Cardiac arrest sonographic assessment as emergency physician
Reading File
Finding Sources
Finding Sources
Searching PubMed
"cardiac arrest" AND "point-of-care ultrasound" AND "emergency"
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading Article
PMID: 41610792
Reading File
Reading Article
PMID: 39930527
Reading Article
PMID: 41274023
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching the Web
POCUS cardiac arrest SHoC protocol emergency physician 2024 2025 guidelines
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC10887671
Loading Image
Loading Image
I now have comprehensive information from Rosen's Emergency Medicine, Miller's Anesthesia, the SHoC protocol, and three recent systematic reviews/meta-analyses. Here is a thorough, clinically organized answer:
POCUS in Cardiac Arrest: Emergency Physician's Guide
Overview
Point-of-care ultrasound (POCUS) during cardiac arrest serves three core roles: identifying reversible causes, assessing cardiac activity and prognosis, and monitoring CPR quality and guiding advanced interventions. All major resuscitation bodies (AHA, ERC, ACEP, ASE) endorse POCUS in arrest with the cardinal rule that it must never cause CPR interruptions beyond 10 seconds.
- Rosen's Emergency Medicine, p. 3622
- Miller's Anesthesia 10e, p. 5033
The Golden Rule: CPR Integration
POCUS must be performed during the rhythm/pulse check pause, not before it. Image acquisition should occur within the 10-second window; interpretation and extracardiac scanning resume once chest compressions restart. A dedicated timekeeper is recommended. Some protocols require a second operator to avoid the sonographer delaying compression restarts.
Preferred Views During Arrest
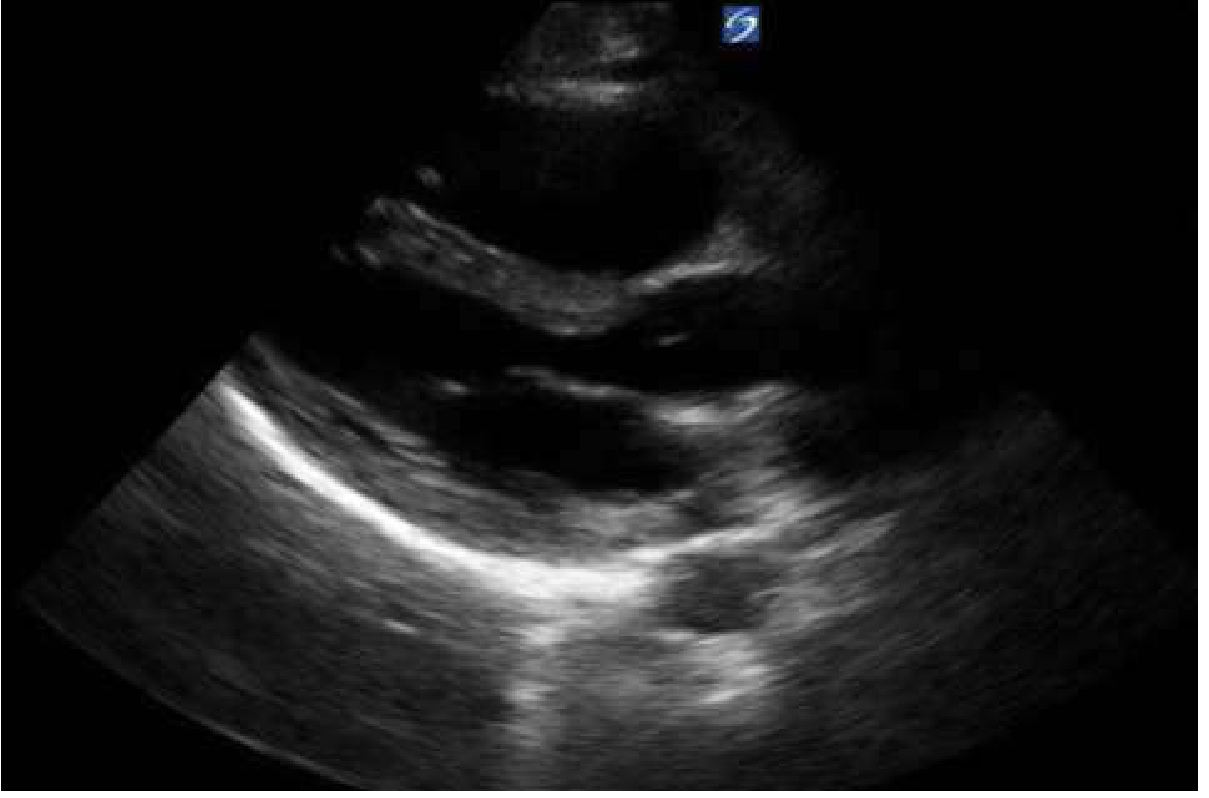
1. Subcostal (Subxiphoid) Four-Chamber View - PRIMARY VIEW
The go-to view in arrest. It:
- Does not interfere with chest compressions
- Allows assessment of pericardial fluid, RV/LV size and function
- Is identical to the FAST cardiac window

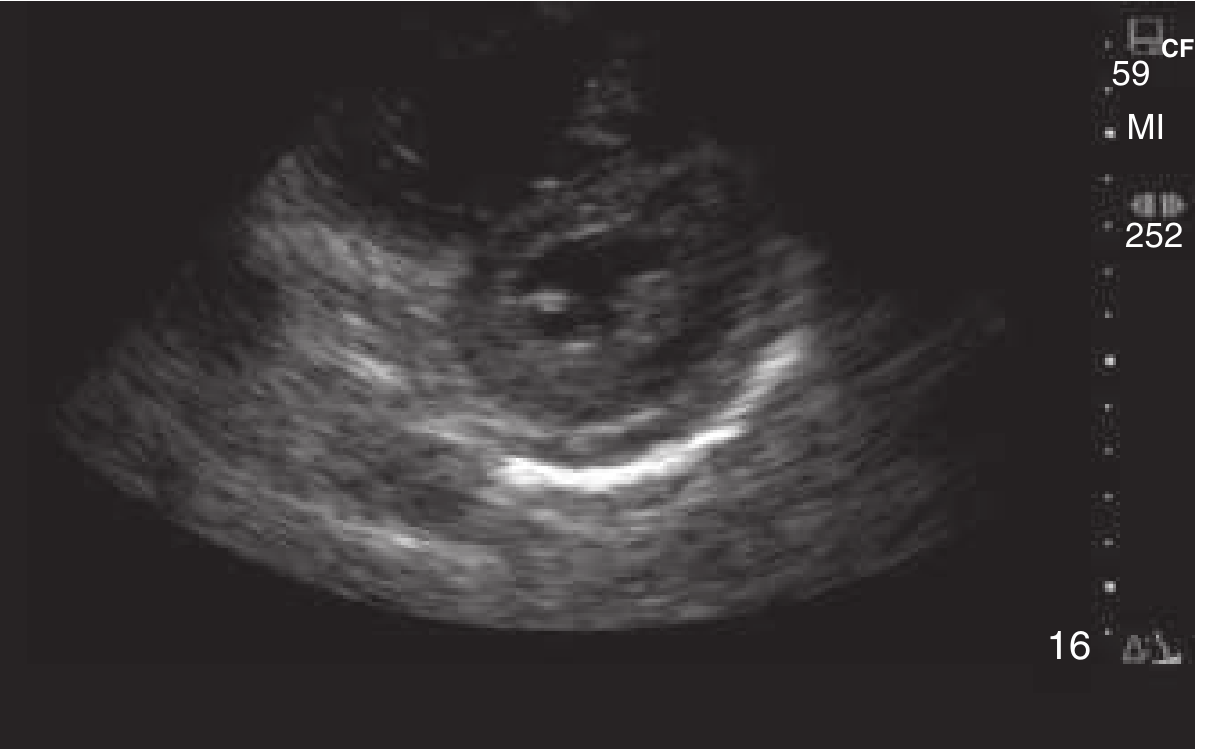
2. Parasternal Long-Axis (PLAX) - FALLBACK
Used when subcostal window is poor. Best for LV function, pericardial effusion, and valve assessment.
