I have everything from Guyton & Hall directly. Now let me deliver the full teaching session.
PHYSIOLOGY MASTERCLASS - GUYTON & HALL
CHAPTER 1 & 2: THE CELL - Foundation of All Physiology
"You cannot understand any system in physiology unless you first understand its smallest living unit - the cell."
━━━━━━━━━━━━━━━━━━━━
STAGE 1: BIG PICTURE
━━━━━━━━━━━━━━━━━━━━
Why Does This Topic Exist?
Think of the human body like a country. Every country is made up of cities. Every city is made up of buildings. Every building is made up of bricks.
In the human body:
- Bricks = Cells
- Buildings = Tissues
- Cities = Organs
- Country = Organ Systems
The cell is the fundamental unit of life. Everything in physiology - every heartbeat, every breath, every thought - begins at the cellular level.
The human body contains 35-40 trillion cells (Guyton, Ch.1). Each one is a miniature factory, running 24/7, consuming fuel, making products, communicating with neighbors, and self-repairing.
Its Role in Homeostasis
The body's master goal is homeostasis - keeping the internal environment stable despite constant external change.
Who maintains homeostasis? Cells do. Every cell:
- Takes in O₂ and nutrients
- Releases CO₂ and waste
- Responds to signals (hormones, nerves)
- Adjusts its own function to maintain balance
If cells fail → homeostasis fails → disease occurs → death follows.
How It Connects to ALL Systems
Cell dysfunction
↓
Tissue fails (Histopathology)
↓
Organ fails (Pathology)
↓
System fails (Clinical Medicine)
↓
Body fails (Death)
| System | Cell Type | Specialized Function |
|---|
| Nervous | Neuron | Electrical signaling |
| Cardiac | Cardiomyocyte | Contraction |
| Blood | RBC | O₂ transport |
| Immunity | Lymphocyte | Defense |
| Kidney | Podocyte | Filtration |
| Liver | Hepatocyte | Metabolism |
| Gut | Enterocyte | Absorption |
Real-Life Importance
- Cancer = cell division gone wrong
- Diabetes = cell receptor failure (insulin resistance)
- Heart failure = cardiomyocyte death
- Alzheimer's = neuron degeneration
- Infection = pathogens attacking cells
Every disease in medicine is ultimately a cellular disease.
━━━━━━━━━━━━━━━━━━━━
STAGE 2: BASIC FOUNDATION
━━━━━━━━━━━━━━━━━━━━
Important Definitions
| Term | Definition |
|---|
| Cell | The smallest living unit capable of independent existence and performing all basic life functions |
| Protoplasm | All living material inside the cell (water + electrolytes + proteins + lipids + carbohydrates) |
| Organelle | Specialized structures within the cell with specific functions ("little organs") |
| Cytoplasm | Everything inside the cell membrane EXCEPT the nucleus |
| Nucleoplasm | Fluid inside the nucleus |
| Cell membrane | Also called plasma membrane - the boundary of the cell |
| Homeostasis | Maintenance of a stable internal environment |
Composition of Protoplasm (Guyton Ch.2)
| Component | % of cell mass | Key roles |
|---|
| Water | 70-85% | Universal solvent, medium for reactions |
| Proteins | 10-20% | Structure + enzymes + receptors |
| Lipids | ~2% | Membranes, energy storage |
| Carbohydrates | 1-3% (up to 6% in liver) | Energy currency, signaling |
