EXPLAIN ME 10 COMMON HEART DISEASE WITH ECG CHANGES AND ECG IMAGES OF THOSE DISEASE
Reading File
Finding Sources
Searching the Web
10 common heart diseases ECG changes electrocardiogram findings
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Searching the Web
ECG images atrial fibrillation ventricular hypertrophy heart block WPW syndrome pulmonary embolism
Loading Image
Loading Image
Searching the Web
ECG atrial fibrillation irregularly irregular no P waves example image
Loading Image
Searching the Web
ECG complete heart block third degree ventricular hypertrophy WPW delta wave pulmonary embolism S1Q3T3 images
Loading Image
Loading Image
Finding Sources
Searching the Web
ECG LVH left ventricular hypertrophy voltage criteria image AND heart failure ECG low voltage
Loading Image
Loading Image
10 Common Heart Diseases: ECG Changes with Images
1. ST-Elevation Myocardial Infarction (STEMI)
Pathophysiology: Complete occlusion of a coronary artery causes transmural ischemia with immediate electrical changes.
ECG Changes:
- ST-segment elevation ≥1 mm in two contiguous leads (the defining feature)
- Hyperacute T waves (tall, broad, peaked) in the earliest minutes
- Pathologic Q waves (>40 ms wide, >25% QRS height) developing within 8-12 hours - mark irreversible necrosis
- Reciprocal ST depression in leads opposite to the infarct zone
- Lead-based localization (from Rosen's Emergency Medicine):
| Location | Leads with ST Elevation |
|---|---|
| Anterior STEMI | V1-V4 |
| Lateral STEMI | I, aVL, V5, V6 |
| Inferior STEMI | II, III, aVF |
| Right ventricular AMI | V4R |
| Posterior AMI | V8, V9 (or V1-V3 depression) |
ECG Image - Anterolateral STEMI (ST elevation in V2-V6, I, aVL; in-stent thrombosis):
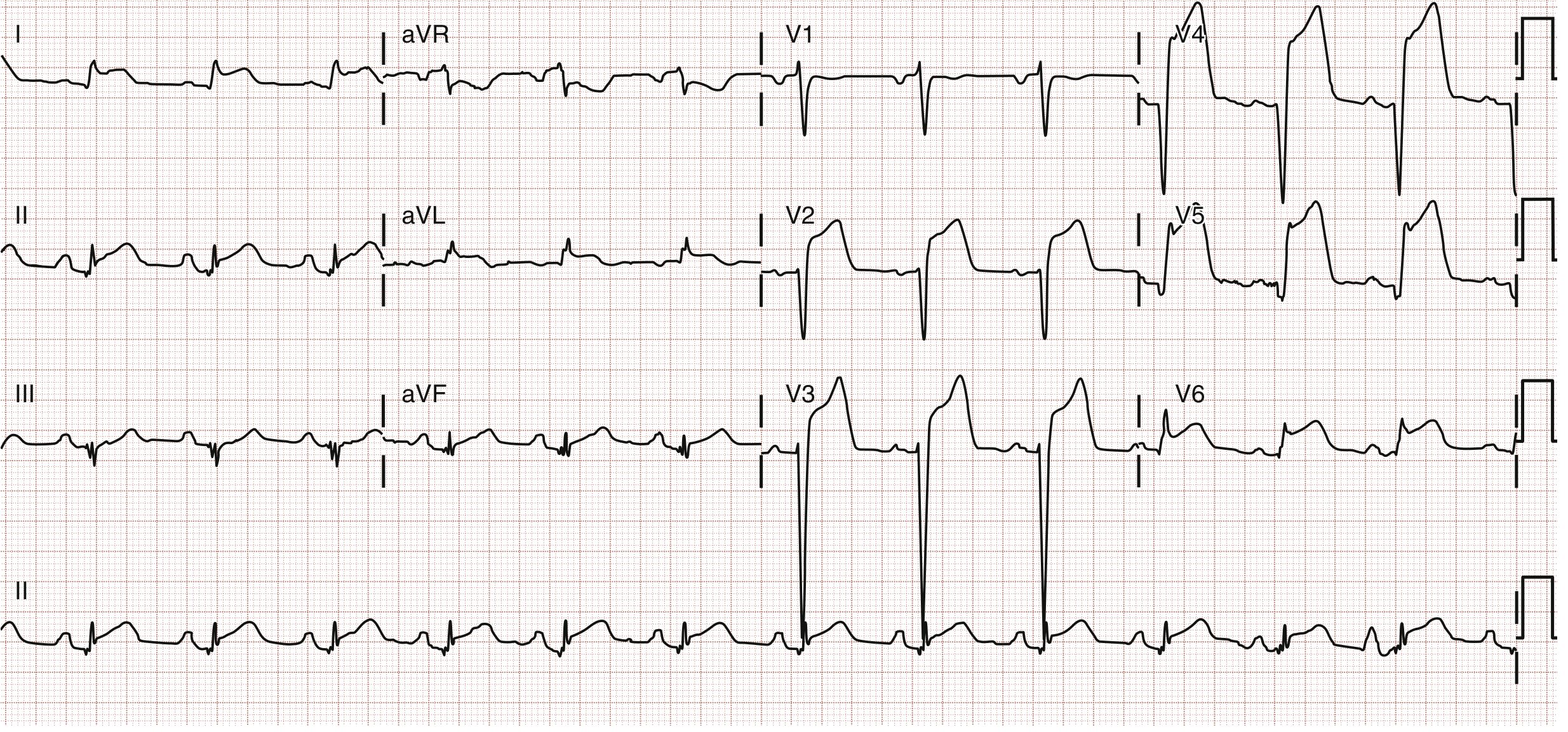
Fig: Anterolateral ST segment elevation myocardial infarction (STEMI). STE is seen in V2-V6, I, and aVL. Patient had in-stent thrombosis of the LAD. - Rosen's Emergency Medicine
ECG Image - Inferior STEMI with ST elevation in II, III, aVF and right ventricular involvement in V1:
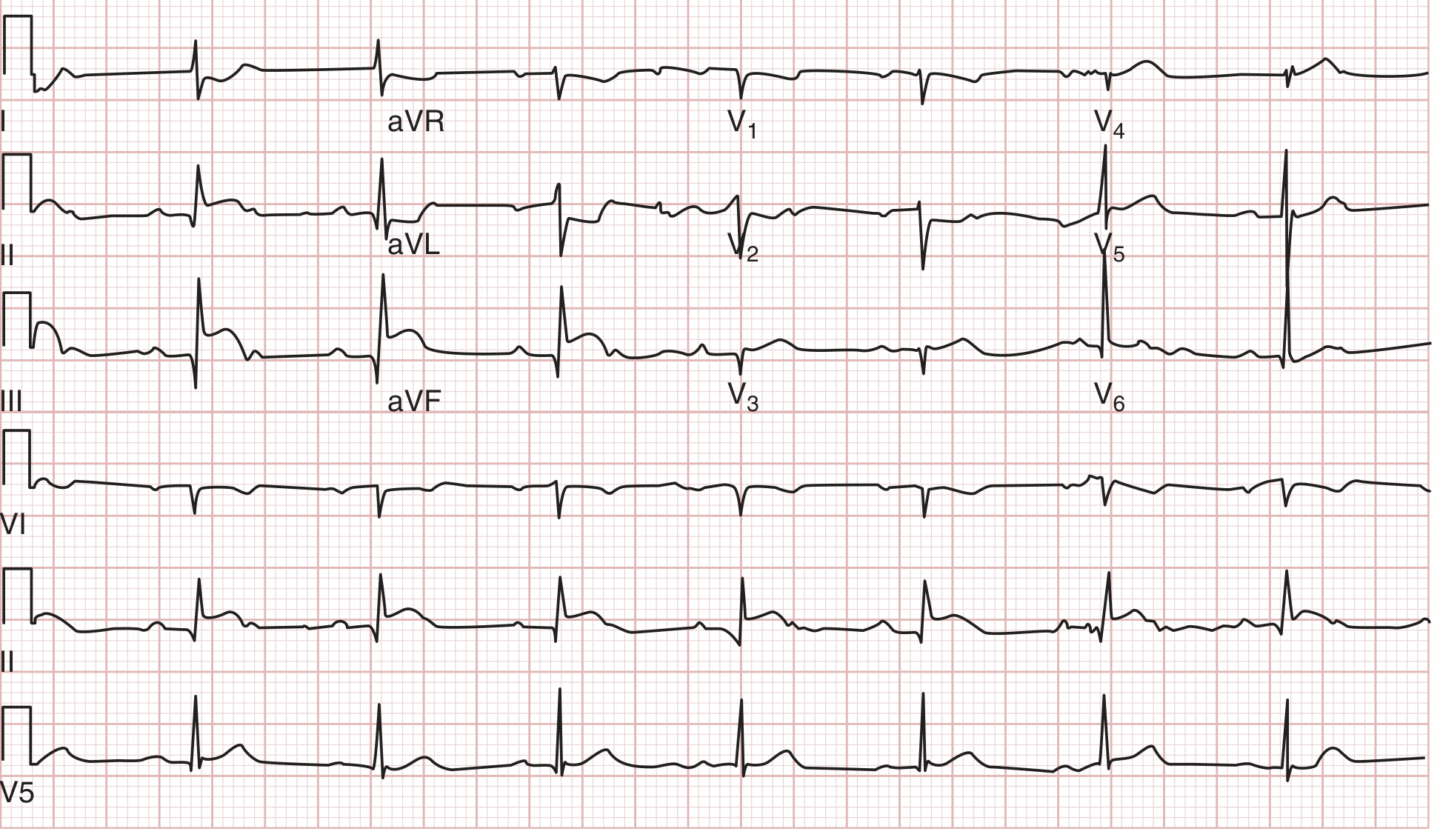
Fig: Inferior STEMI from right coronary artery (RCA) occlusion. Note ST elevation in leads II, III, aVF, and V1 (right ventricular involvement). - Tintinalli's Emergency Medicine
2. Non-ST-Elevation Myocardial Infarction / Unstable Angina (NSTEMI/UA)
Pathophysiology: Partial coronary occlusion causing subendocardial ischemia without full-thickness necrosis.
