urgent
During this entire filling phase:
- Sympathetic nervous system keeps the detrusor relaxed and internal sphincter CLOSED
- Voluntary control keeps the external sphincter CLOSED
- The brain says "not yet!" - it actively inhibits the micturition reflex
Phase 2: THE MICTURITION REFLEX (The Trigger)
When the bladder fills enough, stretch receptors in the bladder wall fire off signals. Here is the reflex arc:
Bladder stretch receptors
↓ (pelvic nerves - afferent signals)
Sacral spinal cord (S2, S3, S4) ← THE MICTURITION CENTER
↓ (pelvic nerves - efferent signals)
Parasympathetic activation
↓
Detrusor muscle CONTRACTS
↓
Pressure rises → more stretch → more stretch receptor firing
↓ (self-regenerative cycle)
Strong sustained contraction
This is a spinal reflex - it can happen even without the brain (as in spinal cord injury patients).
Phase 3: VOIDING (Emptying Phase)
"The green light is given" - when socially appropriate:
Step 1: Cerebral cortex stops inhibiting the sacral micturition center Step 2: Person voluntarily relaxes the external sphincter (you control this) Step 3: Pontine Micturition Center (PMC) in brainstem coordinates everything Step 4: Internal sphincter also relaxes Step 5: A small bit of urine enters the posterior urethra → triggers MORE stretch receptors → makes the detrusor contraction even stronger Step 6: Detrusor contracts powerfully → urine is expelled Step 7: Abdominal muscles may also contract voluntarily to help
After complete emptying, the reflex fatigues, detrusor relaxes, and both sphincters close again.
Neural Control Summary - "Who Controls What"
| Brain Center | Role |
|---|---|
| Cerebral cortex | Voluntary control - can STOP or START urination |
| Pontine Micturition Center (PMC) | Coordinates detrusor contraction + sphincter relaxation simultaneously |
| Sacral cord (S2-S4) | The actual reflex center - parasympathetic outflow |
| Sympathetic (T10-L2) | Storage phase - relaxes detrusor, closes internal sphincter |
| Pudendal nerve | Controls external sphincter (voluntary) |
Key rule: The detrusor contracts at the SAME TIME the sphincters relax - these must be perfectly coordinated. If they don't coordinate (called "detrusor-sphincter dyssynergia"), urination fails.
What is a Cystometrogram (CMG)?
A cystometrogram is a graph that shows the relationship between bladder volume (x-axis) and intravesical pressure (y-axis) as the bladder is slowly filled.
How it is done: A catheter is inserted into the bladder, it is emptied, then saline is slowly dripped in while pressure is continuously recorded.
The Normal Cystometrogram:
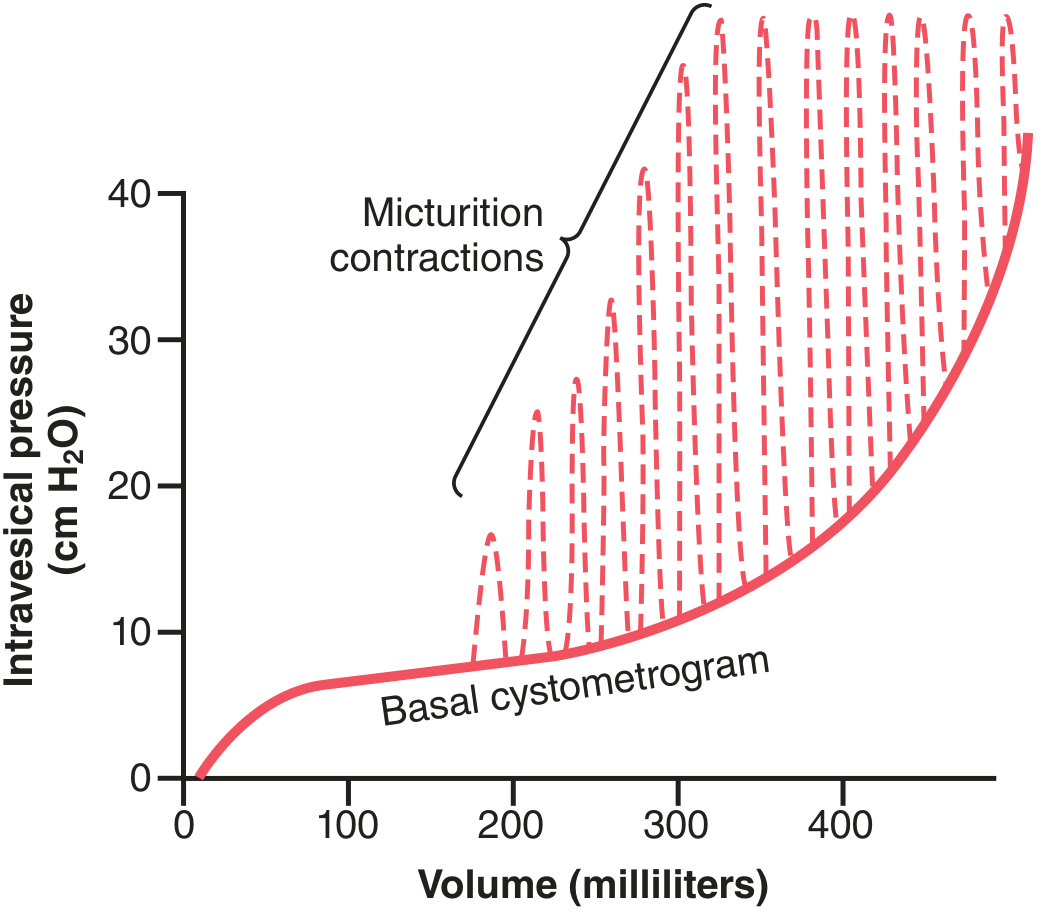
Reading the graph (in easy words):
| Volume | What the Graph Shows | What it Means |
|---|---|---|
| 0 - 50 mL | Slight initial pressure rise | Bladder wall is slightly tense at first |
| 50 - 300 mL | Flat/very slowly rising line | Detrusor relaxes, bladder is very compliant - this is the TONIC segment |
| 300 - 400 mL | Pressure starts rising | Bladder is getting full, compliance decreasing |
| >400 mL | Sharp rise in pressure | Bladder is overfull and struggling |
| Dashed spikes | Sudden sharp pressure peaks (micturition waves) | These are the micturition reflex contractions - each spike = one attempted voiding reflex |
The spikes (micturition contractions) appear first around 200 mL, then become bigger and more frequent as the bladder fills more.
Significance of the Cystometrogram
The CMG is used clinically to diagnose bladder problems. Here is what different abnormal patterns mean:
| CMG Finding | What it Means | Clinical Condition |
|---|---|---|
| High pressure at low volumes (steep curve) | Bladder is stiff/non-compliant | Fibrotic bladder, neurogenic bladder |
| Absent micturition spikes | Detrusor cannot contract | Atonic/flaccid bladder (e.g., lower motor neuron lesion, tabes dorsalis) |
| Early and large micturition spikes at low volumes | Detrusor is overactive/irritable | Overactive bladder, upper motor neuron lesion |
| Normal curve but no voiding | Sphincter not relaxing | Detrusor-sphincter dyssynergia |
| Normal CMG | Bladder function intact | Rules out neurogenic bladder |
In one line:
The cystometrogram is the "ECG of the bladder" - it tells us whether the bladder fills normally, feels sensation at the right volume, and contracts at the right time.
One-Line Summary of Micturition
Bladder fills → stretch receptors fire → sacral cord reflex → detrusor contracts + sphincters relax (coordinated by pons) → urine expelled → all under voluntary cortical control.
Sources:
- Guyton and Hall Textbook of Medical Physiology, pp. 332-334 (Micturition Reflex & Cystometrogram)
- Medical Physiology (Boron & Boulpaep), p. 737 (Cystometrogram & Micturition Reflex Control)
Late distal tubules and collecting tubules contain two types of intercalated cells
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
All diagrams and content retrieved. Here is the full easy-word explanation:
Two Types of Intercalated Cells in Late Distal Tubule and Collecting Duct
First - What Are Intercalated Cells?