| Electrolytes | Small % | Electrical gradients, enzyme cofactors |
High-yield fact: Fat cells (adipocytes) are the exception - triglycerides can make up 95% of their mass!
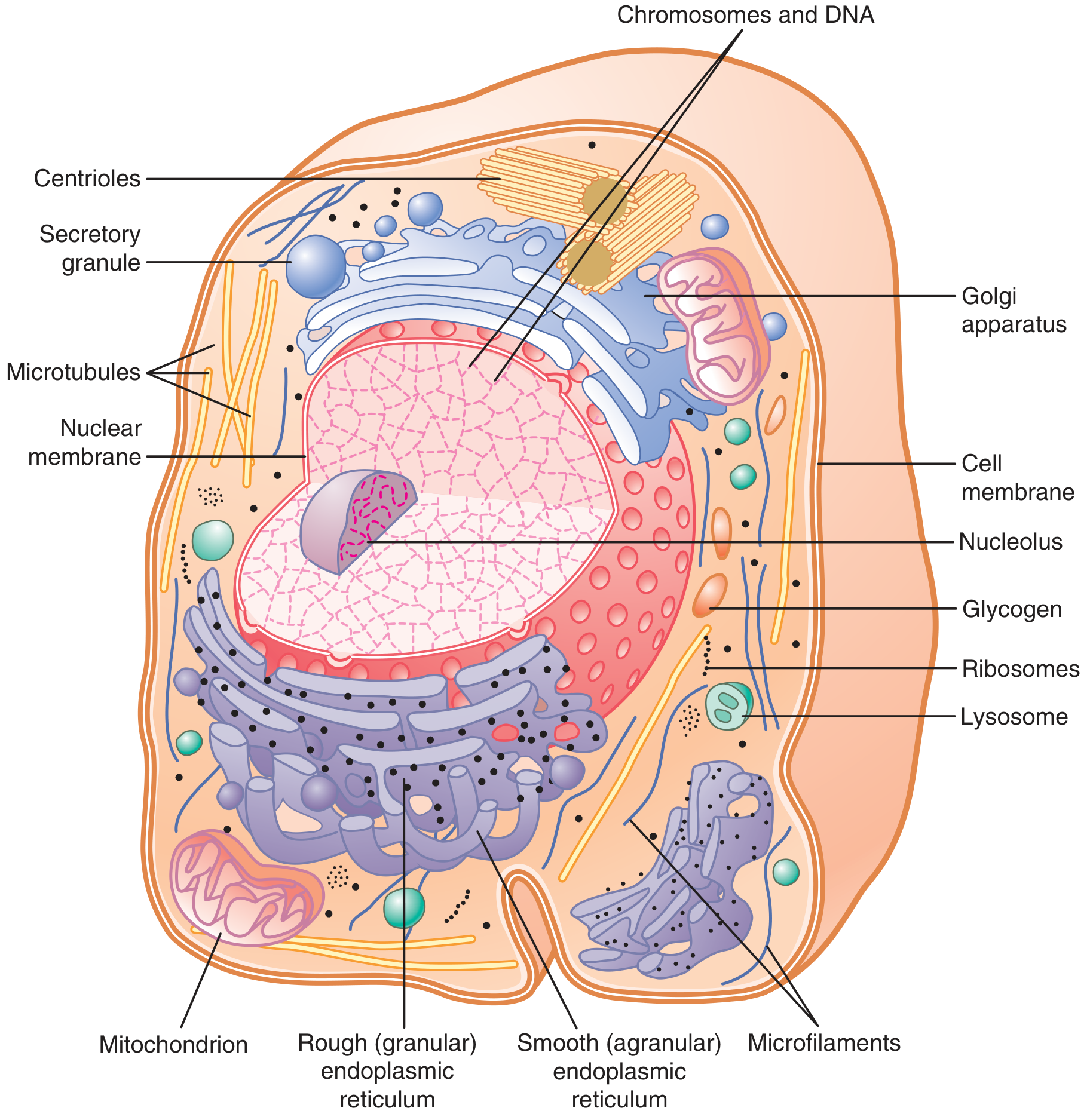
Anatomical Basis: Two Major Parts of the Cell
THE CELL
├── NUCLEUS (Command center)
│ ├── Nuclear membrane (double layer with pores)
│ ├── Nucleoplasm
│ ├── Chromosomes + DNA
│ └── Nucleolus (ribosome factory)
│
└── CYTOPLASM (Working floor)
├── Cell membrane (outer boundary)
├── Endoplasmic Reticulum (RER + SER)
├── Golgi Apparatus (post office)
├── Mitochondria (power plant)
├── Lysosomes (garbage disposal)
├── Peroxisomes (detox unit)
├── Ribosomes (protein factory)
├── Cytoskeleton (scaffolding)
└── Centrioles (cell division)
Here is the Guyton & Hall diagram of the cell (Fig. 2.2):
━━━━━━━━━━━━━━━━━━━━
STAGE 3: CORE PHYSIOLOGY - CELL MEMBRANE
━━━━━━━━━━━━━━━━━━━━
The Cell Membrane - The Most Important Structure in Physiology
What is it?
According to Guyton (Ch.2): A lipid bilayer with inserted proteins, 7.5-10 nm thick.
Composition (High-yield for exams!):
| Component | % |
|---|
| Proteins | 55% (majority!) |
| Phospholipids | 25% |
| Cholesterol | 13% |
| Other lipids | 4% |
| Carbohydrates | 3% |
Structure of the Lipid Bilayer - Explained Simply
Think of it like a sandwich:
- Two slices of bread = two layers of phospholipids
- The filling = the hydrophobic fatty acid tails
- Butter on outside = the hydrophilic phosphate heads
OUTSIDE OF CELL (water)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
⊙⊙⊙⊙⊙⊙⊙⊙⊙⊙⊙⊙ ← Phosphate heads (HYDROPHILIC)
|||||||||||||||||||||||||||||||| ← Fatty acid tails (HYDROPHOBIC)
|||||||||||||||||||||||||||||||| ← Fatty acid tails (HYDROPHOBIC)
⊙⊙⊙⊙⊙⊙⊙⊙⊙⊙⊙⊙ ← Phosphate heads (HYDROPHILIC)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
INSIDE OF CELL (water)
Why this arrangement?
- Phospholipids are amphipathic (amphis = both, pathos = feeling)
- They have both a water-loving head AND a fat-loving tail
- In water, the tails hide from water by facing each other inward
- This creates a self-assembling bilayer - no energy needed!
Fluid Mosaic Model
The membrane is not rigid - it is fluid. Proteins FLOAT in this lipid sea like icebergs in an ocean. This is the Fluid Mosaic Model (Singer & Nicolson, 1972).
Why fluid?
- Unsaturated fatty acids prevent tight packing
- Cholesterol regulates fluidity (prevents both extremes)
Membrane Proteins - The Workhorses
| Type | Location | Function |
|---|
| Integral proteins (Intrinsic) | Span entire membrane | Channels, pumps, receptors, transporters |
| Peripheral proteins (Extrinsic) | Attached to surface | Enzymes, structural support |
Functions of membrane proteins:
- Ion channels - Selective pores for Na⁺, K⁺, Ca²⁺, Cl⁻
- Carrier proteins (transporters) - Carry specific molecules across
- Pumps - Use energy (ATP) to move substances against gradient
- Receptors - Bind hormones, neurotransmitters
- Enzymes - Catalyze reactions at membrane surface
- Structural proteins - Connect to cytoskeleton
- Cell identity markers - Glycoproteins (ABO blood groups!)