ECG Changes:
- ST depression ≥0.5 mm in two or more contiguous leads (most common pattern)
- T-wave inversion - symmetric, deep inversions (particularly V1-V4 in Wellens' syndrome = critical LAD stenosis)
- Transient ST changes that may normalize between pain episodes
- Pseudonormalization of a previously inverted T wave during ischemia
- No pathologic Q waves and no ST elevation (by definition)
- A completely normal ECG does NOT exclude NSTEMI - troponins are essential
Wellens' Pattern (critical LAD stenosis):
- Type A: biphasic T waves in V2-V3
- Type B: deeply inverted symmetric T waves in V2-V3 (more specific, ~75% sensitivity)
ECG Image - NSTEMI/ACS with Widespread ST Depression and aVR Elevation:
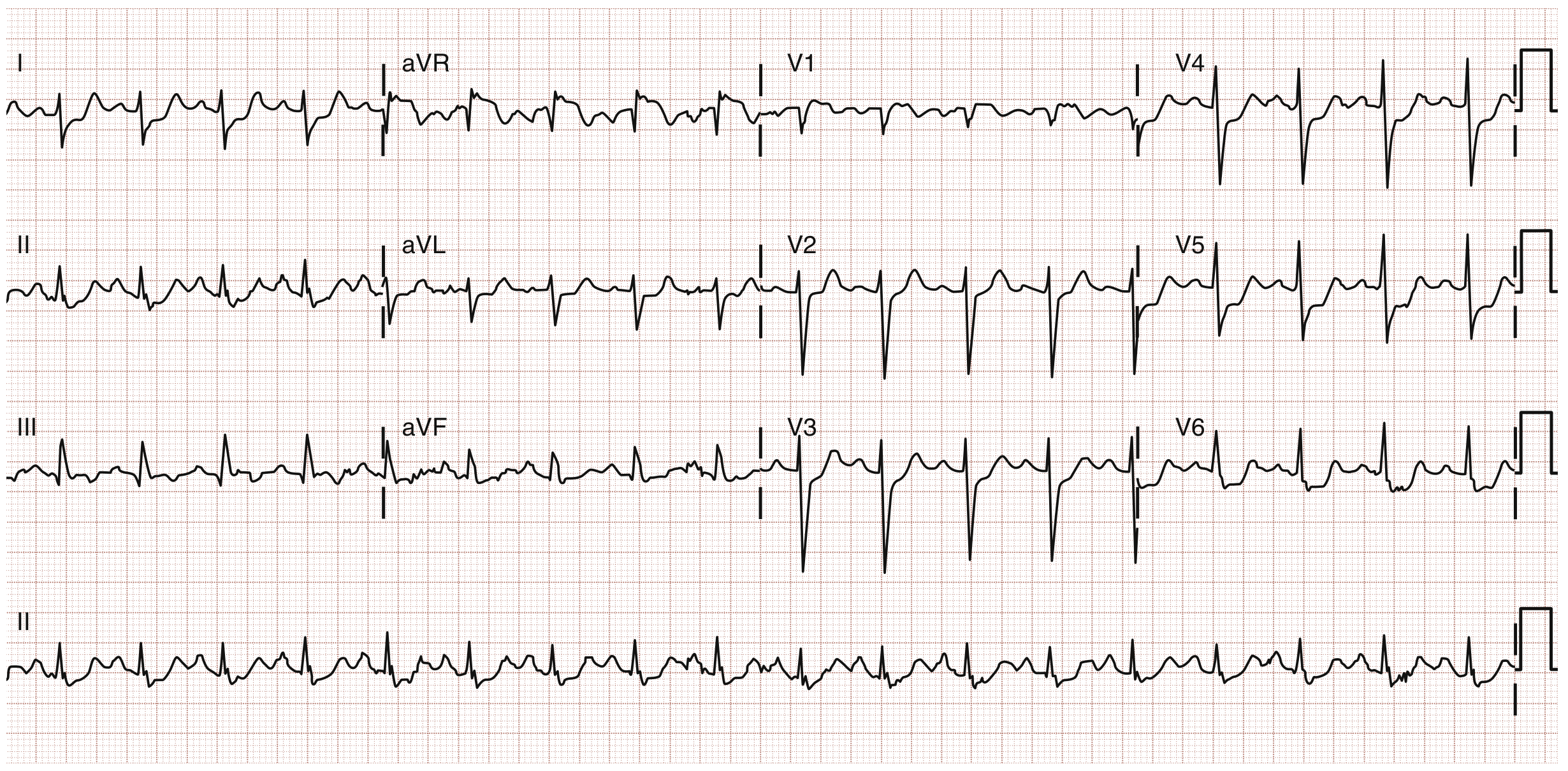
Fig: ST elevation in lead aVR with widespread ST depression - a pattern suggesting left main coronary artery disease or proximal LAD occlusion. - Tintinalli's Emergency Medicine
3. Atrial Fibrillation (AF)
Pathophysiology: Chaotic electrical activity in the atria replaces organized P waves with fibrillatory impulses; the AV node conducts irregularly.
