Features of tuberculosis in eye
Reading File
Finding Sources
Finding Sources
Searching PubMed
ocular tuberculosis clinical features
Reading File
Searching Images
ocular tuberculosis uveitis choroidal tubercle
Searching PubMed
ocular tuberculosis uveitis
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive content from Kanski's Clinical Ophthalmology and clinical images. Here is a complete, organized answer.
Ocular Tuberculosis — Clinical Features
Mycobacterium tuberculosis reaches the eye haematogenously from a primary pulmonary focus. Importantly, ocular involvement commonly occurs without clinically overt systemic disease, so the absence of active pulmonary TB does not exclude the diagnosis. Immune deficiency (including HIV) is a key risk factor, and atypical mycobacteria (e.g., M. avium) may cause disease in immunocompromised patients.
1. Anterior Segment
| Feature | Details |
|---|---|
| Anterior uveitis | Most common; typically granulomatous with mutton-fat keratic precipitates (KPs) |
| Iris nodules | Koeppe (pupil margin) and Busacca (iris stroma) nodules |
| Posterior synechiae | Broad-based PS can form |
| Phlyctenulosis | Hypersensitivity reaction at limbus; nodular lesion with surrounding injection |
| Interstitial keratitis | Stromal corneal inflammation |
| Scleritis | Granulomatous nodular or diffuse |
| Conjunctivitis | Rare; phlyctenular conjunctivitis more typical |
2. Posterior Segment (Most Distinctive Features)
a. Choroidal Granuloma (Tubercle/Tuberculoma)
Focal, elevated dome-shaped yellow-white lesions — may be unilateral or bilateral, solitary or multiple.
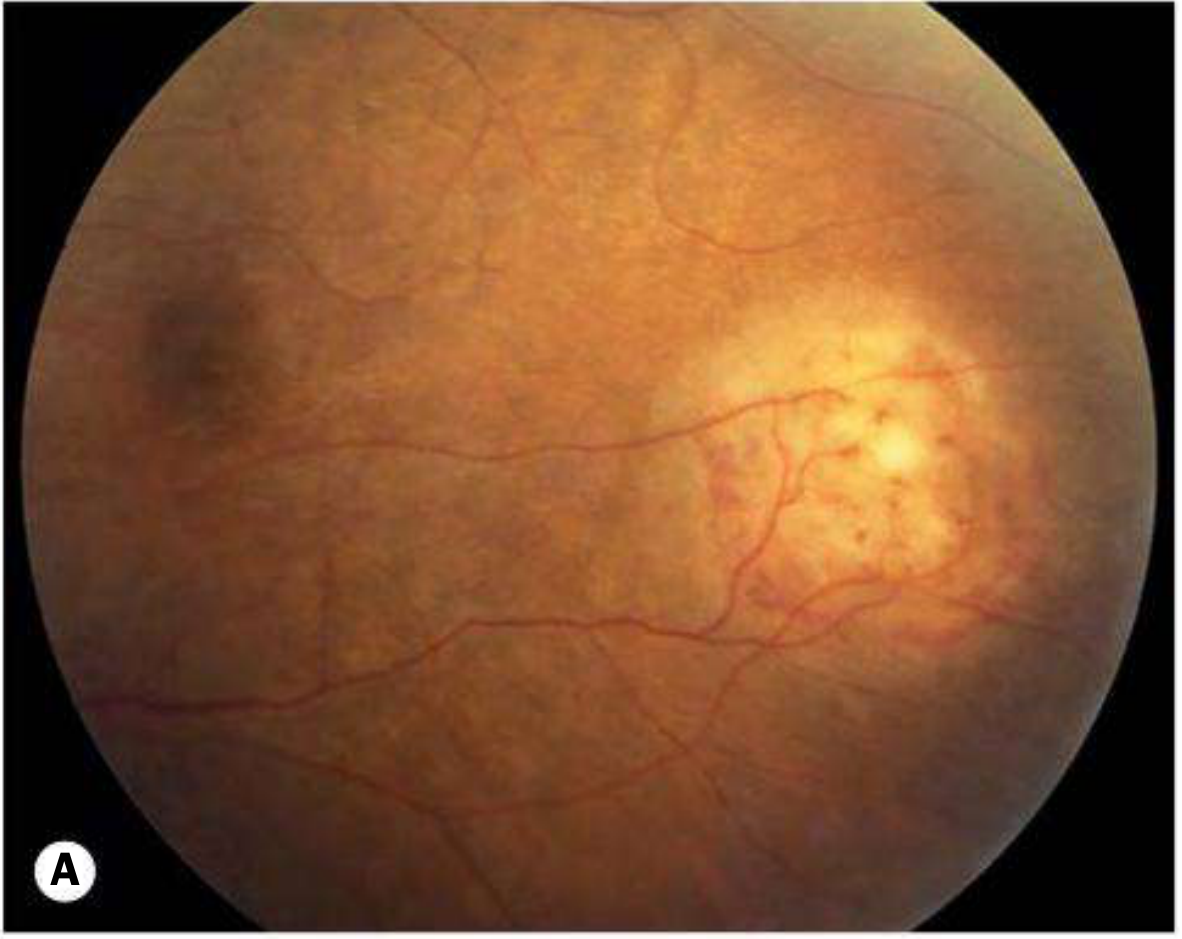
- A large abscess-like tubercle is termed a tuberculoma
- In AIDS, extensive choroidal infiltration can occur
- Choroidal tubercles on fundoscopy are pathognomonic of miliary TB (Tintinalli)
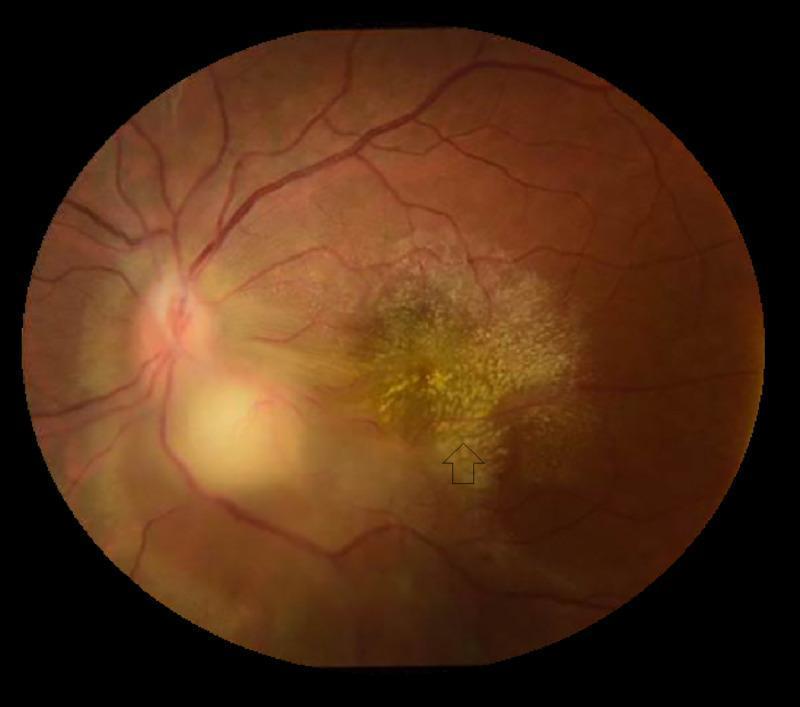
b. Serpiginoid (Serpiginous-like) Choroiditis
A pattern increasingly recognized as strongly suggestive of TB — multifocal choroiditis spreading centrifugally in a serpiginous pattern. Choroiditis tracking retinal vessels has reasonable specificity for TB.