━━━━━━━━━━━━━━━━━━━━
STAGE 3 CONTINUED: ORGANELLES - STEP BY STEP
━━━━━━━━━━━━━━━━━━━━
Each Organelle - What, Why, How, Clinical Link
1. MITOCHONDRIA - "The Powerhouse of the Cell"
What: Double membrane-bound organelle with its own DNA (maternal inheritance!)
Structure:
Outer membrane (smooth)
↓
Intermembrane space (H⁺ accumulates here)
↓
Inner membrane (highly folded = CRISTAE)
↓
Matrix (contains enzymes for Krebs cycle + mitochondrial DNA)
Why cristae? More folds = more surface area = more ATP synthase = more ATP production!
Function (step by step):
Glucose + O₂ enter cell
↓
Pyruvate enters mitochondria
↓
Krebs Cycle in matrix → NADH + FADH₂
↓
Electron Transport Chain on inner membrane
↓
H⁺ pumped into intermembrane space
↓
H⁺ flows back through ATP synthase
↓
ATP generated (36-38 ATP per glucose)
↓
CO₂ + H₂O as byproducts
Guyton Key Fact: Without mitochondria, >95% of ATP production stops immediately.
Clinical Links:
- Mitochondrial myopathy - Muscle weakness, lactic acidosis
- MELAS syndrome - Mitochondrial Encephalopathy, Lactic Acidosis, Stroke-like episodes
- Maternal inheritance - Mitochondrial diseases passed only through mother
- Cyanide poisoning - Blocks cytochrome c oxidase (Complex IV) → no ATP → rapid death
2. ENDOPLASMIC RETICULUM (ER)
Two types - remember with this mnemonic: "RER = Rough = Ribosomes = pRoteins; SER = Smooth = Steroids + detox"
| Feature | RER (Rough) | SER (Smooth) |
|---|
| Ribosomes | YES (gives rough look) | NO |
| Function | Protein synthesis + folding | Lipid/steroid synthesis, Ca²⁺ storage, detox |
| Abundance | Secretory cells (pancreas, liver) | Steroid cells (adrenal cortex, gonads), liver |
| Product | Proteins → Golgi | Lipids, steroids |
Clinical links:
- Liver SER - Cytochrome P450 enzymes detoxify drugs here
- Drug interactions - Enzyme inducers (rifampicin, phenytoin) → upregulate SER → faster drug metabolism
- ER stress - Unfolded Protein Response (UPR) - when too many misfolded proteins accumulate → cell death → diabetes, neurodegeneration
3. GOLGI APPARATUS - "The Post Office / Processing Plant"
Simple analogy: Amazon warehouse. Products (proteins) arrive from ER → get labeled (glycosylated) → sorted → shipped to final destination.
Flow:
Proteins arrive from RER (in transport vesicles)
↓
Enter Cis-Golgi (receiving side - faces ER)
↓
Trans-Golgi (shipping side - faces cell membrane)
↓
Proteins get:
- Glycosylation (sugar tags added)
- Phosphorylation
- Sulfation
↓
Sorted into vesicles → sent to:
- Lysosomes
- Secretory granules (exocytosis)
- Cell membrane
Clinical link:
- I-cell disease (Mucolipidosis II) - Phosphorylation of lysosomal enzymes fails → enzymes secreted outside cell instead of going to lysosomes → lysosomal storage disease
4. LYSOSOMES - "The Garbage Disposal / Suicide Bag"
What: Membrane-bound vesicles containing 40+ hydrolytic enzymes (acid hydrolases)
pH inside: 4.5-5.0 (acidic - required for enzyme activity)
Maintained by: H⁺-ATPase pump on lysosomal membrane
Functions:
- Digest material from phagocytosis (bacteria, dead cells)
- Digest material from pinocytosis
- Autophagy (cell eats its own old organelles)
- Apoptosis (programmed cell death) - "suicide bag" concept
Lysosomal Storage Diseases - Critical for exams:
| Disease | Enzyme Deficient | Substance Accumulated | Features |
|---|
| Gaucher's | Glucocerebrosidase | Glucocerebroside | Bone pain, splenomegaly |
| Niemann-Pick | Sphingomyelinase | Sphingomyelin | Neurodegeneration, cherry-red spot |
| Tay-Sachs | Hex-A | GM2 ganglioside | Neurodegeneration, cherry-red spot (Ashkenazi Jews) |
| Hurler's | α-L-iduronidase | Heparan + dermatan sulfate | Gargoylism, corneal clouding |
| Pompe's | Acid maltase | Glycogen | Cardiomegaly, hypotonia |
Memory trick for Gaucher's: Gaucher's = Glucose storage = liver, spleen, Gone wrong (bone marrow)
5. PEROXISOMES
What: Small membrane-bound organelles containing oxidases and catalase
Function:
Fatty acids (very long chain) enter peroxisome
↓
β-oxidation → H₂O₂ (toxic!) produced
↓
Catalase breaks down H₂O₂ → H₂O + O₂
↓
Detoxified!