ECG Changes (from Tintinalli's Emergency Medicine, Table 18-8):
- Absence of discernible P waves - replaced by chaotic fibrillatory baseline (f-waves at 350-600/min)
- Irregularly irregular ventricular rhythm - the hallmark finding, no pattern to R-R intervals
- Narrow QRS complexes (unless pre-existing bundle branch block or WPW)
- Ventricular rate typically 110-140 bpm in uncontrolled AF
- If conducted via accessory pathway (WPW + AF): wide, bizarre, irregular QRS at very rapid rates (>200 bpm) - life-threatening
ECG Image - Atrial Fibrillation:

Fig: Atrial fibrillation (top strip) - note absent P waves, chaotic baseline, and irregularly irregular QRS complexes. Compared with atrial flutter (middle) and multifocal atrial tachycardia (bottom). - Healio / Learn the Heart
4. Acute Pericarditis
Pathophysiology: Inflammation of the pericardium causes diffuse epicardial injury, producing characteristic widespread ECG changes that evolve through 4 stages.
ECG Changes - 4 Stages (from Fuster and Hurst's The Heart):
- Stage 1 (hours-days): Diffuse ST-segment elevation (concave/saddle-shaped) in ALL leads except aVR and V1 + PR-segment depression (very specific finding) - ST elevation in aVR is opposite
- Stage 2 (days): ST and PR normalize
- Stage 3 (1-3 weeks): Diffuse T-wave inversions
- Stage 4 (weeks-months): ECG returns to baseline
Key distinctions from STEMI:
- ST elevation is diffuse (not territory-specific)
- Concave rather than convex ST morphology
- PR depression is characteristic (rarely seen in STEMI)
- No reciprocal ST depression (except aVR)
- No Q waves
ECG Image - Acute Pericarditis (Stage 1):
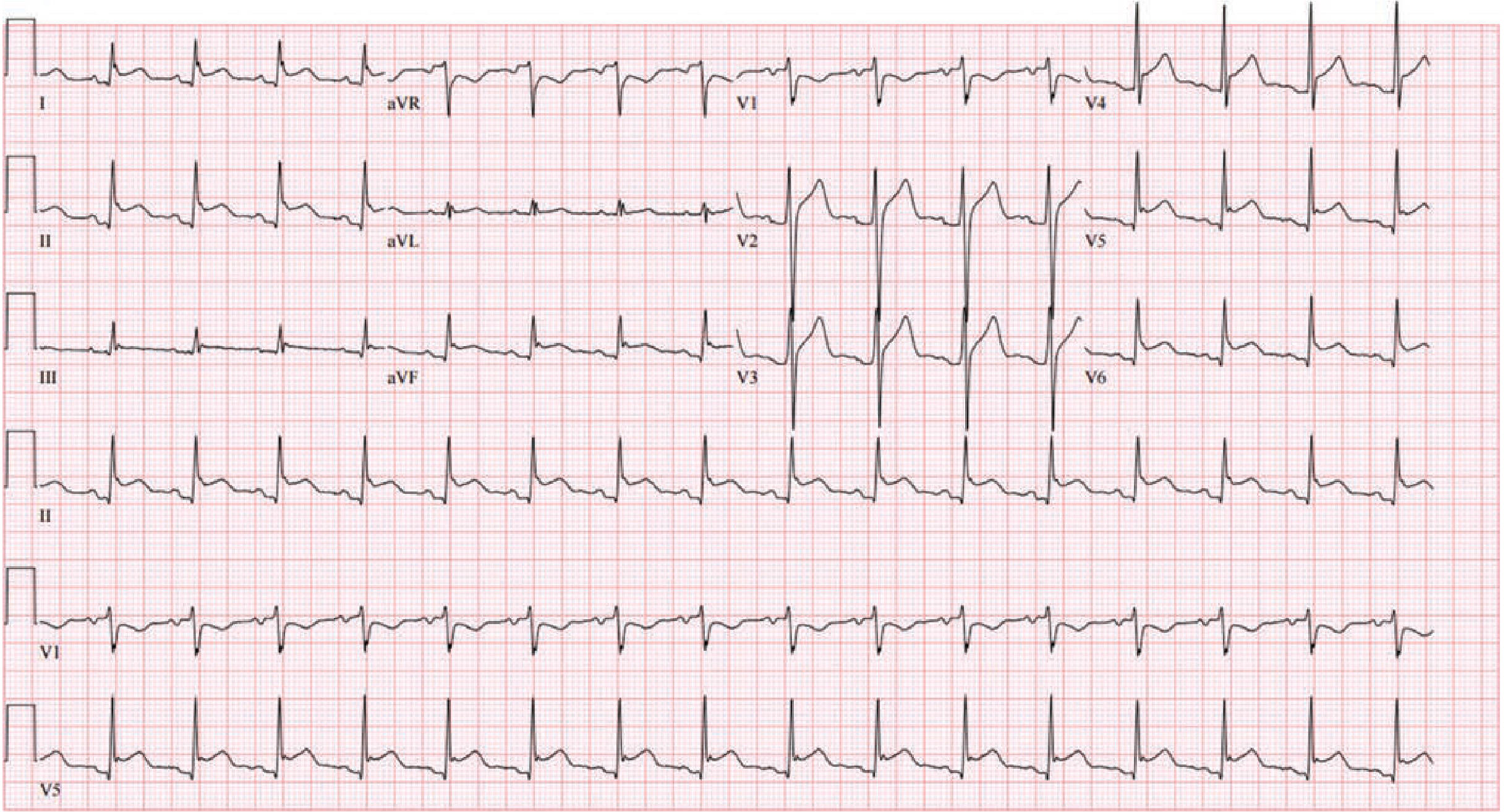
Fig: Stage 1 acute pericarditis. Diffuse ST-segment elevation with PR-segment depression in a non-territory-specific distribution. Note ST depression with PR elevation in aVR (reciprocal). - Fuster and Hurst's The Heart, 15th Ed.