3. Supplemental Views (after compressions resume)
- Lung views (bilateral): absent lung sliding = tension pneumothorax
- IVC view: collapsibility index for volume status (filling assessment)
- Abdominal (in trauma): free fluid
The SHoC Protocol: The Four "Fs"
The Sonography in Hypotension and Cardiac Arrest (SHoC) protocol from the International Federation for Emergency Medicine (IFEM) structures the exam as:
| F | What to Assess | Clinical Question |
|---|---|---|
| Fluid (pericardial) | Anechoic rim around heart | Tamponade? |
| Form | RV:LV ratio, septal shift | PE, RV strain? |
| Function | Wall motion, contractility | True vs pseudo-PEA? Cardiac standstill? |
| Filling (IVC) | IVC diameter + collapse | Hypovolemia? |
Core views (Fluid, Form, Function) are mandatory during the pulse check pause. Filling and lung views are supplemental.
Diagnostic Applications: Identifying Reversible Causes (The Hs and Ts)
POCUS directly visualizes several of the ACLS "Hs and Ts":
Cardiac Tamponade
- Findings: Anechoic fluid in pericardial space, diastolic RV collapse, plethoric (non-collapsible) IVC
- Pericardial effusions as small as 50 mL can cause tamponade in the acute setting
- If found, proceed to pericardiocentesis under ultrasound guidance
- Rosen's Emergency Medicine, p. 3623
Pulmonary Embolism (Massive)
- Findings: Dilated RV (RV:LV ratio >0.9 in A4C), McConnell's sign (RV free wall akinesis with preserved apex), "D" sign on parasternal short axis (septal flattening from elevated RV pressure), thrombus in right heart
- McConnell's sign is highly suggestive of PE but also seen in RV infarction
Tension Pneumothorax
- Findings: Absent lung sliding (M-mode: "barcode" / "stratosphere" sign instead of "seashore" sign); lung point pathognomonic if found
- More sensitive than supine CXR, approaching CT sensitivity
- Rosen's Emergency Medicine, p. 3623
Hypovolemia
- Findings: Small, hyperdynamic LV ("kissing walls"), flat/collapsible IVC (<1 cm diameter)
- Guides empiric fluid resuscitation
Aortic Dissection / AAA Rupture
- Aortic dissection: linear echogenic intimal flap in the aorta or pericardial effusion + dilated aortic root (>4 cm)
- AAA: aortic diameter >3 cm (risk of rupture higher >4.5 cm), free peritoneal fluid in rupture
- Sensitivity 80-90%, specificity ~100% for dissection but should not be used to exclude it
Prognostic / Functional Assessment
True PEA vs Pseudo-PEA
One of the most actionable distinctions in arrest:
- True PEA (cardiac standstill): No wall motion visible - universally poor prognosis
- Pseudo-PEA: Organized cardiac motion present despite no palpable pulse - patient may respond to aggressive resuscitation, treat as profound shock
Cardiac Standstill and ROSC Prediction
A 2026 systematic review and meta-analysis (24 studies, 3,684 patients) found:
- Sensitivity of cardiac standstill for predicting absence of ROSC: 85.6% (95% CI 0.789-0.904)
- Specificity: 79.0% (95% CI 0.671-0.874)
- Diagnostic odds ratio: 22.6 (95% CI 12.45-41.0)
- AUC: 0.871 - indicating good diagnostic accuracy
- Breglia et al., J Emerg Med 2026 [PMID: 41610792]
PEA with Cardiac Activity - Prognosis
In PEA patients, the presence of any cardiac activity on POCUS predicts better outcomes (2025 meta-analysis, 18 studies, 1,202 patients):
- ROSC prediction: sensitivity 0.86, specificity 0.64
- Survival to admission: sensitivity 0.89, specificity 0.73 (best AUC: 0.89)
- POCUS cardiac activity is useful as part of a multimodal approach to termination of resuscitation decisions
- Jian et al., Scand J Trauma Resusc Emerg Med 2025 [PMID: 39930527]
Important Caveat
Cardiac standstill alone should not be the sole reason to terminate resuscitation - it must be interpreted in clinical context (rhythm, ETCO2, duration of arrest, reversible causes present/treated).
