Signs of raised intracranial pressure
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the full answer.
Signs of Raised Intracranial Pressure (ICP)
Normal ICP is 5-15 mmHg. When it rises, it compromises cerebral perfusion pressure (CPP = MAP - ICP) and ultimately causes brainstem herniation if uncorrected.
Pathophysiological Basis: The Monro-Kellie Doctrine
The skull is a rigid box. Any increase in volume (blood, brain, CSF, or mass) must be compensated by displacement of another component. Once compensation is exhausted, ICP rises exponentially.
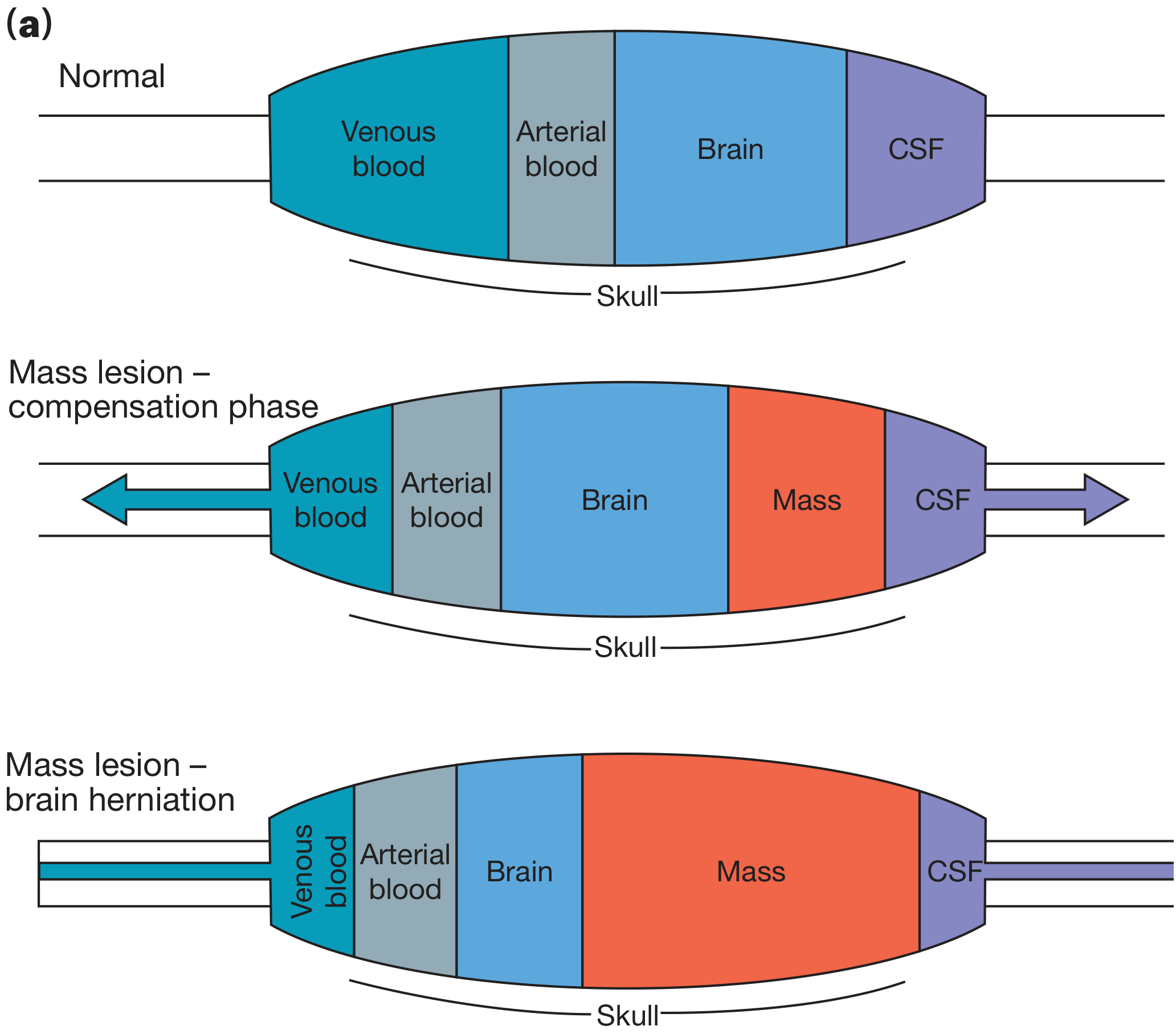
Fig. Monro-Kellie doctrine: During the compensation phase, venous blood and CSF are displaced. Once exhausted, ICP rises steeply and herniation occurs - Bailey & Love's Surgery, p. 382.