5. Left Ventricular Hypertrophy (LVH)
Pathophysiology: Chronic pressure overload (hypertension, aortic stenosis) or volume overload increases LV muscle mass, increasing electrical voltage and altering repolarization.
ECG Changes:
- Increased QRS voltage (the primary feature):
- Sokolow-Lyon criterion: S in V1 + R in V5 or V6 >35 mm
- Cornell criterion: R in aVL + S in V3 >28 mm (men) or >20 mm (women)
- R in aVL >11-12 mm alone (modified Cornell)
- Left axis deviation (LAD)
- Prolonged QRS duration (up to 120 ms)
- LV strain pattern - ST depression and T-wave inversion in left-sided leads (I, aVL, V5, V6), representing secondary repolarization abnormality
- Left atrial enlargement - broad, notched P wave (P mitrale) in lead II; biphasic P in V1
ECG Image - Severe LVH with Strain Pattern:
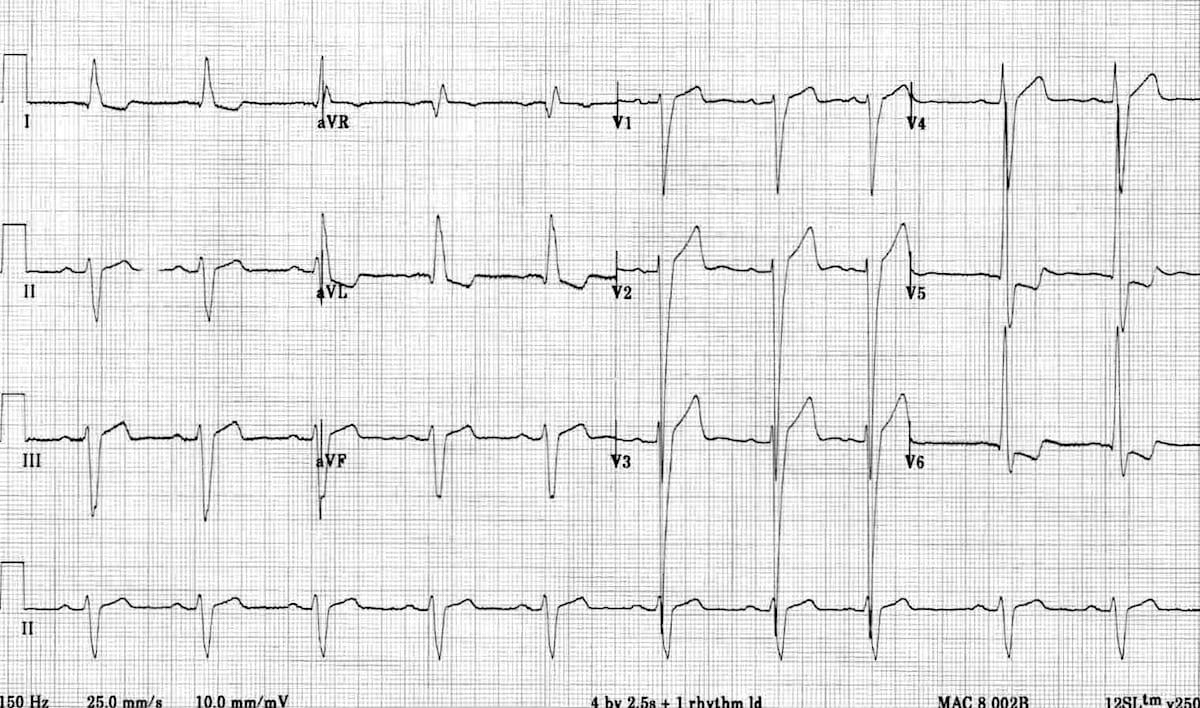
Fig: Severe LVH - note extremely tall R waves in V5 and deep S waves in V2 meeting Sokolow-Lyon criteria, with ST depression/T-inversion in lateral leads (strain pattern). - LITFL ECG Library
6. Complete (Third-Degree) AV Heart Block
Pathophysiology: No conduction passes from atria to ventricles. The atria and ventricles beat independently from separate pacemakers.