Pulse Check: POCUS vs Manual Palpation
A 2026 systematic review (6 studies) compared POCUS of great arteries to manual carotid/femoral pulse palpation:
- POCUS had higher accuracy in all three studies reporting accuracy
- POCUS was faster in all five studies reporting speed
- Manual pulse palpation is known to be unreliable even by experienced providers
- Ko et al., J Emerg Med 2026 [PMID: 41274023]
Doppler ultrasound of the femoral artery can also be used during CPR to confirm adequacy of compressions generating cardiac output.
CPR Quality Monitoring
POCUS (especially TEE if available) can assess:
- Adequate depth and rate of compressions (real-time LV compression)
- Mitral valve opening during release = adequate decompression
- Coronary perfusion pressure correlates (aortic relaxation pressure)
- TEE is increasingly preferred in periarrest settings as it avoids interrupting chest compressions entirely
- Miller's Anesthesia 10e, p. 5033
Transesophageal Echocardiography (TEE) in Arrest
TEE offers:
- Continuous real-time imaging without interrupting CPR
- Superior image quality vs TTE in arrest (no chest wall obstruction)
- Direct LV compression assessment
- Identification of all reversible causes
- Especially useful when TTE windows are poor
ACLS guidelines note TEE may be "even more useful" in the periarrest patient to minimize non-CPR intervals. Rosen's Emergency Medicine, p. 3622
Practical Algorithm Summary
CARDIAC ARREST
|
▼
Rhythm/Pulse Check Pause (≤10 sec)
|
├── Subcostal 4-chamber (preferred) or PLAX
| ├── Pericardial fluid? → Tamponade → Pericardiocentesis
| ├── RV dilation + McConnell's → PE → Lytics / ECPR
| ├── Cardiac standstill? → Poor prognosis (multimodal)
| └── Organized activity? → Pseudo-PEA → Aggressive Rx
|
▼
Resume compressions → interpret + plan supplemental views
|
├── Lung US: absent sliding → Tension PTX → Needle decompression
├── IVC: collapsed → Hypovolemia → Fluids
└── Aorta: aneurysm/dissection, free fluid (trauma)
Key Points Summary
- Timing is non-negotiable: POCUS during CPR must fit within the ≤10-second pulse check pause; all four major resuscitation guidelines require this
- Subcostal view first - does not interfere with compressions; fallback to PLAX if inadequate
- The SHoC Four Fs: Fluid (tamponade), Form (PE/RV strain), Function (standstill vs activity), Filling (IVC/volume)
- Cardiac standstill predicts failure to achieve ROSC with sensitivity ~86%, specificity ~79% (2026 meta-analysis, n=3684); do not use in isolation to terminate resuscitation
- Pseudo-PEA (organized activity despite no pulse) is actionable - treat as shock, not arrest
- POCUS pulse check is faster and more accurate than manual palpation (2026 systematic review)
- TEE avoids compression interruptions entirely and should be considered when available
- Do not use POCUS to exclude aortic dissection or PE - sensitivity insufficient for rule-out
- Reversible causes directly visualized: tamponade, massive PE, tension PTX, hypovolemia, aortic catastrophe
Sources: Rosen's Emergency Medicine (9e), p. 3617-3623; Miller's Anesthesia 10e, p. 5033; SHoC Protocol (IFEM USIG); Breglia et al. J Emerg Med 2026 [PMID 41610792]; Jian et al. Scand J Trauma Resusc Emerg Med 2025 [PMID 39930527]; Ko et al. J Emerg Med 2026 [PMID 41274023]
This is a shared conversation. Sign in to Orris to start your own chat.