The late distal tubule and cortical collecting tubule are lined by two main cell types:
| Cell Type | Main Job |
|---|---|
| Principal cells | Reabsorb Na⁺ and water, secrete K⁺ (aldosterone-controlled) |
| Intercalated cells | Handle H⁺ and HCO₃⁻ - the acid-base specialists |
Here is what these cells look like in the tubule cross-section:
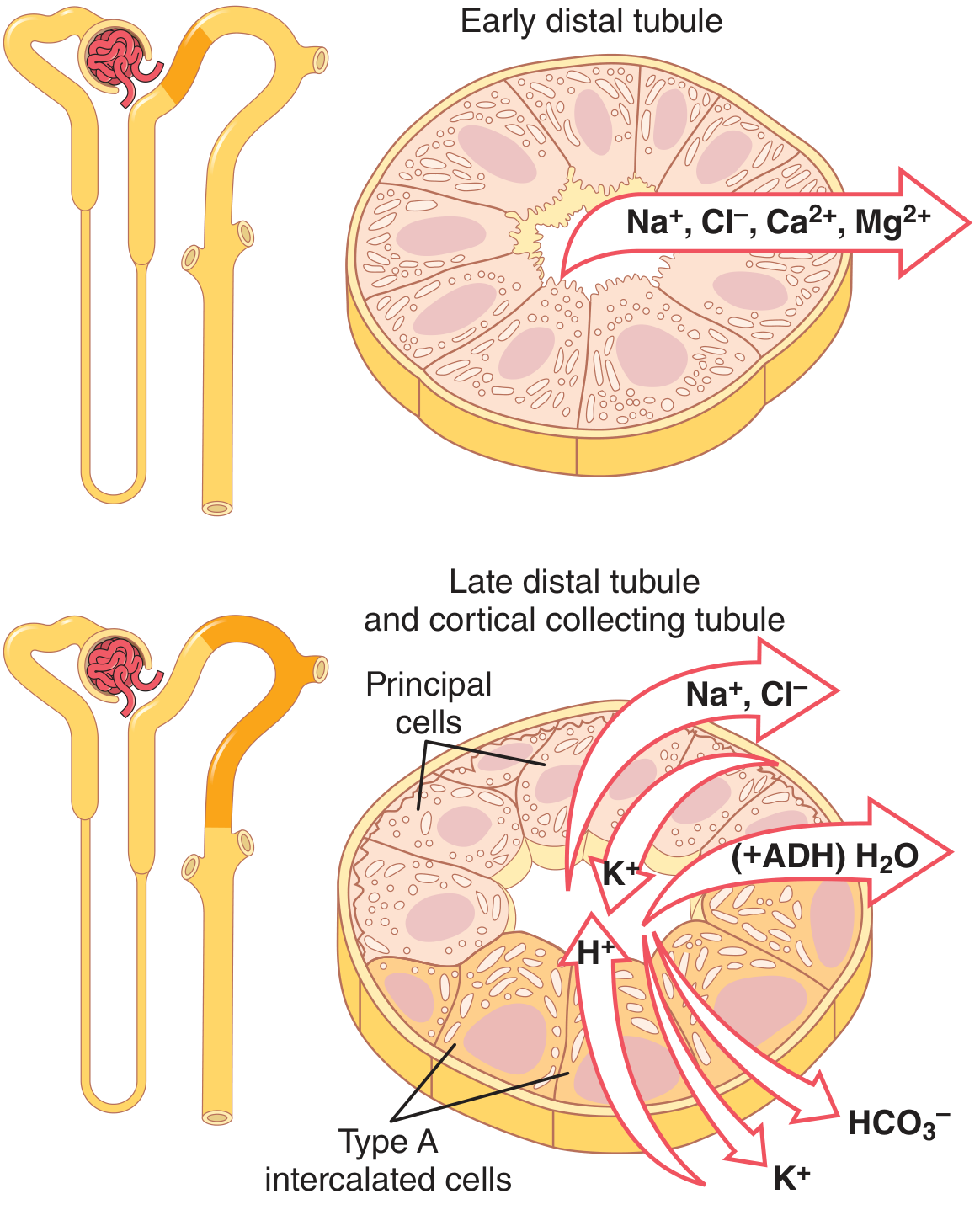
The intercalated cells come in two subtypes - Type A and Type B - and they do exactly OPPOSITE things. Think of them as "Team Acid" and "Team Alkali."
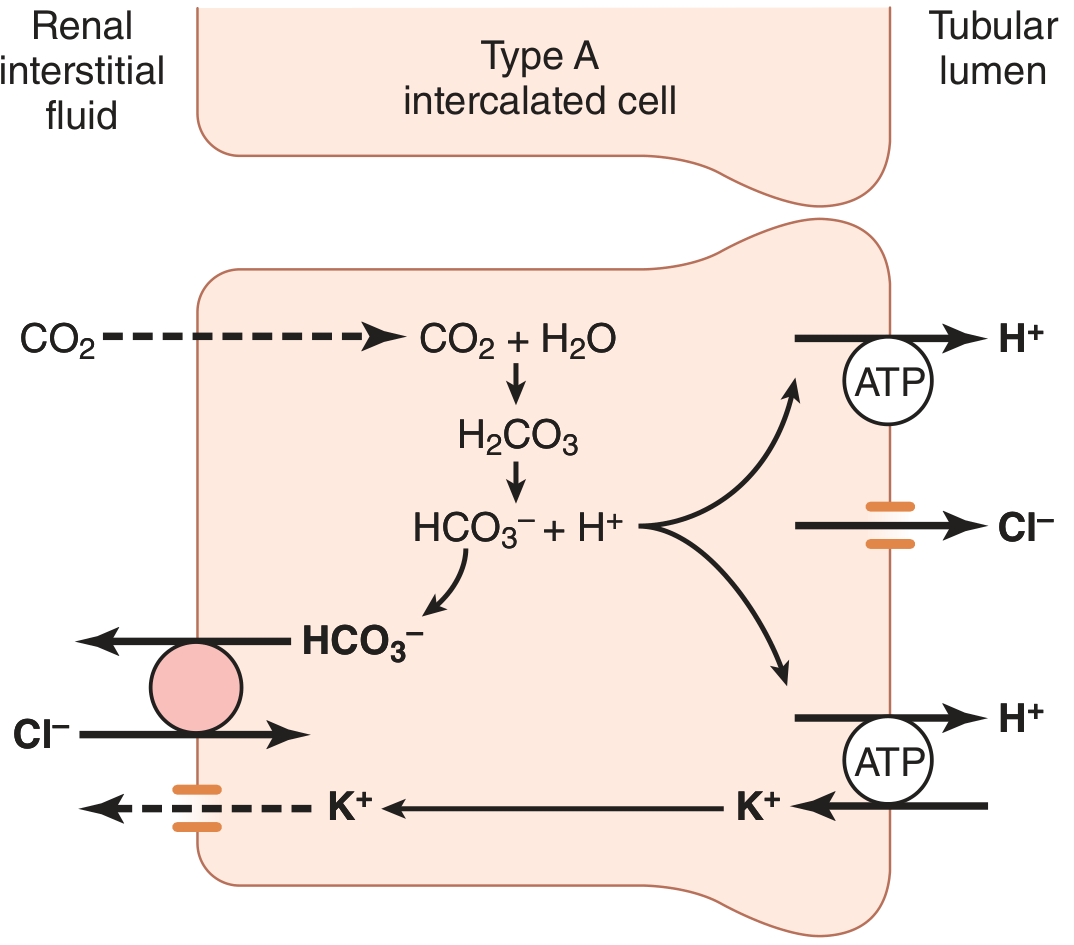
TYPE A Intercalated Cell - "The Acid Secretor"
Active when: Body is too ACIDIC (acidosis)
What it does:
- Secretes H⁺ (acid) INTO the tubular lumen → excreted in urine
- Reabsorbs HCO₃⁻ (base) back into the blood
- Reabsorbs K⁺ from the lumen
How it works (step by step):
Step 1: CO₂ enters the cell from blood Step 2: Inside cell: CO₂ + H₂O → H₂CO₃ (via carbonic anhydrase) → H⁺ + HCO₃⁻ Step 3: H⁺ is pumped OUT into the tubular lumen by two pumps on the APICAL (luminal) side:
- H⁺-ATPase (proton pump) - most important
- H⁺-K⁺-ATPase (exchanges H⁺ out for K⁺ in) Step 4: HCO₃⁻ exits on the BASOLATERAL side (blood side) via a Cl⁻/HCO₃⁻ exchanger → goes back to blood ✅
The Key Pumps: ON THE APICAL (LUMEN) SIDE
Memory trick for Type A: A = Acid out → H⁺ pumped into LUMEN. "A for Acid secretor, Apical ATPase."