ECG Changes:
- Complete AV dissociation - P waves and QRS complexes are completely independent (P waves march through at their own rate, QRS at a slower escape rate)
- Regular P-P interval (normal atrial rate, 60-100 bpm)
- Regular R-R interval (escape rhythm, bradycardic)
- Escape QRS morphology:
- Junctional escape (narrow QRS, rate ~40-60 bpm) if block is at AV node
- Ventricular escape (wide, bizarre QRS, rate ~20-40 bpm) if block is below the His bundle - more dangerous
- No relationship between P waves and QRS - P waves may fall before, within, or after QRS
- Causes: inferior MI (often transient), Lyme carditis, digoxin toxicity, idiopathic fibrosis
ECG Image - Inferior STEMI with AV Block (showing dissociation pattern):
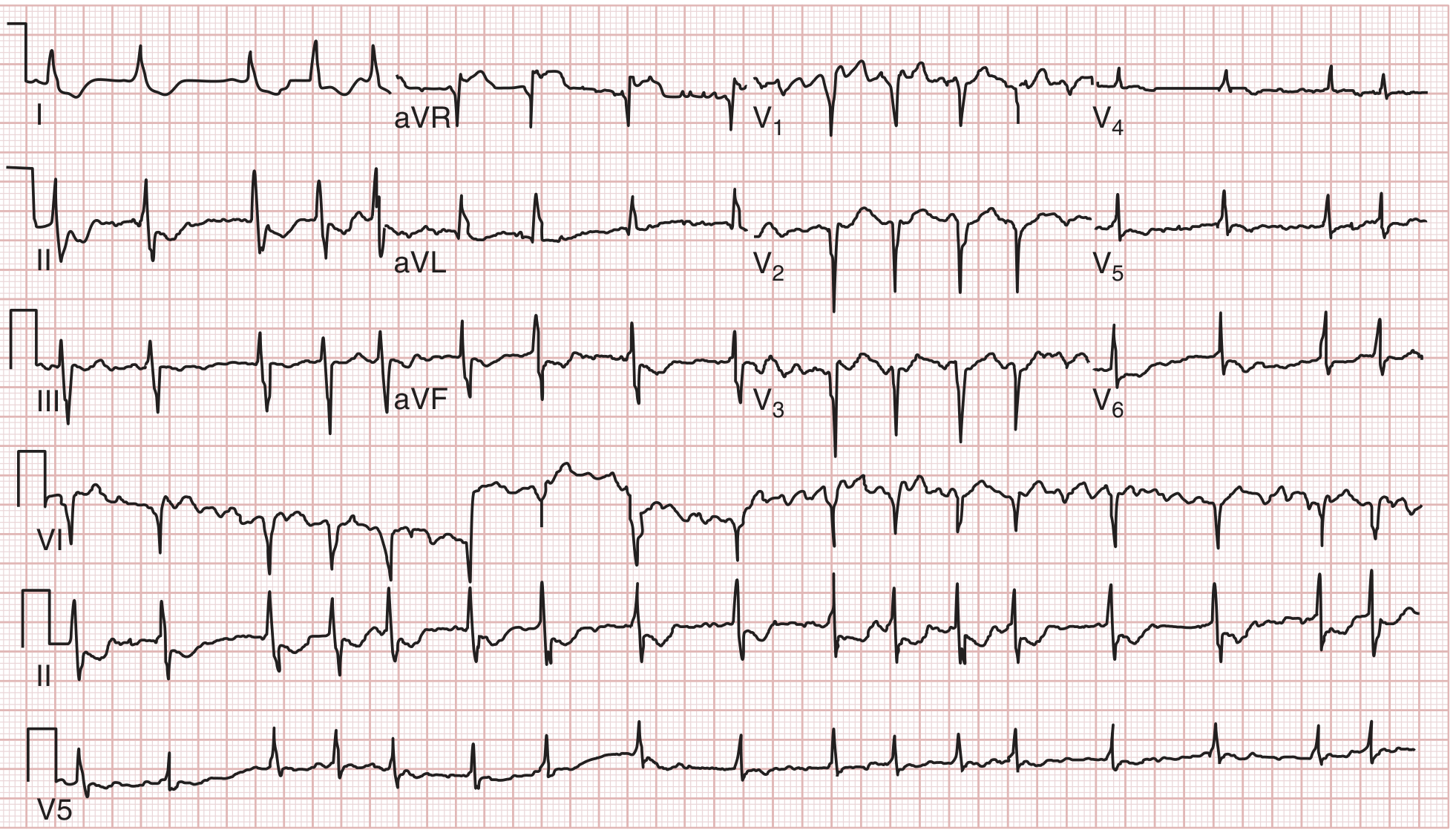
Fig: Inferior-lateral MI from left circumflex artery occlusion - ST elevation in II, III, aVF, and V2 with ST depression in V1-V3 (reciprocal). Inferior MIs can be complicated by AV block due to RCA/AV nodal artery compromise. - Tintinalli's Emergency Medicine
7. Wolff-Parkinson-White (WPW) Syndrome
Pathophysiology: An accessory pathway (Bundle of Kent) bypasses the AV node, pre-exciting part of the ventricle before the normal conduction system depolarizes the rest. This creates a characteristic ECG pattern.
