Hey 👋👋 Can you tell me the physiological basis of tetany in hypocalcemia 🤔🤔 Also, please add a note on hypercalcemia 🫠🫠
Physiological Basis of Tetany in Hypocalcemia
The Core Mechanism: Calcium and Membrane Excitability
- The threshold potential shifts closer to the resting membrane potential
- Nerve and muscle cell membranes become hyperexcitable
- A smaller-than-normal stimulus - or even no stimulus at all - is enough to trigger spontaneous action potentials
- The result is repetitive, involuntary firing of peripheral nerves and skeletal muscle = tetany
"Hypocalcemia increases the excitability of nerve and muscle cells, which can lead to tetany." - Frameworks for Internal Medicine, p. 6298
"The archetypical presentation of hypocalcemia is tetany, classically diagnosed by the Chvostek sign... or the Trousseau sign." - Morgan & Mikhail's Clinical Anesthesiology, p. 4807
Important Note: Ionized vs. Total Calcium
Clinical Manifestations of Hypocalcemia (from mild to severe)
| Severity | Manifestations |
|---|---|
| Mild | Perioral and peripheral paresthesias, numbness, tingling |
| Moderate | Muscle twitching, cramps, carpopedal spasm, hyperreflexia |
| Severe | Tetany, laryngospasm/bronchospasm, seizures |
| Cardiac | QT interval prolongation, arrhythmias, hypotension, CHF |
| CNS | Irritability, depression, psychosis; raised intracranial pressure (chronic) |
Sources: Fitzpatrick's Dermatology, p. 4994; Morgan & Mikhail's Clinical Anesthesiology, Table 35-8; Harrison's Principles 22E, p. 1506
Classic Bedside Signs
"Trousseau's sign is more specific for hypocalcemia than Chvostek's sign." - Frameworks for Internal Medicine, p. 6322
Causes of Hypocalcemia Leading to Tetany
- PTH-related - Hypoparathyroidism (post-surgical most common), congenital, autoimmune
- Vitamin D-related - Deficiency, malabsorption
- Magnesium deficiency - Inhibits PTH secretion AND causes PTH resistance
- CKD - Reduced 1α-hydroxylase activity → reduced active vitamin D
- Acute pancreatitis - Calcium saponification
- Alkalosis - Reduces ionized calcium (hyperventilation tetany)
- Citrated blood transfusions - Chelates ionized calcium
Harrison's Principles 22E, p. 1494-1511; Katzung's Basic & Clinical Pharmacology 16E, p. 577
Note on Hypercalcemia
The Classic Mnemonic: "Bones, Stones, Moans, and Abdominal Groans"
| Domain | Manifestations |
|---|---|
| Bones | Bone pain, fractures, osteoporosis, osteitis fibrosa cystica |
| Stones | Nephrolithiasis, polyuria (nephrogenic DI), renal insufficiency |
| Groans (abdominal) | Constipation, nausea/vomiting, peptic ulcer disease, pancreatitis, gallstones |
| Moans (psychiatric) | Depression, lethargy, confusion, psychosis, seizures (severe) |
Robbins Pathologic Basis of Disease, p. 1660; Textbook of Family Medicine 9e, p. 1533
Physiological Basis of Hypercalcemia Symptoms
- Skeletal muscle: weakness, fatigue, hypotonia
- CNS: lethargy, confusion, coma (at very high levels)
- Smooth muscle: constipation (GI hypomotility)
- Heart: shortened QT interval, bradycardia, arrhythmias; calcium can be deposited in valves (mitral/aortic calcification)
- Kidney: impairs ADH action → nephrogenic diabetes insipidus → polyuria/polydipsia
"Hypercalcemia decreases neuromuscular excitability, which can lead to cardiac dysrhythmias, lethargy, disorientation, and death." - Frameworks for Internal Medicine, p. 6299
Key Causes
- Primary hyperparathyroidism (most common overall) - solitary adenoma (~80%), hyperplasia (~15%), rarely carcinoma (<1%)
- Malignancy (most common cause of symptomatic hypercalcemia) - typically Ca >14 mg/dL via PTHrP, osteolytic metastases, or ectopic 1,25(OH)₂D