Also: Bile acid synthesis, plasmalogen synthesis, oxidation of amino acids
Clinical link:
- Zellweger syndrome - Absent peroxisomes → very long chain fatty acid accumulation → severe neurodegeneration + death in infancy
6. RIBOSOMES - "The Protein Factory"
Composition:
- Made of rRNA + proteins
- Two subunits: 60S (large) + 40S (small) = 80S (in eukaryotes)
- Bacteria have 50S + 30S = 70S (this difference is exploited by antibiotics!)
Types:
| Type | Location | Makes |
|---|
| Free ribosomes | Float in cytoplasm | Intracellular proteins |
| Bound ribosomes | On RER surface | Secretory proteins, membrane proteins |
Why this matters clinically:
| Antibiotic | Subunit blocked | Mechanism |
|---|
| Aminoglycosides (gentamicin) | 30S | Misreads mRNA → nonsense proteins |
| Tetracyclines | 30S | Blocks tRNA entry |
| Macrolides (erythromycin) | 50S | Blocks translocation |
| Chloramphenicol | 50S | Blocks peptidyl transferase |
| Linezolid | 50S | Blocks 70S initiation complex |
Key concept: Antibiotics work because bacterial ribosomes are 70S, while our cells have 80S ribosomes - so antibiotics are selectively toxic to bacteria!
7. NUCLEUS - "The Command Center"
Structure:
Nuclear Envelope (double membrane)
↓
Nuclear Pores (~3,000-4,000 per nucleus)
- Allow passage of RNA out, proteins in
↓
Nucleoplasm
↓
Chromatin = DNA + histone proteins
- Euchromatin = active (transcribing)
- Heterochromatin = inactive (condensed)
↓
Nucleolus (1-2 per nucleus)
- Site of rRNA synthesis
- Makes ribosome subunits
- DISAPPEARS during cell division (high-yield!)
Key numbers:
- Human cell: 46 chromosomes (23 pairs)
- ~3 billion base pairs of DNA
- DNA fully stretched: ~2 meters long (but coiled into 6 µm nucleus!)
8. CYTOSKELETON - "The Internal Scaffolding"
Three components:
| Component | Composition | Size | Function |
|---|
| Microfilaments | Actin | 7 nm | Cell shape, muscle contraction, movement |
| Intermediate filaments | Keratin, vimentin, desmin | 10 nm | Mechanical strength, anchoring |
| Microtubules | Tubulin (α+β) | 25 nm | Cell division (spindle), transport, cilia |
Clinical links:
- Colchicine - Inhibits tubulin polymerization → disrupts mitotic spindle → treats gout (also stops neutrophil migration!)
- Taxol (paclitaxel) - Prevents microtubule depolymerization → cell cannot complete division → cancer drug
- Kartagener syndrome - Dynein arm defect in cilia → immotile cilia → bronchiectasis + situs inversus + male infertility
━━━━━━━━━━━━━━━━━━━━
STAGE 4: MOLECULAR & CELLULAR PHYSIOLOGY
━━━━━━━━━━━━━━━━━━━━
Transport Across Cell Membrane
This is one of the most tested topics in all of physiology. Master this completely.
Two Categories:
MEMBRANE TRANSPORT
│
├── PASSIVE (No ATP needed - goes with gradient)
│ ├── Simple diffusion
│ ├── Facilitated diffusion (needs carrier/channel)
│ └── Osmosis (water movement)
│
└── ACTIVE (ATP needed - goes against gradient)
├── Primary active transport (directly uses ATP)
└── Secondary active transport (uses gradient created by primary)
1. SIMPLE DIFFUSION
What: Movement of substances from high concentration → low concentration through the lipid bilayer directly.
Which substances can cross directly?
- Must be: small + nonpolar + lipid-soluble
- Examples: O₂, CO₂, N₂, steroid hormones, alcohol, fatty acids, urea (small)
Fick's Law of Diffusion:
Rate of diffusion ∝ (Concentration gradient × Surface area × Diffusion coefficient) / Membrane thickness
Rate of diffusion ∝ ΔC × A × D
─────────────
d
Where:
- ΔC = concentration difference
- A = surface area
- D = diffusion coefficient (related to lipid solubility)
- d = membrane thickness
Clinical application:
- Emphysema - Alveolar wall destruction → decreased surface area (A↓) → decreased O₂ diffusion → hypoxia
- Pulmonary fibrosis - Thickened alveolar membrane (d↑) → decreased diffusion → hypoxia
2. FACILITATED DIFFUSION
What: Passive transport using protein carriers or channels. Still goes DOWN the concentration gradient. No ATP needed.
Two types of proteins used:
| Feature | Channel Proteins | Carrier Proteins |
|---|
| Mechanism | Open pore - substances flow through | Bind substance, change shape, release on other side |
| Speed | Very fast (millions of ions/sec) | Slower (thousands/sec) |
| Selectivity | Highly selective (by size + charge) | Highly selective (specific binding site) |
| Examples | Na⁺, K⁺, Ca²⁺, Cl⁻ channels | GLUT transporters, amino acid carriers |
Types of Channels:
- Leak channels - Always open (resting K⁺ channels → resting membrane potential)
- Voltage-gated - Open/close based on membrane potential (Na⁺ channels in action potential)
- Ligand-gated - Open when a specific molecule binds (nicotinic ACh receptor at NMJ)
- Mechanically-gated - Open when physically stretched (hearing hair cells)
3. OSMOSIS
What: Movement of WATER across a semipermeable membrane from low solute → high solute concentration (or equivalently, high water → low water concentration).