ECG Changes:
- Short PR interval <120 ms (bypasses AV node delay)
- Delta wave - slurred, slow upstroke at the start of the QRS (initial pre-excitation of ventricle via accessory pathway)
- Wide QRS (>120 ms) due to fusion of accessory pathway and normal conduction
- Discordant ST-T changes - ST depression and T-wave inversions opposite to the delta wave direction
- WPW Type A (left-sided pathway): dominant R in V1, resembles RVH
- WPW Type B (right-sided pathway): negative delta/QRS in V1, resembles LBBB
- During AF with WPW: extremely rapid, irregular, wide-complex tachycardia >200 bpm - treat as an emergency (avoid AV nodal blockers like adenosine/verapamil)
Key point: The delta wave can mimic STEMI (pseudo-delta waves in certain leads) and can also mask true infarction.
8. Pulmonary Embolism (PE)
Pathophysiology: Massive PE causes acute right ventricular pressure overload and strain, producing distinctive but non-specific ECG changes.
ECG Changes:
- Sinus tachycardia - most common finding (found in ~40% of PE cases)
- S1Q3T3 pattern (McGinn-White sign): Deep S wave in lead I + Q wave in lead III + inverted T wave in lead III - classic but seen in only ~20%
- Right heart strain pattern: T-wave inversions in V1-V4 (anterior leads)
- Right bundle branch block (RBBB) - complete or incomplete - due to acute RV dilation
- Right axis deviation
- Atrial fibrillation or flutter
- Clockwise rotation of the heart (S waves in V5-V6)
- Note: ECG can be completely normal in up to 20% of PE cases
ECG Image - Anterior STEMI for comparison with PE (which can also show V1-V4 changes):
The pericarditis ECG above (diffuse ST elevation + PR depression) illustrates how PE-related ST changes can be confused with other diagnoses. Below is the anterolateral STEMI ECG for comparison with the V-lead changes seen in PE:
Note: In PE, the T-wave inversions are primarily in V1-V4 (right-sided strain), while anterior STEMI shows ST elevation in V1-V4. The key distinction: PE gives T inversions in V1-V4; STEMI gives ST elevation.
9. Dilated Cardiomyopathy / Congestive Heart Failure
Pathophysiology: Ventricular dilation and dysfunction alter conduction, causing diffuse myocardial changes on ECG.
ECG Changes:
- Left bundle branch block (LBBB) - very common (broad, notched QRS >120 ms; dominant negative in V1; dominant positive in V5-V6; no septal Q waves in I/V5-V6)
- Sinus tachycardia at rest (elevated sympathetic tone)
- Non-specific ST-T changes and T-wave flattening
- LVH voltage criteria (if hypertensive cardiomyopathy)
- Low-voltage QRS (<5 mm in limb leads, <10 mm in precordial leads) - suggests pericardial effusion or infiltrative disease (amyloid)
- Prolonged QRS/QTc - risk of ventricular arrhythmias and sudden death
- Atrial fibrillation is very common (20-30% of HF patients)
- Premature ventricular contractions (PVCs) - common
- First-degree AV block - PR >200 ms
ECG Image - Serial ACS/HF ECG Showing Evolution:
Fig: This ECG demonstrates how acute MI - a common cause of new-onset cardiomyopathy - shows evolving changes including ST deviation and left-sided involvement. Dilated cardiomyopathy may show LBBB, low voltage, or persistent ST-T changes from prior infarcts.
10. Atrial Flutter
Pathophysiology: A macro-reentrant circuit in the right atrium (usually around the tricuspid annulus) causes rapid, regular atrial depolarization at ~300 bpm, with AV conduction at a fixed ratio.