Special feature of Type A:
- Can create a H⁺ concentration gradient of up to 1000:1 between cell and lumen
- This is MUCH more powerful than the proximal tubule (which can only do 4-10:1)
- This allows final maximum acidification of urine (pH as low as 4.4)
TYPE B Intercalated Cell - "The Bicarbonate Secretor"
Active when: Body is too ALKALINE (alkalosis)
What it does - EXACTLY OPPOSITE of Type A:
- Secretes HCO₃⁻ (base) INTO the tubular lumen → excreted in urine
- Reabsorbs H⁺ back into the blood
- Secretes K⁺ into the lumen
How it works (step by step):
Step 1: CO₂ enters the cell → same reaction → H⁺ + HCO₃⁻ formed inside Step 2: H⁺-ATPase is on the BASOLATERAL side now (opposite to Type A!) → pumps H⁺ INTO the blood Step 3: HCO₃⁻ is secreted into the LUMEN via a special transporter called PENDRIN (Cl⁻/HCO₃⁻ exchanger on apical membrane) Step 4: Pendrin brings Cl⁻ in and pushes HCO₃⁻ out into the tubule → excreted in alkaline urine ✅
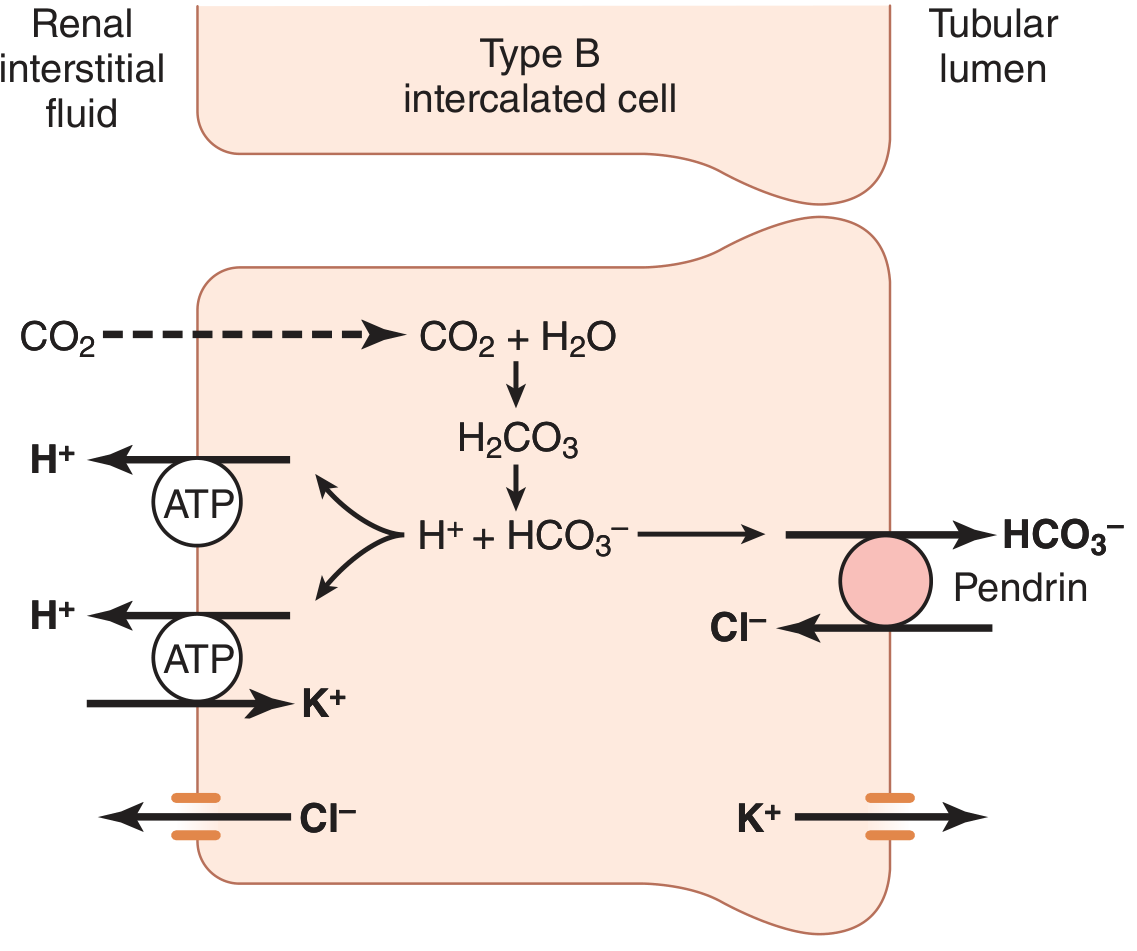
Memory trick for Type B: B = Base (HCO₃⁻) secreted into lumen. B for Bicarbonate secretor, Basolateral ATPase.
Side-by-Side Comparison Table
| Feature | Type A Intercalated Cell | Type B Intercalated Cell |
|---|---|---|
| Active in | Acidosis | Alkalosis |
| H⁺-ATPase location | APICAL (lumen side) | BASOLATERAL (blood side) |
| Cl⁻/HCO₃⁻ exchanger | Basolateral (anion exchanger 1) | Apical (PENDRIN) |
| H⁺ movement | Secreted INTO lumen | Reabsorbed into blood |
| HCO₃⁻ movement | Reabsorbed into blood | Secreted INTO lumen |
| K⁺ movement | Reabsorbed from lumen | Secreted into lumen |
| Net effect on urine | Urine becomes MORE ACIDIC | Urine becomes MORE ALKALINE |
| Net effect on blood | Blood pH rises (corrects acidosis) | Blood pH falls (corrects alkalosis) |
| Numbers (CCD) | ~60% of intercalated cells | ~40% of intercalated cells |
How the Body Adjusts the Numbers
The kidney is smart - it can actually change the proportion of Type A vs Type B cells depending on the body's needs:
- In chronic acidosis → more Type A cells are made → more H⁺ secretion
- In chronic alkalosis → more Type B cells are made → more HCO₃⁻ secretion
This is a long-term adaptive mechanism.
Clinical Relevance
| Disease | Problem |
|---|---|
| Distal RTA (Type 1) | Type A cells CANNOT secrete H⁺ properly → urine can't be acidified below pH 5.5, blood becomes acidic |
| Metabolic alkalosis | Type B cells activated → secrete excess HCO₃⁻ in urine to correct it |
Super Simple Summary
Type A = "Acid out, Base in" → fights ACIDOSIS (H⁺ ATPase on apical/lumen side)Type B = "Base out, Acid in" → fights ALKALOSIS (Pendrin on apical/lumen side, H⁺ ATPase on basolateral/blood side)Both cells generate H⁺ and HCO₃⁻ inside using carbonic anhydrase - they just send them in opposite directions!
Sources:
- Guyton and Hall Textbook of Medical Physiology, pp. 357-358 (Late Distal Tubules and Collecting Tubules - Figure 28.13)
- Brenner and Rector's The Kidney, pp. 109-110 (Cortical Collecting Duct - Intercalated Cell Subtypes)
Easyyy word
Here is the same topic explained in the simplest possible words - like explaining to a friend! 😊
Two Types of Intercalated Cells - Super Easy Version
The Big Idea First
Your blood pH must stay around 7.4 - not too acidic, not too alkaline.
The intercalated cells in the late distal tubule and collecting duct are the kidney's pH police. They sense when the blood is too acidic or too alkaline and FIX it.
There are two cops - Type A and Type B - and they do opposite jobs.
Think of It Like a Water Pump with Two Modes
Imagine a reversible pump in a cell:
- In Mode A → pump pushes ACID out into urine
- In Mode B → pump pushes BASE out into urine
🔴 TYPE A Cell - "The Acid Dumper"
When does it turn ON?
When your blood is too ACIDIC (like after eating lots of protein, exercise, diarrhea)
What does it do?
It throws H⁺ (acid) out into the urine It pulls HCO₃⁻ (base) back into the blood
How? (Very simple version)
Inside the cell:
CO₂ + H₂O → H⁺ + HCO₃⁻
↓ ↓
PUMPED OUT Goes to BLOOD
into URINE (saves it)
(via H⁺-ATPase
on LUMEN side)
Result: Urine becomes acidic. Blood becomes less acidic. ✅
One Line Memory:
"A = Acid out through the Apical (lumen) side"
🔵 TYPE B Cell - "The Base Dumper"
When does it turn ON?
When your blood is too ALKALINE (like after vomiting a lot, too much antacids)
What does it do?