Key concept: Osmolarity vs Tonicity
| Term | Definition | Clinical use |
|---|
| Osmolarity | Total solute concentration (mOsm/L) | Measured in lab |
| Tonicity | Effect of solution on cell volume (only non-penetrating solutes count) | Clinical IV fluids |
Normal plasma osmolarity = 285-295 mOsm/L
Formula:
Plasma Osmolarity = 2[Na⁺] + Glucose/18 + BUN/2.8
= 2 × 140 + 90/18 + 14/2.8
≈ 290 mOsm/L
IV Fluid Osmolarity (High-yield):
| Solution | Osmolarity | Tonicity | Effect on RBC |
|---|
| 0.9% NaCl (Normal Saline) | 308 mOsm/L | Isotonic | No change |
| 0.45% NaCl (Half Normal Saline) | 154 mOsm/L | Hypotonic | Cell swells (lysis risk) |
| 3% NaCl (Hypertonic saline) | ~1026 mOsm/L | Hypertonic | Cell shrinks (crenation) |
| 5% Dextrose (D5W) | 278 mOsm/L | Initially isotonic, then hypotonic (glucose metabolized) | Swells |
4. PRIMARY ACTIVE TRANSPORT - The Na⁺/K⁺-ATPase Pump
The most important pump in the human body.
What it does:
Uses 1 ATP to move:
3 Na⁺ OUT of cell
2 K⁺ INTO cell
(Against concentration gradients for both)
Why 3 out, 2 in?
- Creates net outward movement of positive charge
- Makes inside of cell slightly negative → resting membrane potential (~-70mV in neurons)
What it maintains:
- [Na⁺] inside cell: ~12 mEq/L (low)
- [Na⁺] outside cell: ~142 mEq/L (high)
- [K⁺] inside cell: ~150 mEq/L (high)
- [K⁺] outside cell: ~4 mEq/L (low)
Regulation:
- Increased by: Intracellular Na⁺↑, aldosterone (increases pump expression in kidney), thyroid hormone
- Inhibited by: Digoxin/cardiac glycosides (clinically important!)
Clinical application:
- Digoxin - Inhibits Na⁺/K⁺-ATPase → [Na⁺]i rises → Na⁺/Ca²⁺ exchanger (NCX) works less → [Ca²⁺]i rises → stronger cardiac contraction (positive inotropy)
- Hypokalemia - Low K⁺ → pump dysfunction → muscle weakness, arrhythmias
- Ouabain - Cardiotoxic plant compound, same mechanism as digoxin (used experimentally)
5. SECONDARY ACTIVE TRANSPORT
Concept: The Na⁺ gradient created by the Na⁺/K⁺-ATPase pump is stored energy. This stored energy can be used to transport other substances.
Two types:
Cotransport (Symport) - same direction:
Na⁺ (high outside → low inside) carries glucose IN together
→ Na⁺-glucose cotransporter (SGLT) in gut and kidney
Countertransport (Antiport) - opposite directions:
Na⁺ comes IN while H⁺ goes OUT
→ Na⁺/H⁺ exchanger in kidney proximal tubule
Key example - SGLT2 Inhibitors:
- Dapagliflozin, Empagliflozin, Canagliflozin
- Block SGLT2 in kidney → glucose cannot be reabsorbed → glucosuria → lower blood glucose
- Used in Type 2 Diabetes, Heart Failure, CKD
- Adverse effects: Urinary tract infections, Fournier's gangrene (rare but deadly)
━━━━━━━━━━━━━━━━━━━━
STAGE 5: INTEGRATED PHYSIOLOGY
━━━━━━━━━━━━━━━━━━━━
How Cell Membrane Physiology Links to Every System:
| System | Connection to Cell Membrane |
|---|
| Nervous | Action potential requires Na⁺ channels + K⁺ channels + Na⁺/K⁺-ATPase |
| Muscle | Excitation-contraction coupling via voltage-gated Ca²⁺ channels |
| Kidney | SGLT, Na⁺/K⁺-ATPase drive water and solute reabsorption |
| GIT | Na⁺-glucose cotransport in enterocytes drives glucose absorption |
| Endocrine | Hormone receptors on cell membrane or nuclear receptors inside cell |
| Cardiac | Funny channels (If), L-type Ca²⁺ channels drive pacemaker activity |
| Immune | Membrane receptors (TCR, BCR) recognize antigens |
━━━━━━━━━━━━━━━━━━━━
STAGE 7 & 8: CLINICAL PHYSIOLOGY + PATHOPHYSIOLOGY
━━━━━━━━━━━━━━━━━━━━
Classic Clinical Scenarios Based on Cell Physiology:
Scenario 1: Cyanide Poisoning
Normal: O₂ → Electron Transport Chain → ATP production
↓ CYANIDE BLOCKS Complex IV (cytochrome c oxidase)
No ATP produced
↓
Na⁺/K⁺-ATPase fails (needs ATP)
↓
Na⁺ floods into cells → cells swell
K⁺ leaks out → hyperkalemia
↓
Neurons and cardiac cells die (most sensitive - highest ATP demand)
↓
Signs: Altered consciousness, seizures, cardiac arrest
↓
Treatment: Hydroxocobalamin (binds CN⁻) or sodium thiosulfate
Scenario 2: Hypoxic Cell Injury (Universal Mechanism of Disease)
Ischemia / Hypoxia
↓
Mitochondrial oxidative phosphorylation fails
↓
ATP depletes
↓
Na⁺/K⁺-ATPase pump fails
↓
Na⁺ enters cell → H₂O follows → Cell SWELLS (hydropic change)
K⁺ exits cell
Ca²⁺ enters cell (massive influx)
↓
Cellular enzymes activated by Ca²⁺:
- Phospholipases → membrane damage
- Proteases → cytoskeletal damage
- Endonucleases → DNA damage
↓
Mitochondrial permeability transition pore opens
↓
CELL DEATH (Necrosis)
This is the mechanism of: Myocardial infarction, Stroke, AKI, Liver failure from any cause.