ECG Changes:
- Flutter waves ("F-waves") - classic "sawtooth" or "picket fence" pattern at ~300 bpm
- Most visible in leads II, III, aVF, and V1 (inferior leads are best)
- Regular atrial rate ~300 bpm (240-340 bpm)
- Fixed AV block ratio:
- 2:1 block - ventricular rate ~150 bpm (most common)
- 3:1 block - ventricular rate ~100 bpm
- 4:1 block - ventricular rate ~75 bpm
- Regular ventricular rhythm (unless variable block)
- Narrow QRS unless aberrant conduction
- Tip: At a ventricular rate of exactly 150 bpm, always suspect flutter with 2:1 block - flutter waves may be hidden in T waves
ECG Image - Atrial Flutter:
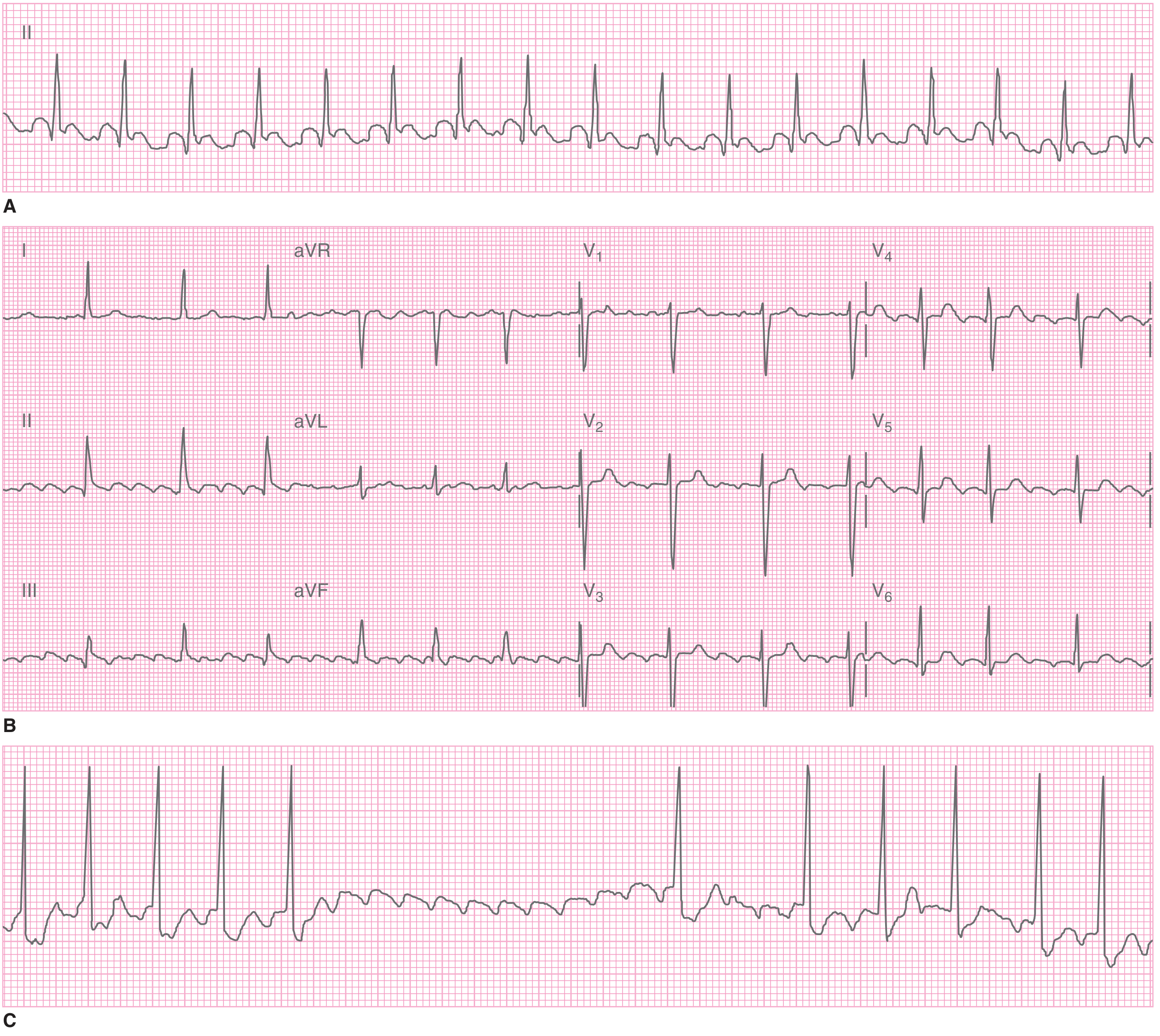
Fig: A. Regular narrow tachycardia at ~155 bpm. B. Full 12-lead showing classic sawtooth flutter waves in leads II, III, and aVF. C. Response to carotid sinus massage - transient AV block unmasks flutter waves clearly. - Tintinalli's Emergency Medicine
Quick Summary Table
| # | Condition | Key ECG Finding | Rate | Rhythm |
|---|---|---|---|---|
| 1 | STEMI | ST elevation in contiguous leads + Q waves | Normal-fast | Regular |
| 2 | NSTEMI/UA | ST depression, T-wave inversion | Normal | Regular |
| 3 | Atrial Fibrillation | No P waves, irregularly irregular | Variable | Irregular |
| 4 | Acute Pericarditis | Diffuse ST elevation + PR depression | Normal | Regular |
| 5 | LVH | High voltage + lateral strain | Normal | Regular |
| 6 | Complete Heart Block | AV dissociation, bradycardia | Slow escape | Regular (AV dissociated) |
| 7 | WPW Syndrome | Short PR + delta wave + wide QRS | Variable | Variable |
| 8 | Pulmonary Embolism | S1Q3T3, sinus tach, V1-V4 T inversions | Fast | Regular |
| 9 | Dilated CMP/CHF | LBBB, low voltage, AF, PVCs | Variable | Variable |
| 10 | Atrial Flutter | Sawtooth F-waves at ~300 bpm, 2:1 block | ~150 bpm | Regular |
Sources: Rosen's Emergency Medicine, Tintinalli's Emergency Medicine, Fuster and Hurst's The Heart (15th Ed.), Goldman-Cecil Medicine, Harrison's Principles of Internal Medicine 22E, LITFL ECG Library
This is a shared conversation. Sign in to Orris to start your own chat.