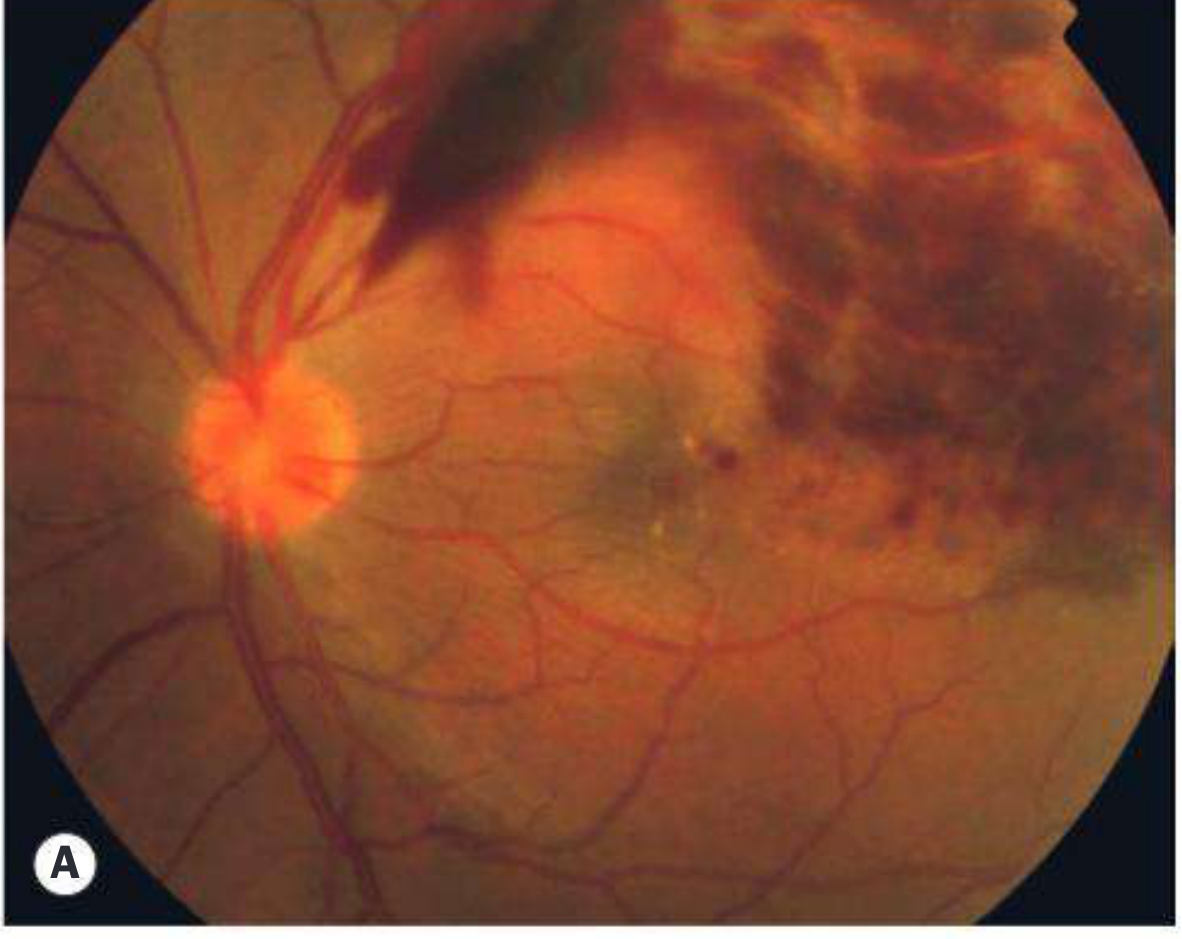
c. Retinal Vasculitis (Periphlebitis — Eales-type)
- Predominantly venous (periphlebitis)
- Retinal haemorrhages are common
- Vascular occlusion → extensive ischaemia → preretinal/disc neovascularization
- Eales disease (peripheral periphlebitis with neovascularization) is hypothesized to represent a hypersensitivity reaction to TB
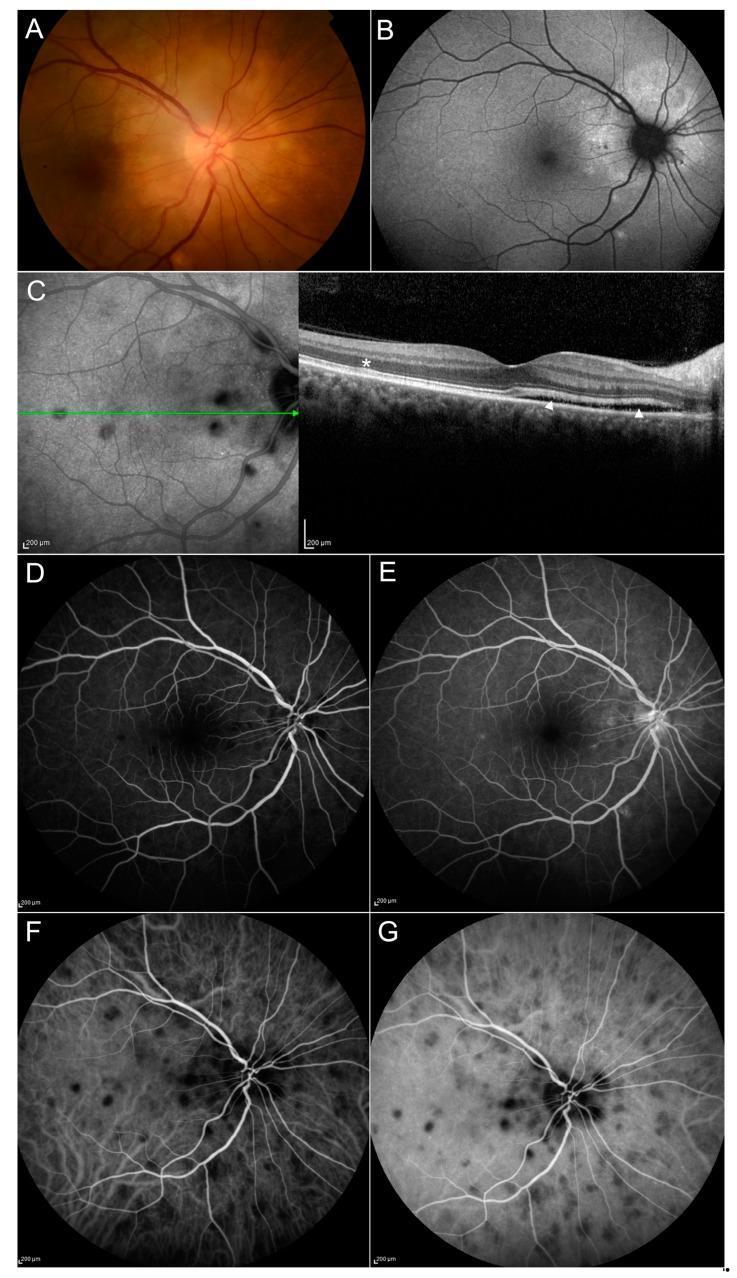
d. Multimodal Imaging Panel
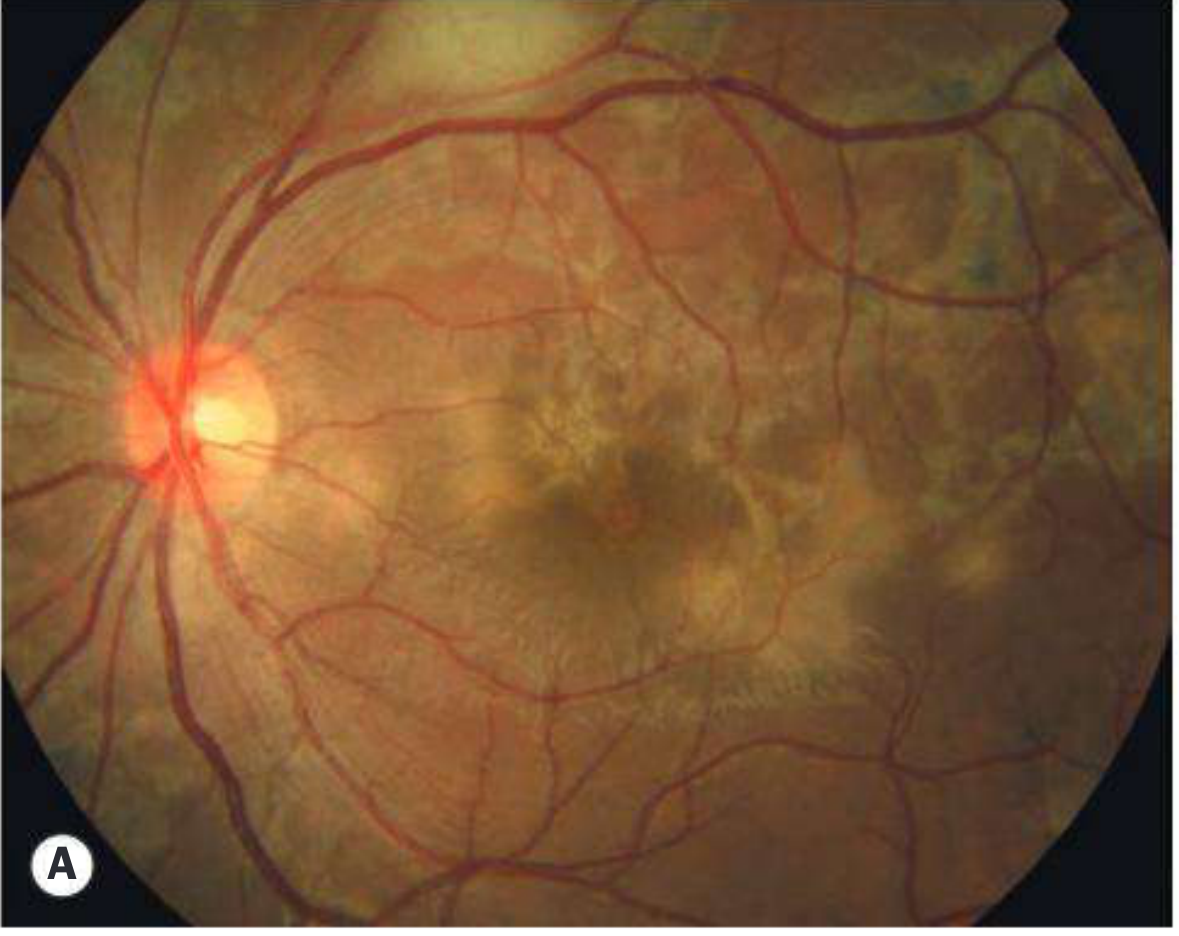
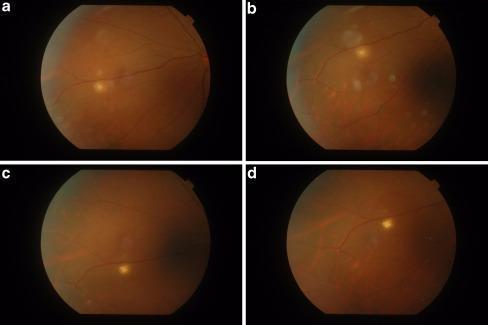
e. Choroidal Tubercle — Progression/Healing
3. Vitreous
- Viritis is very common — may be secondary to anterior, intermediate, or posterior foci
- Macular complications: cystoid macular oedema and epiretinal membrane formation
4. Adnexal / Other Manifestations
| Structure | Feature |
|---|---|
| Eyelids | Reddish-brown nodules — lupus vulgaris |
| Optic nerve | Optic neuropathy, neuroretinitis |
