Schizophrenia common clinical Manifestations
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Here is a comprehensive overview of the common clinical manifestations of schizophrenia, drawn from Harrison's, Goldman-Cecil Medicine, Adams & Victor's Neurology, Stahl's Essential Psychopharmacology, and Kandel's Principles of Neural Science.
Schizophrenia: Clinical Manifestations
Schizophrenia is a heterogeneous syndrome characterized by perturbations of language, perception, thinking, social activity, affect, and volition. There are no pathognomonic features. Onset typically occurs in late adolescence to young adulthood (slightly earlier in males), and the course is often chronic with poor functional outcomes.
The DSM-5 requires at least two characteristic symptoms present for a 1-month period, with continuous signs for at least 6 months.
Symptom Domains
Modern psychiatry organizes schizophrenic symptoms into five dimensions (Stahl's Essential Psychopharmacology):
- Positive symptoms
- Negative symptoms
- Cognitive symptoms
- Affective symptoms
- Aggressive symptoms
1. Positive Symptoms
(Additions to normal experience — respond well to antipsychotics)
| Symptom | Description |
|---|---|
| Hallucinations | Most commonly auditory (voices commenting on the patient or conversing with each other); visual, olfactory, and tactile hallucinations also occur |
| Delusions | Fixed false beliefs — persecutory (most common), referential, grandiose, somatic, or bizarre |
| Disorganized thinking / speech | Loosening of associations, tangentiality, derailment, neologisms (invented words), clanging (sound-based word associations), thought blocking |
| Grossly disorganized behavior | Unpredictable agitation, inappropriate affect, disheveled appearance, social disinhibition |
| Catatonia | A spectrum including stupor, mutism, waxy flexibility (catalepsy), stereotypy, echolalia, echopraxia, posturing |
Thought disorder example (Kandel's Principles of Neural Science): "I don't think they care for me because two million camels . . . 10 million taxis . . . Father Christmas on the rebound."
2. Negative Symptoms
(Diminution of normal functions — associated with poor long-term prognosis and poor drug response)
Negative symptoms predominate in one-third of the schizophrenic population.
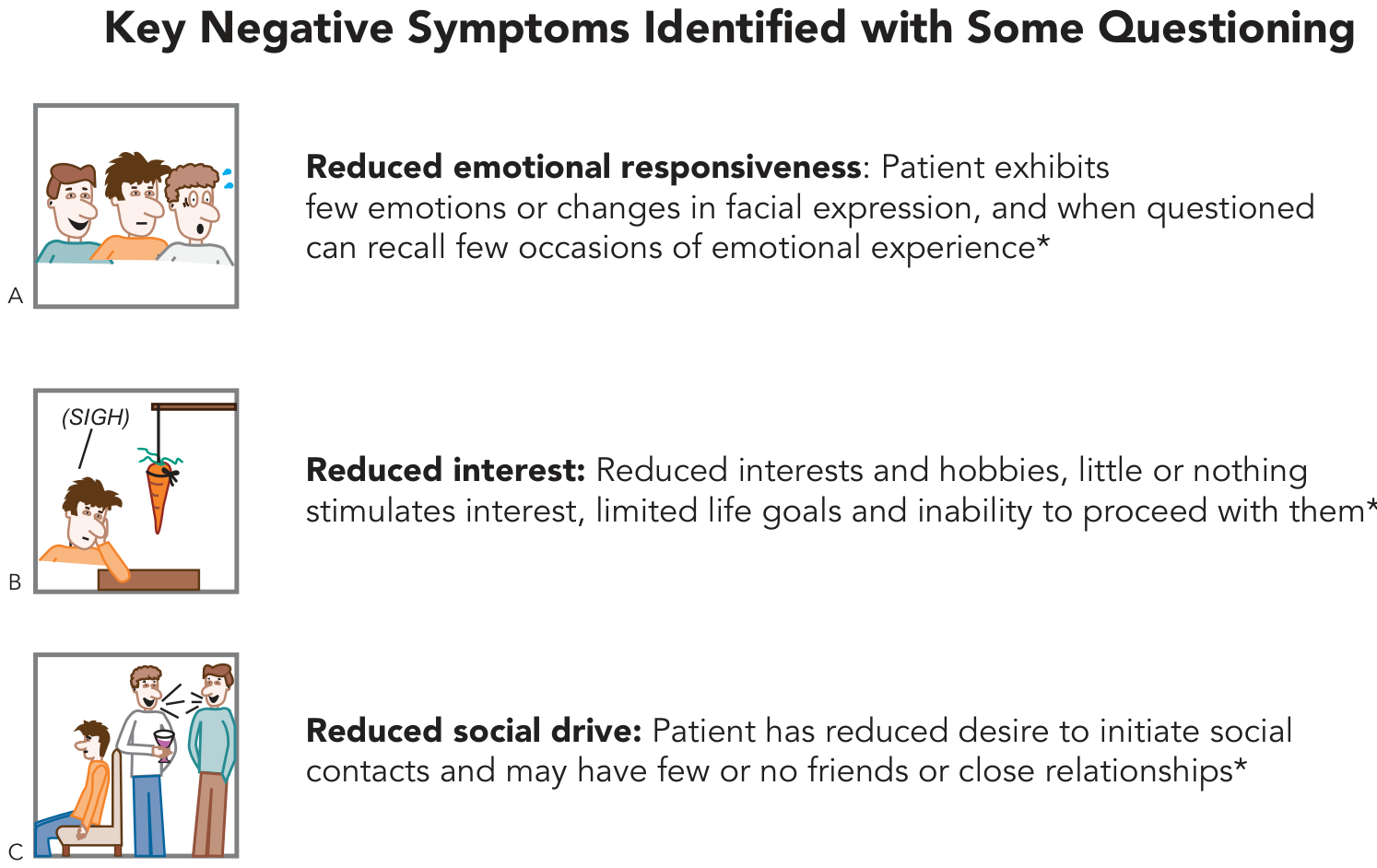
| Symptom | Description |
|---|---|
| Affective flattening (blunted affect) | Reduced facial expression, monotone voice, limited eye contact, diminished emotional responsiveness |
| Alogia | Poverty of speech and impoverished thought content |
| Avolition / Abulia | Lack of motivation; inability to initiate or sustain goal-directed activity |