Clinical Signs and Symptoms
Early / General Signs
| Feature | Details |
|---|---|
| Headache | Classic early symptom - worse in the morning (lying flat increases ICP), aggravated by coughing, straining, or Valsalva. Described as progressive and diffuse. |
| Nausea and vomiting | Often projectile; due to compression of vomiting centres in the medulla. Vomiting may occur without nausea. |
| Papilledema | Swelling of the optic disc due to raised pressure transmitted along the optic nerve sheath. Takes 12-24 hours to develop after acute events; its absence does NOT exclude raised ICP, especially in the elderly. |
| Visual disturbances | Transient visual obscurations (brief episodes of bilateral visual blurring on postural change); enlarged blind spot; reduced visual acuity if chronic. |
| Altered consciousness | Progressive: from drowsiness/lethargy → confusion → stupor → coma. |
Eye Signs
| Sign | Mechanism |
|---|---|
| Papilledema | Most reliable objective sign; optic disc swelling with blurred margins and engorged veins on fundoscopy. |
| Sixth nerve (abducens) palsy | Lateral rectus weakness causing diplopia - a "false localizing sign" due to stretching of CN VI over the petrous ridge; unilateral or bilateral. |
| Third nerve (CN III) palsy | Late sign indicating uncal herniation compressing CN III; produces ipsilateral fixed dilated pupil ("blown pupil") with ptosis and down-and-out gaze. |
| Subhyaloid (preretinal) hemorrhages | Terson syndrome - seen with subarachnoid hemorrhage; hemorrhage beneath the internal limiting membrane of the retina. |
Late / Herniation Signs
Cushing's Triad (a pre-terminal sign of impending brainstem herniation):
- Hypertension (widened pulse pressure)
- Bradycardia
- Irregular respiration (Cheyne-Stokes, apneustic, or ataxic breathing)
This triad results from cerebellar tonsillar herniation through the foramen magnum compressing the medullary vasomotor and respiratory centres. The patient at this stage is said to be "coning."
Herniation Syndromes
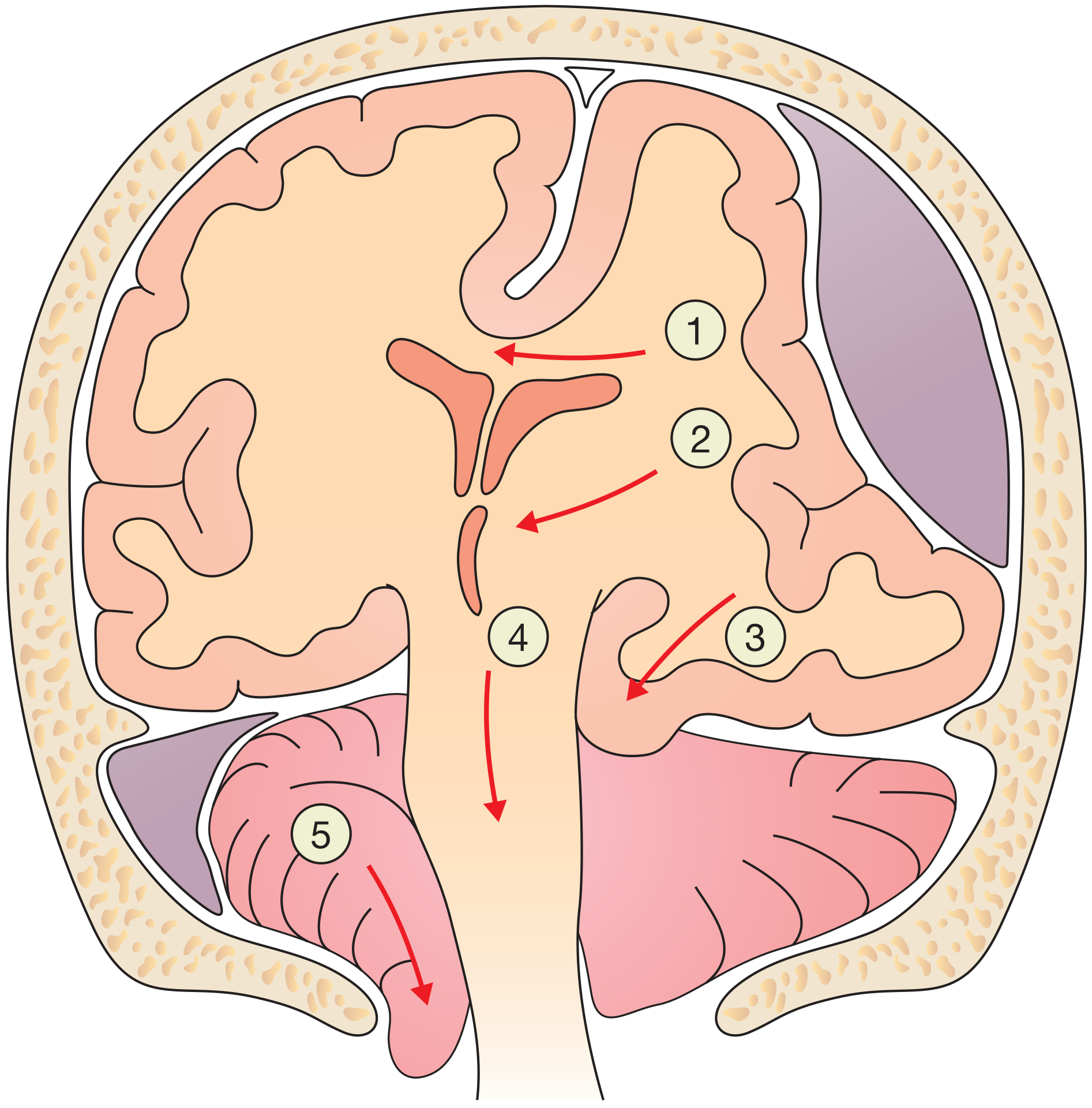