It throws HCO₃⁻ (base) out into the urine It pulls H⁺ (acid) back into the blood
How? (Very simple version)
Inside the cell:
CO₂ + H₂O → H⁺ + HCO₃⁻
↓ ↓
Goes to BLOOD PUMPED OUT
(saves it) into URINE
(via PENDRIN
on LUMEN side)
Result: Urine becomes alkaline. Blood becomes less alkaline. ✅
One Line Memory:
"B = Base (HCO₃⁻) out through the lumen via Pendrin"
The Trick to Remember - They Are Mirror Images!
| Type A | Type B | |
|---|---|---|
| Blood too...? | Acidic | Alkaline |
| Dumps into urine | H⁺ (acid) | HCO₃⁻ (base) |
| Saves for blood | HCO₃⁻ (base) | H⁺ (acid) |
| Pump location | Lumen side (apical) | Blood side (basolateral) |
| Special transporter | Cl⁻/HCO₃⁻ exchanger (basolateral) | Pendrin (lumen side) |
The Simplest Analogy Ever 🎯
Imagine two dustbins (trash cans) next to a road:
- Type A bin collects and throws away acid trash (H⁺) into the urine road
- Type B bin collects and throws away base trash (HCO₃⁻) into the urine road
The body chooses which bin is open depending on what trash has built up in the blood!
Both Cells Use the SAME Machine Inside
Both Type A and Type B cells use carbonic anhydrase to make H⁺ and HCO₃⁻ inside the cell from CO₂ and water. The ONLY difference is:
Which direction they push things - it's the same factory, different exit doors!
Disease Connection (Bonus - Easy!)
- Type A cell broken? → Can't throw away acid → Blood stays acidic → Distal Renal Tubular Acidosis (Type 1 RTA)
- Too much alkalosis? → Type B cells increase in number → dump more base → fixes it
3-Word Summary
| Type A | Type B |
|---|---|
| "Acid → Urine" | "Base → Urine" |
Source: Guyton and Hall Textbook of Medical Physiology, pp. 357-358
In summary
Summary: Two Types of Intercalated Cells
The One Table You Need
| Type A | Type B | |
|---|---|---|
| Activated by | Acidosis (blood too acidic) | Alkalosis (blood too alkaline) |
| Secretes into urine | H⁺ (acid) | HCO₃⁻ (base) |
| Returns to blood | HCO₃⁻ (base) | H⁺ (acid) |
| H⁺-ATPase pump sits on | Apical (lumen) side | Basolateral (blood) side |
| Special transporter | Cl⁻/HCO₃⁻ exchanger (basolateral) | Pendrin (apical/lumen) |
| Net effect on urine | Acidic urine | Alkaline urine |
| Net effect on blood | Corrects acidosis | Corrects alkalosis |
One Line Each
🔴 Type A = Blood too acidic → dumps H⁺ into urine, saves HCO₃⁻ for blood. Pump on lumen side.
🔵 Type B = Blood too alkaline → dumps HCO₃⁻ into urine via Pendrin, saves H⁺ for blood. Pump on blood side.
The Golden Memory Trick
| A | Acid out, Apical pump |
| B | Base out, Basolateral pump, Pendrin |
Both cells use carbonic anhydrase inside to make H⁺ and HCO₃⁻ from CO₂ - they just send them in OPPOSITE directions.
Renal hypertension easyyy worddd
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Got everything needed. Here is the full easy-word explanation:
Renal Hypertension - Super Easy Words
What Is It?
Renal hypertension = High blood pressure CAUSED by the kidney.
Normal blood pressure = 120/80 mmHg. When the kidney senses it is NOT getting enough blood, it panics and releases chemicals that raise blood pressure throughout the whole body.
Simple idea: "Kidney feels low pressure → Kidney calls for help → Blood pressure goes UP everywhere"
Why Does the Kidney Cause High BP?
The kidney has a built-in alarm system called the Renin-Angiotensin-Aldosterone System (RAAS).
Think of it like this:
Kidney = a security guard for blood pressure When blood flow to the kidney drops, the guard shouts: "Emergency! Send more blood pressure!"
The Step-by-Step Mechanism (RAAS Explained Simply)
Kidney gets LESS blood flow
↓
Kidney releases RENIN (a chemical alarm)
↓
Renin converts Angiotensinogen → Angiotensin I (in blood)
↓
ACE (in lungs) converts Angiotensin I → Angiotensin II
↓
Angiotensin II does TWO things:
1. SQUEEZES blood vessels → BP rises immediately (within minutes)
2. Tells adrenal gland to release ALDOSTERONE
↓
Aldosterone tells kidneys to HOLD ON to Na+ and water
↓
More water in blood = More blood volume = BP rises more (over days)
Result: Sustained HIGH blood pressure
The Famous Goldblatt Experiment - Easy Version
Harry Goldblatt in the 1930s proved that kidney causes hypertension by doing a simple experiment:
He placed a clamp on the renal artery of a dog → Less blood reached the kidney → The dog developed HIGH blood pressure!
Here is what happened over time:
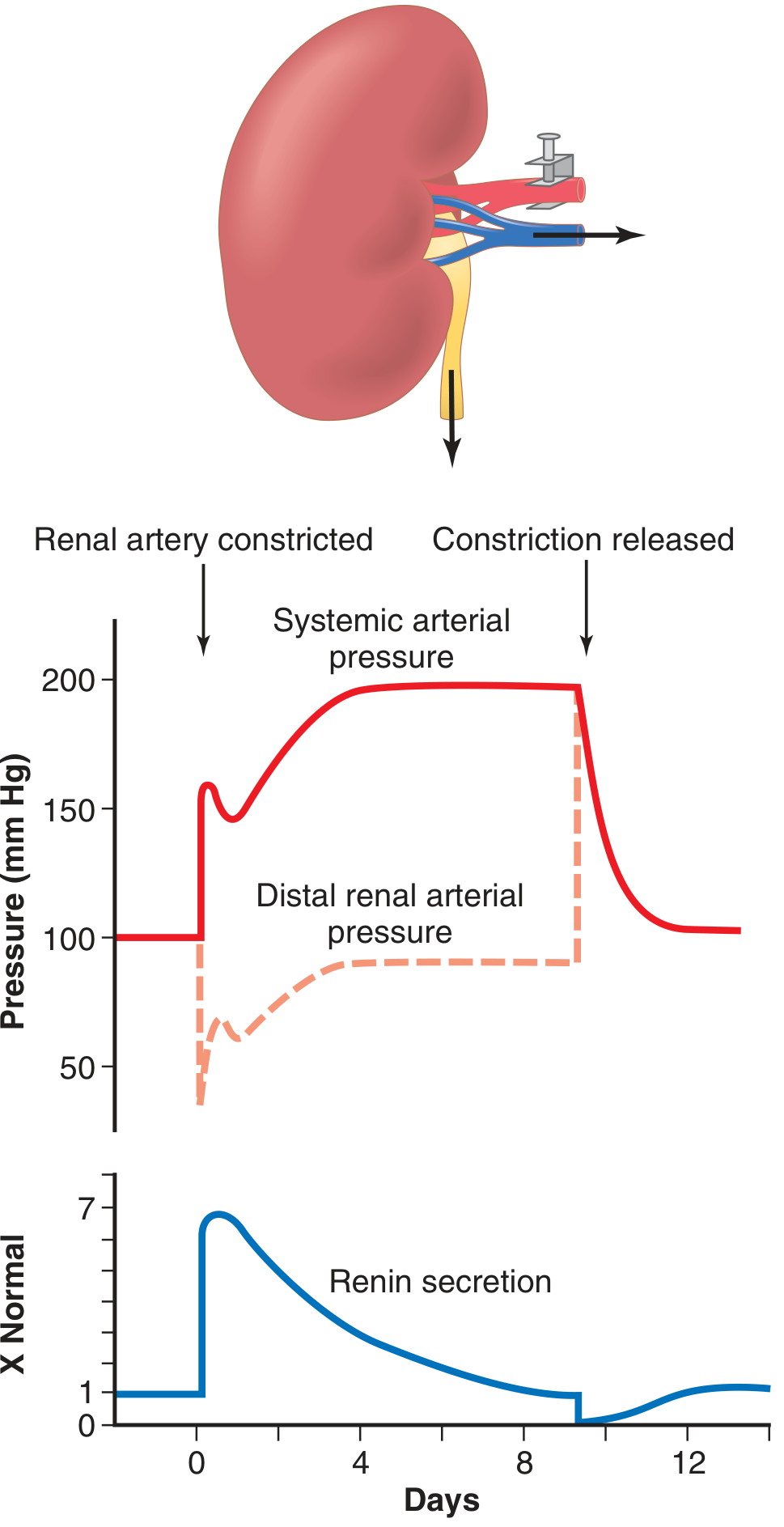
Reading the graph:
- Red solid line = Systemic (whole body) blood pressure - shoots UP
- Red dashed line = Pressure in the kidney after the clamp - drops first, then slowly recovers
- Blue line = Renin secretion - spikes very high at first, then comes back down
Two phases of BP rise:
| Phase | Time | Cause |
|---|---|---|
| Phase 1 - Fast | Within hours | Angiotensin II squeezes blood vessels |
| Phase 2 - Slow | Over 5-7 days | Salt and water retention raises blood volume |
Types of Renal Hypertension
1. 🔴 One-Kidney Goldblatt Hypertension
- One kidney is present + its artery is clamped/narrowed
- That single kidney keeps retaining salt and water
- BP stays high permanently until clamp removed
- Clinical example: Single kidney transplant with renal artery stenosis
2. 🟠 Two-Kidney Goldblatt Hypertension
- Both kidneys present, but artery to ONE is narrowed (e.g., atherosclerosis)
- The ischemic kidney releases renin
- Renin and angiotensin II travel to the NORMAL kidney and ALSO make it retain salt
- Both kidneys now hold on to salt → BP rises
- Clinical example: Renal artery stenosis (most common cause of renal hypertension)
3. 🟡 Patchy Kidney Disease
- Small damaged/scarred patches inside one or both kidneys
- These patches feel ischemic → keep releasing renin
- Rest of kidney retains salt
- Common in older people
- Example: Chronic kidney disease, multiple small infarcts
4. 🟢 Coarctation of Aorta
- Aorta is narrowed above the renal arteries (congenital defect in babies)
- Kidneys receive LOW pressure → release renin → BP rises in upper body
- Upper body BP very high, lower body BP normal
- Easy to diagnose: High BP in arms, low BP in legs
Common Real-Life Causes
| Cause | What Happens |
|---|---|
| Renal artery stenosis (atherosclerosis) | Artery to kidney narrows → kidney ischemia → renin release |
| Fibromuscular dysplasia | Artery wall thickens in young women → same effect |
| Chronic kidney disease | Damaged kidney tissue secretes renin |
| Renin-secreting tumor | JGA tumor constantly releases renin |
| Coarctation of aorta | Aorta narrowed → kidneys feel low pressure |
| Polycystic kidney disease | Cysts compress kidney arteries internally |
How Is It Different From Essential Hypertension?