| Anhedonia | Inability to experience pleasure; reduced interest in hobbies or life goals |
| Asociality | Social withdrawal; few or no close relationships |
3. Cognitive Symptoms
(Often the earliest to appear; do not respond to antipsychotics)
Cognitive deficits begin before the first psychotic episode and progress throughout the illness. They emphasize executive dysfunction, not the memory loss typical of dementia.
Key cognitive impairments (Stahl's / Kandel's):
- Impaired working memory and executive function
- Problems representing and maintaining goals
- Difficulty focusing, sustaining, and allocating attention
- Impaired verbal fluency (spontaneous speech generation)
- Deficits in serial learning (lists, sequences)
- Impaired social cognition (reading emotions from faces)
- Problems monitoring performance and problem-solving
4. Affective Symptoms
Patients frequently experience depression, suicidality, and anxiety comorbidly. Approximately 10% of schizophrenic patients commit suicide (Harrison's 22e). Dysphoria and hopelessness are common, especially during partial remissions.
5. Aggressive Symptoms
Hostility and aggression can occur, particularly during acute psychotic episodes. These may be directed at others or at the self.
Temporal Pattern of Onset
| Phase | Features |
|---|---|
| Premorbid | Subtle social awkwardness, lower IQ than expected for family |
| Prodromal | Social withdrawal, odd beliefs, perceptual distortions, declining function |
| Acute (psychotic) episodes | Florid positive symptoms (hallucinations, delusions, disorganized behavior) |
| Residual phase | Predominance of negative and cognitive symptoms; positive symptoms attenuate with age |
Diagnostic Criteria Snapshot (DSM-5)
- ≥2 of: delusions, hallucinations, disorganized speech, grossly disorganized/catatonic behavior, negative symptoms
- Duration: active symptoms ≥1 month; continuous signs ≥6 months
- Significant social/occupational dysfunction
- Exclusion of mood disorders, substances, and medical causes
Related Diagnostic Spectrum
| Disorder | Duration |
|---|---|
| Brief psychotic disorder | < 1 month |
| Schizophreniform disorder | 1–6 months |
| Schizophrenia | ≥ 6 months |
| Schizoaffective disorder | Schizophrenic + independent mood episodes |
| Delusional disorder | Delusions only, ≥1 month, otherwise normal functioning |
Sources: Harrison's Principles of Internal Medicine 22e — Goldman-Cecil Medicine — Adams & Victor's Principles of Neurology 12e — Stahl's Essential Psychopharmacology — Kandel's Principles of Neural Science 6e
This is a shared conversation. Sign in to Orris to start your own chat.