Fig. Herniation syndromes: (1) Subfalcine - cingulate herniates under falx; (2) Midline shift; (3) Uncal - temporal lobe over tentorium, compresses CN III; (4) Central herniation; (5) Tonsillar herniation through foramen magnum causing Cushing's triad - Bailey & Love's Surgery, p. 382.
| Herniation type | Key sign |
|---|---|
| Uncal (transtentorial) | Ipsilateral fixed dilated pupil (CN III compression), then contralateral hemiparesis |
| Central | Bilateral small reactive pupils → bilateral motor posturing (decorticate then decerebrate) |
| Tonsillar (foramen magnum) | Cushing's triad, sudden apnoea, cardiac arrest |
| Subfalcine | Leg weakness (ACA territory compression) |
Signs in Children / Infants
- Bulging fontanelle (in infants with open fontanelles)
- Sunset sign (downward conjugate gaze deviation due to pressure on the tectal plate)
- Cracked-pot sign (Macewen's sign) - percussion of the skull produces a hollow note due to spread sutures
- Rapid head circumference increase
- Prominent scalp veins
Summary: Early vs. Late Signs
| Stage | Signs |
|---|---|
| Early | Morning headache, nausea/vomiting, papilledema, visual obscurations, CN VI palsy |
| Intermediate | Declining GCS, CN III palsy (blown pupil), hemiparesis, Babinski sign |
| Late (herniation) | Cushing's triad (hypertension + bradycardia + irregular breathing), decorticate/decerebrate posturing, fixed dilated pupils, coma |
Key point: Papilledema + CN VI palsy + morning headache with vomiting is the classic triad of raised ICP from a space-occupying lesion (e.g. brain tumour). However, papilledema may be absent in acute rises (e.g. extradural haematoma) and in the elderly. Cushing's triad is a pre-terminal event and warrants immediate intervention.
Sources: Adams & Victor's Principles of Neurology 12e, p. 390 | Bailey & Love's Short Practice of Surgery 28e, pp. 381-382 | Harrison's Principles of Internal Medicine 22e | Plum & Posner's Diagnosis and Treatment of Stupor and Coma
This is a shared conversation. Sign in to Orris to start your own chat.