| Essential (Primary) HTN | Renal HTN | |
|---|---|---|
| Cause | Unknown (genetic + lifestyle) | Known - kidney problem |
| Age | Usually middle-aged adults | Any age |
| Response to ACE inhibitors | Partial | Very good - since RAAS is the main driver |
| Curable? | No (manageable) | Often YES - fix the kidney problem → BP normalizes |
Treatment (Easy Version)
| Treatment | How it Helps |
|---|---|
| ACE inhibitors (e.g., enalapril) | Block conversion of Ang I → Ang II → less vasoconstriction |
| ARBs (e.g., losartan) | Block Angiotensin II receptors directly |
| Renal artery stenting/angioplasty | Open up the narrowed artery → restore blood flow → renin falls → BP normalizes |
| Surgery (bypass or nephrectomy) | For severe cases |
One Line to Remember Everything
"Kidney gets less blood → panics → releases Renin → Angiotensin II squeezes vessels + Aldosterone holds salt/water → Blood pressure rises throughout the body = Renal Hypertension"
Sources:
- Guyton and Hall Textbook of Medical Physiology, pp. 244-246 (Goldblatt Hypertension & RAAS)
- Medical Physiology - Boron & Boulpaep, p. 1255 (Box 40-2 Renal Hypertension)
Enteric nervous system in veryy simple word
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Got everything. Here is the full easy-word answer:
Enteric Nervous System (ENS) - Very Easy Words
What Is the ENS?
The Enteric Nervous System = The Brain of Your Gut.
Your gut (from the food pipe all the way to the anus) has its OWN private nervous system built right inside its walls. It does NOT need your brain to work - it can think and act completely on its own!
Fun fact: The ENS has more than 100 million nerve cells - that's more neurons than the entire spinal cord! This is why it is called the "Second Brain" or "Little Brain".
Where Is It?
It lives inside the wall of the gut - embedded in the layers of the intestine from the esophagus down to the anus.
It has two layers (plexuses):
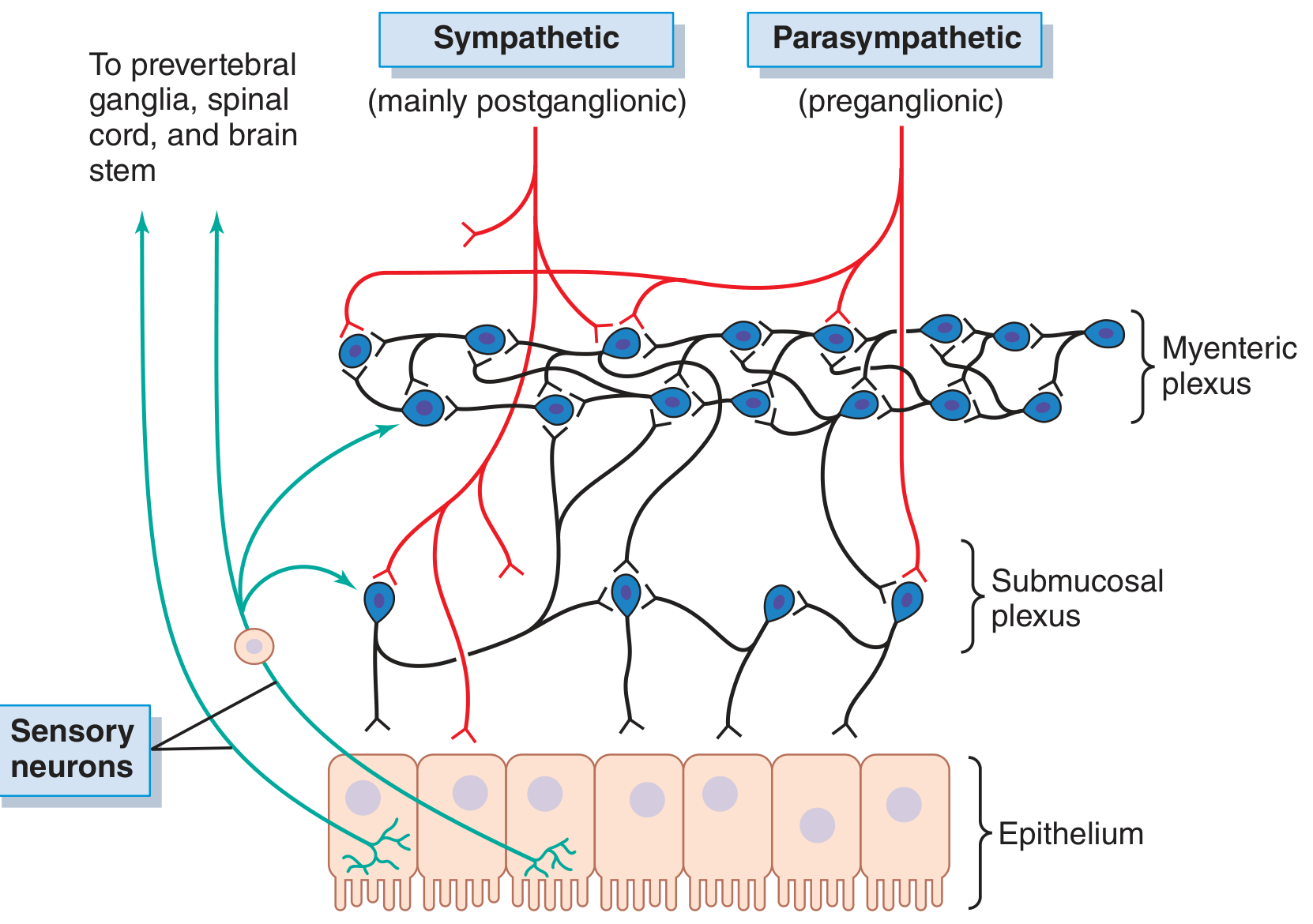
The Two Plexuses - "Two Networks"
Think of them as two departments working inside your gut wall:
1. 🟠 Myenteric Plexus (Auerbach's Plexus)
- Location: Between the two muscle layers (outer longitudinal + inner circular muscle)
- Job: Controls MOVEMENT of the gut - squeezing, pushing food along (peristalsis)
- Simple memory: "Myo = Muscle → Myenteric controls Movement"
When stimulated, it:
- Increases muscle tone (gut stays firm)
- Makes contractions stronger and faster
- Speeds up peristaltic waves (the wave that pushes food forward)
- Also relaxes sphincters (like the pyloric sphincter) so food can pass through
2. 🔵 Submucosal Plexus (Meissner's Plexus)
- Location: In the submucosa (inner layer, close to the gut lining)
- Job: Controls SECRETION - how much juice, enzymes, and mucus the gut produces + local blood flow
- Simple memory: "Sub = underneath the mucosa → controls Secretion"
Summary of the Two Plexuses
| Myenteric Plexus | Submucosal Plexus | |
|---|---|---|
| Other name | Auerbach's plexus | Meissner's plexus |
| Location | Between muscle layers | In submucosa (inner) |
| Main job | Movement / Motility | Secretion + Blood flow |
| Controls | Peristalsis, sphincters | Gland secretion, absorption |
Three Types of Neurons Inside ENS
Just like your brain, the ENS has three types of nerve cells:
| Neuron Type | Job | Simple Analogy |
|---|---|---|
| Sensory neurons | Detect stretch, chemicals, temperature in gut | Spies - report what's inside the gut |
| Interneurons | Connect and process the information | Managers - decide what to do |
| Motor neurons | Send commands to muscles and glands | Workers - actually squeeze or secrete |
Does the ENS Need the Brain?
