CVS examination in medicine
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Finding Sources
I now have comprehensive content from Harrison's and Fuster's Heart. Let me compile a thorough, well-organized response.
Cardiovascular System (CVS) Examination
Sources: Harrison's Principles of Internal Medicine 22E (2025) and Fuster & Hurst's The Heart, 15th Edition
Overview
The CVS examination follows the classical sequence: General Inspection → Blood Pressure → Jugular Venous Pulse → Arterial Pulse → Precordial Inspection & Palpation → Auscultation. Each component provides hemodynamic information that builds a complete clinical picture.
1. General Inspection
Look for signs that point to underlying cardiac pathology:
- Dyspnea at rest - tachypnea, use of accessory muscles
- Cyanosis (central vs peripheral)
- Pallor, jaundice (in severe RHF with hepatic congestion)
- Malar flush - classic in mitral stenosis
- Peripheral edema, ascites - signs of right heart failure
- Clubbing - congenital cyanotic heart disease, infective endocarditis
- Splinter hemorrhages, Osler's nodes, Janeway lesions - infective endocarditis
- Xanthelasmata, corneal arcus - hyperlipidemia
- Specific syndromes: Marfan's (tall, arachnodactyly, lens dislocation, AR), Down's (ASD/VSD), Turner's (coarctation)
2. Blood Pressure Measurement
Accurate measurement requires careful technique:
-
Patient seated, arm at heart level, feet on floor, back supported, after 5-10 min of rest
-
Cuff bladder: 80% of arm circumference in length, 40% in width (too small = overestimate; too large = underestimate)
-
Inflate 30 mmHg above expected systolic; release at 2-3 mmHg/s
-
Systolic = first Korotkoff sound (K1); Diastolic = fifth Korotkoff sound (K5)
-
Measure both arms - a difference >15-20 mmHg suggests subclavian stenosis or aortic dissection
-
Pulsus paradoxus: inspiratory fall in systolic BP >10 mmHg - seen in pericardial tamponade, massive PE, severe obstructive lung disease. Measured as the difference between K1 heard only on expiration vs K1 heard throughout the cycle.
-
Pulsus alternans: beat-to-beat variability in pulse amplitude with regular rhythm - indicates severe LV systolic dysfunction
-
Very low/zero diastolic pressures occur in chronic severe AR or large AV fistula ("diastolic run-off")
-
Harrison's Principles of Internal Medicine 22E, p. 1905
3. Jugular Venous Pressure (JVP) and Waveform
The JVP is the single most important bedside measurement for estimating volume status.
Technical points:
- Use the internal jugular vein (preferred over external, which is valved and not directly in line with the SVC/RA)