━━━━━━━━━━━━━━━━━━━━
STAGE 9: PHARMACOLOGICAL CORRELATIONS
━━━━━━━━━━━━━━━━━━━━
Drugs Targeting Cell Membrane and Organelles:
| Drug | Target | Mechanism | Use |
|---|
| Digoxin | Na⁺/K⁺-ATPase | Inhibits pump → ↑ intracellular Ca²⁺ | Heart failure, AF |
| Colchicine | Microtubules | Inhibits tubulin polymerization | Gout, pericarditis |
| Taxol | Microtubules | Prevents depolymerization | Cancer |
| Vinca alkaloids | Microtubules | Inhibits polymerization | Cancer |
| Furosemide | NKCC2 cotransporter | Blocks Na⁺-K⁺-2Cl⁻ cotransport | Edema, HTN |
| SGLT2 inhibitors | Na⁺-glucose transporter | Blocks glucose reabsorption | T2DM, HF, CKD |
| Metformin | Mitochondrial Complex I | Reduces hepatic glucose production | T2DM |
| Statins | HMG-CoA reductase (in SER) | Reduce cholesterol synthesis | Hyperlipidemia |
| Chloroquine | Lysosomes | Raises lysosomal pH (disrupts function) | Malaria, RA |
| Aminoglycosides | 30S ribosome | Misreading of mRNA | Gram-negative infections |
| Macrolides | 50S ribosome | Blocks translocation | Atypical pneumonia |
━━━━━━━━━━━━━━━━━━━━
STAGE 11: IMPORTANT TABLES
━━━━━━━━━━━━━━━━━━━━
Intracellular vs Extracellular Fluid Composition (MASTER TABLE)
| Ion/Substance | Intracellular | Extracellular | Clinical Relevance |
|---|
| Na⁺ | 12 mEq/L | 142 mEq/L | Hypernatremia → brain shrinkage |
| K⁺ | 150 mEq/L | 4 mEq/L | Hyperkalemia → arrhythmias |
| Ca²⁺ (free) | 0.0001 mEq/L | 2.4 mEq/L | Hypocalcemia → tetany |
| Cl⁻ | 4 mEq/L | 103 mEq/L | Hypochloremia → metabolic alkalosis |
| HCO₃⁻ | 10 mEq/L | 28 mEq/L | Acid-base balance |
| Protein | 40 g/dL | 2 g/dL | Oncotic pressure |
| Glucose | Low (used rapidly) | 90 mg/dL | Hyperglycemia → osmotic diuresis |
| pH | ~7.0 | 7.4 | Acidosis/Alkalosis |
━━━━━━━━━━━━━━━━━━━━
STAGE 12: NUMERICAL VALUES (High-yield)
━━━━━━━━━━━━━━━━━━━━
| Value | Number | Unit |
|---|
| Total cells in human body | 35-40 trillion | cells |
| Cell membrane thickness | 7.5-10 | nm |
| Protein content of cell membrane | 55% | - |
| Phospholipid content | 25% | - |
| Water content of cells | 70-85% | % cell mass |
| Protein content of cells | 10-20% | % cell mass |
| Resting membrane potential | -70 to -90 | mV |
| Normal plasma osmolarity | 285-295 | mOsm/L |
| Normal serum Na⁺ | 135-145 | mEq/L |
| Normal serum K⁺ | 3.5-5.0 | mEq/L |
| Normal serum Ca²⁺ | 8.5-10.5 | mg/dL |
| Normal blood glucose (fasting) | 70-100 | mg/dL |
| pH of lysosomes | 4.5-5.0 | - |
| Eukaryotic ribosome size | 80S (60S + 40S) | - |
| Prokaryotic ribosome size | 70S (50S + 30S) | - |
| Na⁺ pumped out per ATP cycle | 3 | ions |
| K⁺ pumped in per ATP cycle | 2 | ions |
━━━━━━━━━━━━━━━━━━━━
STAGE 13: VIVA PREPARATION
━━━━━━━━━━━━━━━━━━━━
Short Viva Questions:
- What is the composition of the cell membrane?
- What is the fluid mosaic model?
- What is the difference between integral and peripheral proteins?
- Name 4 functions of membrane proteins.
- What does the Na⁺/K⁺-ATPase pump do?
- Why does cyanide kill cells?
- What is the difference between osmolarity and tonicity?
- Why is the inside of cells negative?
- What is the pH of lysosomes and why?
- Why are ribosomes good antibiotic targets?
Examiner's Favorite Questions:
- "Explain the Na⁺/K⁺-ATPase pump and its clinical importance." - Always comes in exams. Cover structure → function → Digoxin mechanism.
- "What is the mechanism of hypoxic cell injury?" - Universal pathology question.
- "Why can lipid-soluble drugs cross the blood-brain barrier?" - Fluid mosaic + membrane permeability.