NO! The ENS works independently. Even if you cut all the nerves from the brain to the gut, the gut will still:
- Move food (peristalsis)
- Secrete digestive juices
- React to food arriving
BUT - the brain CAN talk to the ENS through two systems:
| System | Effect on Gut | Easy Analogy |
|---|---|---|
| Parasympathetic (Vagus nerve = Rest & Digest) | INCREASES gut activity - more movement, more secretion | "Boss says GO! - speed up digestion" |
| Sympathetic (Fight or Flight) | DECREASES gut activity - slows everything down | "Emergency! Stop digesting, run!" |
Key Neurotransmitters (Chemical Messengers) - Easy List
The ENS uses 25+ chemicals to send messages. The most important ones:
| Chemical | Effect |
|---|---|
| Acetylcholine | EXCITES gut - more movement and secretion |
| Norepinephrine | INHIBITS gut - slows everything |
| Serotonin (5-HT) | Triggers peristalsis (90% of body's serotonin is in the GUT!) |
| Nitric oxide (NO) | Relaxes smooth muscle - relaxes sphincters |
| VIP (Vasoactive Intestinal Peptide) | Relaxes muscle, increases secretion |
| Substance P | Excites movement |
What Does the ENS Actually Control?
| Function | How ENS Helps |
|---|---|
| Peristalsis | Myenteric plexus coordinates wave contractions to push food forward |
| Sphincter control | Opens/closes pyloric, ileocecal, and anal sphincters at the right time |
| Secretion of enzymes, mucus, water | Submucosal plexus tells glands when and how much to secrete |
| Blood flow to gut | Increases blood flow when digestion is active |
| Absorption | Coordinates how much is absorbed from the gut lining |
| Local reflexes | e.g., distension in one area automatically triggers peristalsis without asking the brain |
The "Gut-Brain Axis" (Bonus Easy Concept)
The ENS and the brain constantly talk to each other in both directions:
Brain ←→ Vagus Nerve ←→ ENS (Gut)
- Brain → Gut: Stress makes your gut speed up (nervous diarrhea!) or slow down
- Gut → Brain: Gut produces serotonin, which affects your mood
This is why stress causes stomach aches and why people with depression often have gut problems!
Diseases When ENS Goes Wrong
| Disease | ENS Problem |
|---|---|
| Hirschsprung disease | No ENS neurons in part of colon → that part cannot relax → severe constipation in babies |
| Irritable Bowel Syndrome (IBS) | ENS hypersensitive → overreacts to normal stimuli |
| Gastroparesis | ENS in stomach damaged (e.g., diabetes) → stomach doesn't empty properly |
| Achalasia | Loss of inhibitory neurons in esophagus → lower esophageal sphincter doesn't open |
One-Line Summary
"The ENS is a complete nervous system (100 million neurons!) inside the gut wall. It has two networks - Myenteric plexus (controls movement) and Submucosal plexus (controls secretion). It works independently but also receives instructions from the brain via parasympathetic (speeds up) and sympathetic (slows down) nerves."
Sources:
- Guyton and Hall Textbook of Medical Physiology, pp. 778-779 (Neural Control of GI Function - ENS)
- Ganong's Review of Medical Physiology, 26th Edition, p. 274 (Enteric Nervous System)
Fight and flight
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Here is the complete, super simple explanation:
Fight or Flight Response - Very Easy Words
What Is It?
Fight or Flight = Your body's emergency alarm system.
Imagine you are walking and suddenly a wild dog runs at you. In less than a second, your body transforms into a survival machine - your heart races, muscles tense, pupils widen, and you are ready to either fight the dog or run away fast.
This automatic whole-body response is called the Fight or Flight Response.
It was first described by Walter Cannon in 1915.
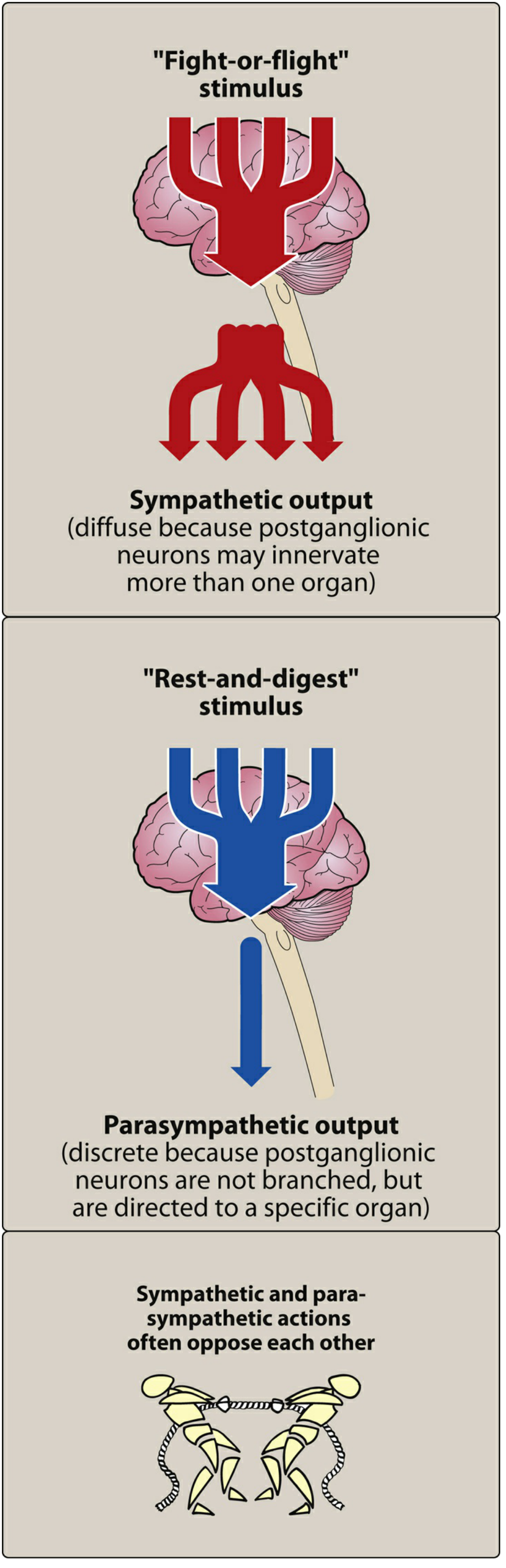
Who Triggers It?
The Sympathetic Nervous System (SNS) + Adrenal Gland
When your brain senses danger:
Danger/Fear/Stress
↓
Hypothalamus in brain sends ALARM signal
↓
Sympathetic Nervous System activates EVERYWHERE at once
↓
Adrenal Medulla releases EPINEPHRINE (Adrenaline) into blood
↓
Every organ in your body responds in seconds!
What Happens to Each Organ? (Body-by-Body)
🫀 Heart
| Normal | Fight or Flight |
|---|---|
| 60-80 beats/min | Goes UP - 100-180 beats/min |
| Normal force | Pumps HARDER |
Why? Muscles need more blood to fight or run.
🫁 Lungs
| Normal | Fight or Flight |
|---|---|
| Normal airway | Bronchioles WIDEN (bronchodilation) |
Why? Wider airways = more oxygen in with each breath = more energy available.