- Others: granulomatous diseases (sarcoidosis), vitamin D toxicity, thiazide diuretics, lithium, immobilization, thyrotoxicosis, familial hypocalciuric hypercalcemia (FHH)
Primary hyperparathyroidism + malignancy account for ~90% of all cases - Robbins, p. 1682
ECG Changes - Quick Comparison
| Condition | QT interval |
|---|---|
| Hypocalcemia | Prolonged QT |
| Hypercalcemia | Shortened QT |
Management of Hypercalcemia (Summary)
| Severity | Approach |
|---|---|
| Mild (≤12 mg/dL) | Hydration, treat underlying cause, discontinue offending meds |
| Moderate (12-15 mg/dL) | Vigorous IV saline hydration + bisphosphonates (pamidronate/zoledronate) |
| Severe (≥15 mg/dL or symptomatic) | Aggressive IV saline diuresis + loop diuretics (furosemide) + IV bisphosphonates/denosumab; dialysis if renal/cardiac failure |
| Definitive (PHPT) | Parathyroidectomy - the only cure |
Harrison's Principles 22E, p. 1486; Textbook of Family Medicine 9e, p. 1573-1576; Katzung's 16E, p. 571
Create a visual diagram of calcium's effect on membrane potential
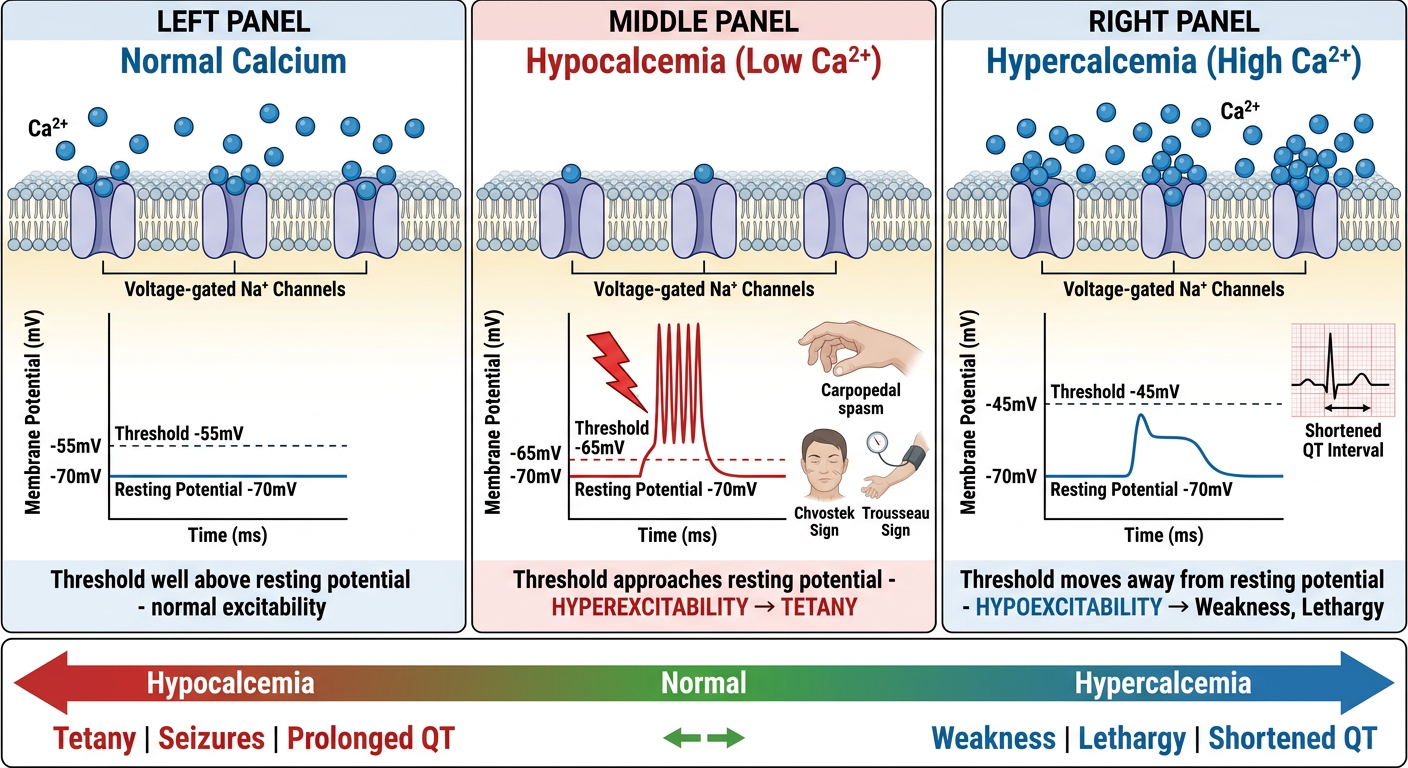
A clean educational medical diagram showing calcium's effect on membrane excitability and action potential threshold. The diagram has three panels side by side: LEFT PANEL - "Normal Calcium": A neuron membrane with calcium ions (Ca2+) shown binding to voltage-gated sodium channels on the outer surface. A graph below shows resting membrane potential at -70mV, threshold at -55mV, with a normal gap between them. Label: "Threshold well above resting potential - normal excitability" MIDDLE PANEL - "Hypocalcemia (Low Ca2+)": Same membrane with fewer/absent calcium ions on channels. The threshold line drops closer to the resting potential (e.g., threshold shifts to -65mV, nearly touching -70mV resting). A lightning bolt symbol shows spontaneous action potential firing. Label: "Threshold approaches resting potential - HYPEREXCITABILITY → TETANY". Small illustration of carpopedal spasm (hand in main d'accoucheur position) and Chvostek/Trousseau signs. RIGHT PANEL - "Hypercalcemia (High Ca2+)": Membrane with excess calcium ions heavily coating channels. The threshold line rises further from resting potential (e.g., threshold at -45mV). Shows a flat/blunted action potential. Label: "Threshold moves away from resting potential - HYPOEXCITABILITY → Weakness, Lethargy". Small ECG strip showing shortened QT interval. BOTTOM SECTION: A horizontal spectrum bar from left to right: "Hypocalcemia" → "Normal" → "Hypercalcemia" with arrows, color-coded red to green to blue. Below the bar, key effects listed: Tetany | Seizures | Prolonged QT ←→ Weakness | Lethargy | Shortened QT. Style: Clean medical illustration, white background, bold labels, professional textbook quality. Color scheme: red for hypocalcemia, green for normal, blue for hypercalcemia.
-
Left (Hypocalcemia - Red): With fewer Ca²⁺ ions binding to voltage-gated Na⁺ channels, the stabilizing effect is lost. The threshold potential drops toward the resting membrane potential (-70 mV), so almost no stimulus is needed to fire an action potential - neurons and muscles fire spontaneously → tetany, carpopedal spasm, seizures, prolonged QT.
-
Middle (Normal - Green): Ca²⁺ maintains an adequate gap between resting potential and threshold. Cells only fire when genuinely stimulated.
-
Right (Hypercalcemia - Blue): Excess Ca²⁺ over-stabilizes the channels, pushing the threshold further from resting potential. A much larger stimulus is needed to fire → weakness, lethargy, hypotonia, constipation, shortened QT.
Thank you ☺️☺️