- "How do SGLT2 inhibitors work?" - Secondary active transport concept.
━━━━━━━━━━━━━━━━━━━━
STAGE 15: MEMORY TOOLS
━━━━━━━━━━━━━━━━━━━━
Mnemonics:
Cell membrane composition: "Pretty Pleased Can't Love Chemistry"
- Proteins 55%
- Phospholipids 25%
- Cholesterol 13%
- Lipids (other) 4%
- Carbohydrates 3%
Lysosomal storage diseases: "Go Nibble Those Hurting Puppies"
- Gaucher's (glucocerebrosidase)
- Niemann-Pick (sphingomyelinase)
- Tay-Sachs (Hex-A)
- Hurler's (iduronidase)
- Pompe's (acid maltase)
Na⁺/K⁺-ATPase: "3 Na out, 2 K in" = 3-2 = like 32 (easy to remember!)
Transport types: "PFSOA"
- Passive diffusion (lipid soluble)
- Facilitated diffusion (channel/carrier)
- Secondary active transport
- Osmosis (water)
- Active (primary, Na⁺/K⁺-ATPase)
Antibiotic ribosome targets:
- "30S: TAGS" - Tetracyclines, Aminoglycosides
- "50S: CHIME" - Chloramphenicol, clindamycin, macrolides (erythromycin), linezolid
━━━━━━━━━━━━━━━━━━━━
STAGE 16: FLOWCHART SUMMARY
━━━━━━━━━━━━━━━━━━━━
THE CELL - MASTER FLOWCHART
━━━━━━━━━━━━━━━━━━━━━━━━━━━━
CELL MEMBRANE (lipid bilayer + proteins)
│
├─ TRANSPORT ─────────────────────────────────┐
│ ├─ Passive: O₂, CO₂, steroids │
│ ├─ Facilitated: glucose (GLUT), ions │
│ ├─ Active Primary: Na⁺/K⁺-ATPase │
│ └─ Active Secondary: SGLT, Na⁺/H⁺ │
│ │
├─ SIGNALING │
│ └─ Receptors → second messengers │
│ (cAMP, IP3, DAG, Ca²⁺) │
│ │
NUCLEUS (DNA → RNA → Protein) │
│ │
├─ Transcription (DNA → mRNA) │
└─ mRNA → Ribosomes │
│ │
├─ Free ribosome → cytoplasmic │
│ proteins │
└─ RER ribosome → secretory │
proteins → Golgi ─────────────→─┘
│
┌────────┴────────┐
↓ ↓
Secretory Lysosome
vesicles (pH 4.5-5)
(exocytosis) (digestion)
MITOCHONDRIA (ATP factory)
│
└─ Krebs cycle + ETC → 36-38 ATP/glucose
If blocked (CN⁻, hypoxia) → cell death
━━━━━━━━━━━━━━━━━━━━
STAGE 17: COMMON MISTAKES & TRAPS
━━━━━━━━━━━━━━━━━━━━
Common Misconceptions:
-
"Osmolarity and Tonicity are the same" - WRONG!
- Osmolarity = total solutes
- Tonicity = only non-penetrating solutes (determines cell volume change)
- Urea contributes to osmolarity but NOT tonicity (it crosses freely)
-
"Facilitated diffusion needs ATP" - WRONG! It is passive (uses concentration gradient, NOT ATP)
-
"The Na⁺/K⁺-ATPase pump always pumps equal amounts in both directions" - WRONG! It pumps 3 Na⁺ out, 2 K⁺ in (electrogenic - creates charge difference)
-
"All membrane proteins are channels" - WRONG! Most membrane proteins are receptors and enzymes, not channels.
-
"Diffusion is only possible in liquids" - WRONG! Diffusion occurs in gases, liquids, and across membranes.
-
"Large cells have more ATP per cell" - The key is surface area to volume ratio. Larger cells have relatively less membrane surface for O₂ entry.
-
"Lysosomal diseases only affect one organ" - WRONG! Lysosomes are in every cell - diseases are multi-systemic.
-
"Digoxin increases heart rate" - WRONG! Digoxin actually slows heart rate (via vagal stimulation) while increasing contractility.
━━━━━━━━━━━━━━━━━━━━
STAGE 18: RAPID REVISION
━━━━━━━━━━━━━━━━━━━━
20 KEY TAKEAWAYS:
- Human body has 35-40 trillion cells; gut microbiota outnumbers human cells
- Cell membrane = lipid bilayer (7.5-10 nm); composition: 55% protein, 25% phospholipid, 13% cholesterol
- Phospholipids are amphipathic - hydrophilic heads outside, hydrophobic tails inside
- Fluid mosaic model - proteins float in fluid lipid bilayer
- Membrane proteins function as: channels, carriers, pumps, receptors, enzymes, identity markers
- Na⁺/K⁺-ATPase: 3 Na⁺ out, 2 K⁺ in, uses 1 ATP - creates resting membrane potential
- Simple diffusion: small, lipid-soluble, nonpolar substances only
- Facilitated diffusion: no ATP, down gradient, uses channels or carriers
- Osmosis: water moves toward higher solute concentration
- Normal plasma osmolarity: 285-295 mOsm/L
- SGLT2 inhibitors exploit secondary active transport to treat diabetes
- Mitochondria generate >95% of cellular ATP via ETC; have own DNA (maternal inheritance)
- RER = protein synthesis; SER = lipid/steroid synthesis + detox (CYP450)
- Golgi = post office - glycosylation, sorting, secretion of proteins
- Lysosomes = acid pH (4.5-5.0); contain 40+ hydrolases; "suicide bag"
- Eukaryote ribosomes = 80S; Prokaryote = 70S - basis of antibiotic selectivity
- Microtubules (tubulin): targeted by colchicine (inhibits) and taxol (stabilizes)
- Cyanide kills by blocking Complex IV → no ATP → Na⁺/K⁺-ATPase fails → cell death
- Hypoxic injury: ATP depletion → pump failure → Ca²⁺ overload → cell death (universal mechanism)
- Lysosomal storage diseases result from enzyme deficiency → substrate accumulation → multi-system disease
━━━━━━━━━━━━━━━━━━━━
STAGE 19: CLINICAL CASES
━━━━━━━━━━━━━━━━━━━━
CASE 1 (Basic):
A 3-year-old child is brought with developmental delay, hepatosplenomegaly, and bilateral cherry-red spots on fundoscopy. The child's parents are both of Ashkenazi Jewish descent.