| Retina | Exudative retinal detachment |
5. Investigation
| Test | Notes |
|---|---|
| Tuberculin skin test (TST/Mantoux) | Positive within 48 hours in active/latent TB |
| IGRA (T-SPOT.TB / QuantiFERON) | ~80% sensitivity; not affected by BCG vaccination; detects latent TB |
| Aqueous/vitreous PCR | Low yield but most specific; ZN stain for AFB on Ziehl-Neelsen, culture on Löwenstein-Jensen medium |
| Chest X-ray / CT / PET-CT | Systemic assessment |
| HIV testing | Mandatory |
| Sputum PCR | For active pulmonary disease |
6. Treatment
- Four-drug anti-TB therapy (HRZE initially) prescribed and monitored by a TB specialist
- Ethambutol requires optic neuropathy monitoring
- Rifabutin can paradoxically cause anterior uveitis
- Concomitant topical and systemic steroids reduce inflammation-induced damage, especially in early weeks (also mitigate paradoxical worsening)
- Laser photocoagulation to ischaemic retina for preretinal neovascularization
- Anti-TB therapy in latent TB-associated uveitis halves recurrence risk and delays first recurrence
Key diagnostic pearl: Ocular TB is frequently a diagnosis of exclusion — made clinically based on TB exposure history, positive immunological tests, and response to treatment, in the absence of other identifiable causes. Choroidal tubercles on fundoscopy remain pathognomonic of miliary TB.
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., pp. 498–499; Tintinalli's Emergency Medicine, 9th ed.
Eye manifestation of syphillis
Finding Sources
Finding Sources
Searching PubMed
ocular syphilis clinical manifestations
Reading File
Reading File
Reading File
Searching Images
ocular syphilis uveitis interstitial keratitis fundus
Finding Sources
Loading Image
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
This is a shared conversation. Sign in to Orris to start your own chat.