👁️ Eyes
| Normal | Fight or Flight |
|---|---|
| Normal pupil | Pupils DILATE (get bigger) |
Why? Bigger pupils = let in more light = see danger better.
💪 Muscles
| Normal | Fight or Flight |
|---|---|
| Normal blood flow | Blood flow INCREASES to skeletal muscles |
Why? Muscles need oxygen and glucose to fight or run.
🩸 Blood Vessels
| Location | What Happens |
|---|---|
| Skin and gut | CONSTRICT (less blood) |
| Heart and muscle | DILATE (more blood) |
Why? In an emergency, blood is redirected from non-essential organs (gut, skin) to essential ones (heart, muscles, brain).
🍬 Blood Sugar (Glucose)
| Normal | Fight or Flight |
|---|---|
| Normal glucose | Glucose RISES in blood |
Why? Liver breaks down glycogen → releases glucose → instant energy for muscles. Also insulin secretion is suppressed so glucose stays in blood longer.
😰 Sweat Glands
| Normal | Fight or Flight |
|---|---|
| Minimal sweating | SWEATING increases |
Why? Cool the body down during intense activity.
💇 Skin
- Piloerection = hair stands up (goosebumps!) - primitive defence mechanism
- Skin blood vessels constrict → skin becomes pale
- Also reduces bleeding if wounded
🧠 Brain
- Alertness increases sharply
- Non-essential thinking (creativity, digestion thoughts) is suppressed
- Focus becomes narrow and sharp
🍽️ Gut (Digestive System)
| Normal | Fight or Flight |
|---|---|
| Active digestion | SHUTS DOWN - motility decreases, secretion decreases |
Why? Digestion is not urgent in an emergency - that energy goes to muscles instead. (That is why you feel nauseous or lose appetite when very stressed!)
🚽 Bladder
- Internal sphincter contracts (holds urine in)
- Detrusor muscle relaxes
You don't want to pee while running from danger!
The Two Chemicals Responsible
| Chemical | Source | How it Works |
|---|---|---|
| Norepinephrine | Sympathetic nerve endings (released directly onto organs) | Fast, local effect |
| Epinephrine (Adrenaline) | Adrenal medulla (released into blood) | Slower but body-wide effect |
Both bind to adrenergic receptors (α and β) on target organs to produce the fight or flight effects.
Fight or Flight vs. Rest and Digest - Side by Side
| Body Part | Fight or Flight (Sympathetic) | Rest and Digest (Parasympathetic) |
|---|---|---|
| Heart rate | ↑ Increases | ↓ Decreases |
| Airways | Dilate (open up) | Constrict (narrow) |
| Pupils | Dilate (widen) | Constrict (narrow) |
| Gut activity | ↓ Decreases | ↑ Increases |
| Salivation | ↓ Dry mouth | ↑ Increases |
| Blood glucose | ↑ Rises | ↓ Falls (insulin released) |
| Blood to muscles | ↑ Increases | ↓ Decreases |
| Bladder | Holds urine | Empties (micturition) |
Easy Analogy - "The Factory Emergency"
Imagine a factory (your body) running normally. Suddenly the fire alarm goes off:
- All machines speed up (heart, lungs)
- Power is redirected to important areas (muscles, brain)
- Non-essential departments close (gut, skin, kidneys reduce work)
- Emergency exits open (bronchi dilate, blood vessels to muscles open)
- Workers sweat from working hard
- The factory runs at MAXIMUM capacity for a short burst
That is exactly what your body does in fight or flight!
What Happens Afterward?
Once the danger is gone:
- Parasympathetic takes over (Rest and Digest)
- Heart slows down
- Breathing normalizes
- Digestion resumes
- You feel tired, shaky, or relieved (post-adrenaline crash)
Clinical Relevance
| Condition | Connection to Fight or Flight |
|---|---|
| Panic attacks | Fight or flight triggered without real danger |
| Phaeochromocytoma | Adrenal tumor releasing excess epinephrine → constant fight or flight symptoms (hypertension, sweating, racing heart) |
| PTSD | Fight or flight system stuck in "on" mode |
| Asthma | Epinephrine (adrenaline) relieves attacks by dilating bronchi |
| Beta-blockers | Drugs that BLOCK the fight or flight effects on the heart |
One-Line Summary
"Fight or flight = Sympathetic nervous system + Adrenaline activating the WHOLE body at once to prepare for danger: Heart faster, breathing deeper, pupils wider, muscles powered up, digestion OFF, glucose released - all in seconds."
Sources:
- Medical Physiology - Boron & Boulpaep, p. 520 (Fight-or-Flight Response)
- Lippincott Illustrated Reviews Pharmacology, pp. 125-126 (Sympathetic Nervous System Functions)
In very easy language
Fight or Flight - Simplest Possible Words 🚨
The Story Version
Imagine you are walking alone at night. Suddenly a big dog jumps out and barks at you.In that ONE second - before you even think - your body has ALREADY changed. Your heart is pounding, you are breathing fast, your eyes are wide open, your muscles are tense.That is Fight or Flight.
Your body is saying: "Danger! Either FIGHT this dog or RUN away - choose fast!"
Who Presses the Alarm Button?
Your brain (hypothalamus) sees the danger first.
It immediately sends one message to the whole body:
"EMERGENCY! Everyone get ready NOW!"
This message travels through the Sympathetic Nervous System - like pressing one button that switches on ALL the lights in a building at once.
The adrenal gland (sitting on top of your kidney) also dumps Adrenaline (Epinephrine) straight into your blood - like pouring fuel on a fire.
What Happens to Your Body - Like a Checklist ✅
Things that SPEED UP or OPEN UP (to help you fight/run):
| What | What Happens | Why |
|---|---|---|
| ❤️ Heart | Beats FASTER and HARDER | Pump more blood to muscles |
| 🫁 Lungs | Airways OPEN WIDER | Take in more oxygen |
| 👁️ Eyes | Pupils get BIG | See better in the dark/danger |
| 💪 Muscles | Get MORE blood | Ready to fight or run |
| 🍬 Blood sugar | RISES | Instant energy for muscles |
| 😰 Sweat | INCREASES | Cool the body down |
Things that SLOW DOWN or CLOSE (not needed in emergency):
| What | What Happens | Why |
|---|---|---|
| 🍽️ Stomach/Gut | SHUTS DOWN | Digestion not needed right now |
| 💧 Saliva | DRY MOUTH | Not eating right now |
| 🚽 Bladder | HOLDS urine | Can't stop to pee! |
| 🩸 Skin blood flow | DECREASES | Blood goes to muscles instead |
The Two Chemicals Doing All This
| Chemical | Think of it as... | What it does |
|---|---|---|
| Adrenaline (Epinephrine) | Rocket fuel poured into blood | Affects the whole body at once |
| Noradrenaline (Norepinephrine) | Local fire starters at each organ | Acts directly at each organ |
Super Simple Diagram
🐕 DANGER SEEN
↓
🧠 Brain says "EMERGENCY!"
↓
⚡ Sympathetic nerves fire everywhere
↓
💉 Adrenaline released into blood
↓
❤️ Heart races
🫁 Lungs open
💪 Muscles charged
🍬 Sugar released
👁️ Eyes wide
🍽️ Gut stops
↓
✅ Body ready to FIGHT or RUN
After the Danger is Gone...
The Parasympathetic system takes over - this is "Rest and Digest."
- Heart slows down
- Breathing normalizes
- Gut starts working again
- You feel tired and shaky - that is the adrenaline wearing off
One Sentence to Remember Everything
"When danger comes → brain panics → adrenaline floods the body → heart races, lungs open, muscles charged, eyes widen, gut stops → you are ready to FIGHT or RUN."
Compare the Two Systems in 5 Words Each
| Sympathetic = "Fight or Flight" | Parasympathetic = "Rest and Digest" |
|---|---|
| Emergency, speed up, run! | Relax, eat, sleep, recover |
Write thw regulation of gastric secretion in easy word
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Got everything. Here is the complete, easy-language explanation:
Regulation of Gastric Secretion - Easy Words
First - What Does the Stomach Secrete?
When you eat, your stomach produces:
- HCl (Hydrochloric acid) - kills bacteria, activates enzymes
- Pepsinogen - enzyme that digests proteins
- Mucus - protects stomach wall from its own acid
- Intrinsic factor - helps absorb Vitamin B12
All of this is controlled in 3 phases - like a 3-step system that starts even before food reaches the stomach.