Questions:
- What is the diagnosis?
- What enzyme is deficient?
- What substance accumulates?
- Which organelle is abnormal?
- Why does the cherry-red spot appear?
CASE 2 (Intermediate):
A 65-year-old man with heart failure is started on digoxin. Two weeks later he presents with nausea, vomiting, blurred vision with yellow halos, and heart rate of 44/min.
Questions:
- What is happening?
- What is the mechanism of digoxin's therapeutic effect?
- What is the mechanism of its toxicity here?
- How does hypokalemia worsen digoxin toxicity?
- What is the treatment?
CASE 3 (Advanced):
A 55-year-old male smoker is admitted with acute MI. EKG shows ST elevation in leads II, III, aVF. Troponin is elevated.
Questions:
- At the cellular level, what is happening in the cardiomyocytes of the infarcted zone right now?
- Explain the sequence from ischemia to irreversible cell death step by step.
- Why does troponin leak into the blood?
- Why does the infarcted area eventually show "coagulative necrosis" on histology?
- What is reperfusion injury, and what cellular mechanism causes it?
━━━━━━━━━━━━━━━━━━━━
STAGE 20: ACTIVE RECALL - MCQs
━━━━━━━━━━━━━━━━━━━━
Q1. The cell membrane is primarily composed of which substance?
- A) Carbohydrates
- B) Proteins
- C) Phospholipids
- D) Cholesterol
(Answer: B - Proteins make up 55% - the largest single component)
Q2. The Na⁺/K⁺-ATPase pump moves:
- A) 2 Na⁺ out, 3 K⁺ in
- B) 3 Na⁺ out, 2 K⁺ in
- C) 3 Na⁺ in, 2 K⁺ out
- D) Equal amounts of both
(Answer: B - "3 out, 2 in" - creates electronegativity inside)
Q3. A drug that inhibits microtubule polymerization would MOST affect which process?
- A) Protein synthesis
- B) ATP production
- C) Cell division
- D) Membrane transport
(Answer: C - Microtubules form the mitotic spindle)
Q4. Which of the following can cross the cell membrane by simple diffusion?
- A) Glucose
- B) Na⁺ ions
- C) Oxygen
- D) Amino acids
(Answer: C - O₂ is small, nonpolar, lipid-soluble)
Q5. A 2-year-old with hypotonia, cardiomegaly, and glycogen accumulation in all tissues most likely has a deficiency of:
- A) Glucocerebrosidase
- B) Sphingomyelinase
- C) Acid maltase
- D) Hexosaminidase A
(Answer: C - Pompe disease = acid maltase (α-1,4-glucosidase) deficiency)
Q6. Assertion-Reason:
-
Assertion: Digoxin toxicity is worsened by hypokalemia
-
Reason: Digoxin and K⁺ compete for the same binding site on Na⁺/K⁺-ATPase
-
A) Both A and R true, R explains A
-
B) Both true, R does not explain A
-
C) A true, R false
-
D) Both false
(Answer: A - Low K⁺ means more digoxin binds to the pump → increased toxicity)
Q7. True/False:
- Urea contributes to tonicity - FALSE (urea is a penetrating solute - doesn't affect cell volume)
- The lysosomal pH is maintained by an H⁺-ATPase pump - TRUE
- Ribosomes disappear from the nucleolus during mitosis - FALSE (the NUCLEOLUS disappears during mitosis)
- SER is most abundant in steroid-secreting cells - TRUE
- Cyanide primarily affects neurons and heart because they have the highest ATP demand - TRUE
What's Next?
You've now mastered Chapter 1-2 of Guyton & Hall - the cell, its structure, membrane transport, and clinical applications. This is the foundation everything else builds on.
Coming next: We go to Chapter 3 - Genetic Control of Protein Synthesis, Cell Function, and Cell Reproduction (DNA → RNA → Protein, Cell Division, Cancer at the cellular level), followed by Chapter 4 - Transport of Substances Through Cell Membranes (deep dive into specific transport systems).
Reply with:
- ✅ "Continue" to go to Chapter 3
- ✅ "More cases" for more clinical cases on this chapter
- ✅ "Test me" for a full 20-question MCQ quiz on Chapter 1-2
- ✅ "Deep dive [topic]" to go deeper into any specific section (e.g., "Deep dive Na/K ATPase pump")