The Big Picture Diagram
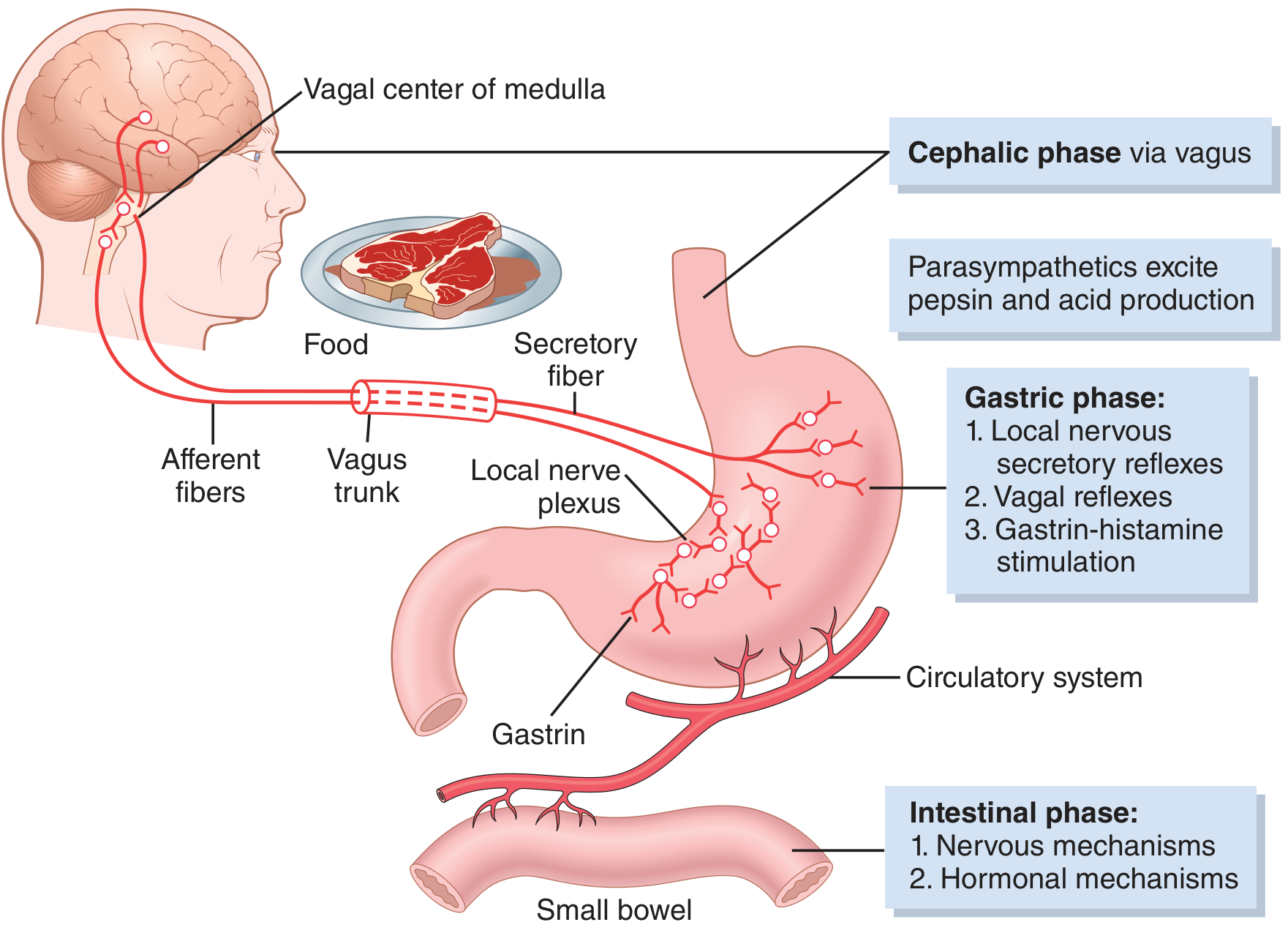
The 3 Phases of Gastric Secretion
🧠 Phase 1 - CEPHALIC PHASE ("Head Phase")
= Before food even enters the stomach
Trigger: Just the sight, smell, thought, or taste of food
Imagine smelling freshly cooked biryani - your mouth waters and your stomach starts producing acid. That is the cephalic phase!
How it works:
See/Smell/Think about food
↓
Brain (Cerebral cortex + Hypothalamus) gets excited
↓
Sends signals via VAGUS NERVE (cranial nerve X)
↓
Vagus releases Acetylcholine in the stomach
↓
Stomach wall starts secreting HCl, Pepsinogen and Mucus
Key messenger: Vagus nerve (Parasympathetic)
Contribution: About 30% of total gastric secretion
Memory: "Cephalic = head thinking about food = vagus gets excited"
🍖 Phase 2 - GASTRIC PHASE ("Stomach Phase")
= When food actually enters the stomach
Trigger: Food (especially proteins) physically distending and touching the stomach wall
This is the BIGGEST phase - contributes 60% of total secretion
How it works (3 sub-mechanisms):
a) Local Reflex (Enteric nervous system)
Food stretches stomach wall
↓
Local nerve plexus in stomach wall fires
↓
Directly stimulates parietal cells → more HCl
b) Vagovagal Reflex (Brain loop)
Stretch receptors in stomach wall
↓
Signal goes UP to brain via vagus
↓
Brain sends signal back DOWN via vagus
↓
More acid secretion
c) Gastrin-Histamine Mechanism (The most important!) ⭐
Proteins in food stimulate G cells (in antrum of stomach)
↓
G cells release GASTRIN hormone into blood
↓
Gastrin travels to ECL cells (in body of stomach)
↓
ECL cells release HISTAMINE
↓
Histamine stimulates PARIETAL CELLS to secrete HCl
Simple: Protein → Gastrin → Histamine → HCl This is why antacids (H₂ blockers like ranitidine) block histamine to reduce acid!
Key messengers: Gastrin + Histamine + Acetylcholine (the "Big 3" stimulators)
🫁 Phase 3 - INTESTINAL PHASE
= When food enters the small intestine
Trigger: Food (especially proteins) entering the duodenum
Contributes only ~10% of total secretion
- Duodenum releases a small amount of gastrin → mildly stimulates stomach to keep secreting
- But this phase is mainly important for INHIBITION (see below)
🛑 INHIBITION of Gastric Secretion (How the stomach turns OFF)
This is equally important - the stomach must STOP making acid when:
- The stomach is empty
- The duodenum is already full / too acidic / has fat
How inhibition happens:
| Trigger | Mechanism | Inhibitor Released |
|---|---|---|
| Acid in duodenum (pH <2) | Enterogastric reflex | Secretin → stops gastrin → reduces acid |
| Fat in duodenum | Hormones from small intestine | GIP (Gastric Inhibitory Peptide) → reduces acid |
| Stomach pH too low (pH <1.5) | Local feedback | Somatostatin from D-cells → shuts off gastrin |
| Duodenum overloaded | Reverse nervous reflex | Sympathetic reflex inhibits stomach |
Somatostatin = the "OFF switch" - when stomach acid gets too high, D-cells release somatostatin → blocks gastrin release → acid stops
The Three Stimulators (Must Know! ⭐)
There are 3 chemicals that directly stimulate parietal cells to make HCl:
| Stimulator | Source | Type |
|---|---|---|
| Acetylcholine (ACh) | Vagus nerve | Nerve signal |
| Gastrin | G cells (antrum) | Hormone |
| Histamine | ECL cells | Local chemical (paracrine) |
All three work TOGETHER - if you block any one of them, acid production drops.
This is the basis of peptic ulcer drugs:
- Atropine → blocks ACh
- H₂ blockers (ranitidine) → blocks histamine
- Proton pump inhibitors (omeprazole) → blocks the acid pump directly
Summary Table - All 3 Phases
| Phase | When | Trigger | Main Messenger | % of Total Secretion |
|---|---|---|---|---|
| Cephalic | Before food enters stomach | Sight/smell/thought of food | Vagus nerve (ACh) | 30% |
| Gastric | Food in stomach | Protein + distension | Gastrin → Histamine | 60% |
| Intestinal | Food in small intestine | Protein in duodenum | Small gastrin release | 10% |
Super Simple Story Version 📖
One-Line Memory
"Cephalic (brain-vagus, 30%) → Gastric (gastrin-histamine, 60%) → Intestinal (10%) → then INHIBITION by somatostatin, secretin, GIP when gut is full"
Source: Guyton and Hall Textbook of Medical Physiology, pp. 803-804 (Phases of Gastric Secretion & Regulation)
This is a shared conversation. Sign in to Orris to start your own chat.