- Patient at 30-45° elevation; vertical distance from the sternal angle (angle of Louis) to the top of the venous column
- Distance >4.5 cm above the sternal angle at 30° is abnormal
- The clavicle is an alternative reference: pulsations above it in the sitting position are clearly abnormal (distance from clavicle to RA is ≥10 cm)
- Bedside CVP is in cmH₂O; convert to mmHg (1.36 cmH₂O = 1.0 mmHg)
- An RA pressure >10 mmHg predicts pulmonary wedge pressure >22 mmHg with 88% positive predictive value in heart failure
Distinguishing JVP from carotid pulse:
| Feature | JVP | Carotid |
|---|---|---|
| Pulsations | Biphasic (in sinus rhythm) | Monophasic |
| Compressibility | Obliterated by light pressure | Not easily obliterated |
| Positional change | Changes with posture/inspiration | No change |
JVP Waveform Components
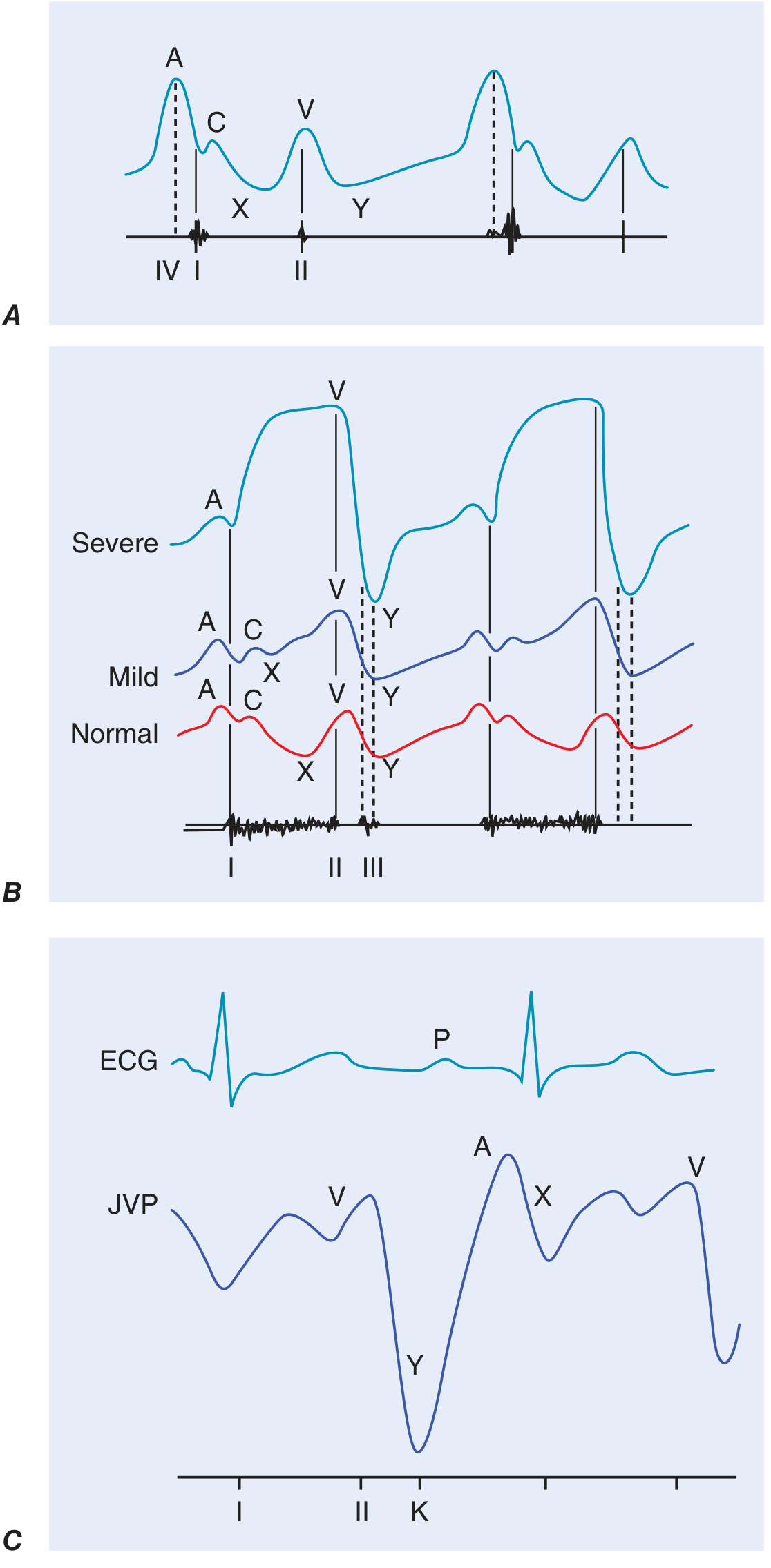
| Wave/Descent | Mechanism | Timing | Abnormalities |
|---|---|---|---|
| a wave | Right atrial presystolic contraction | After P wave, before S1 | Prominent: reduced RV compliance, tricuspid stenosis; Absent: atrial fibrillation; Cannon a waves: AV dissociation (diagnoses VT) |
| c wave | Tricuspid valve pushed into RA during early systole | Interrupts x descent | Small, often not visible |
| x descent | Fall in RA pressure after tricuspid opening | After a wave | Exaggerated: pericardial constriction/tamponade; Absent: tricuspid regurgitation |
| v wave | Atrial filling during ventricular systole | During ventricular systole | Prominent ("cv waves"): tricuspid regurgitation - waveform becomes "ventricularized" |
| y descent | RA pressure fall after tricuspid valve opens | After v wave | Rapid/deep: constrictive pericarditis (along with pericardial knock); Slow/blunted: tricuspid stenosis, tamponade |
Kussmaul's sign: paradoxical rise in JVP with inspiration - seen in constrictive pericarditis, RV failure, restrictive cardiomyopathy (normally JVP falls with inspiration).
Abdominojugular reflux (hepatojugular reflux): sustained JVP rise >3 cm with 15-30 seconds of firm right upper quadrant pressure - positive in right heart failure and elevated central venous pressure.
- Harrison's Principles of Internal Medicine 22E, p. 1904-1905
4. Arterial Pulse Examination
Technique: Palpate the carotid or brachial arteries. Assess amplitude, contour, rate, and rhythm. Also palpate all peripheral pulses (radial, femoral, popliteal, posterior tibial, dorsalis pedis).
Abnormal Pulse Patterns
| Pulse Type | Description | Associated Condition |
|---|---|---|
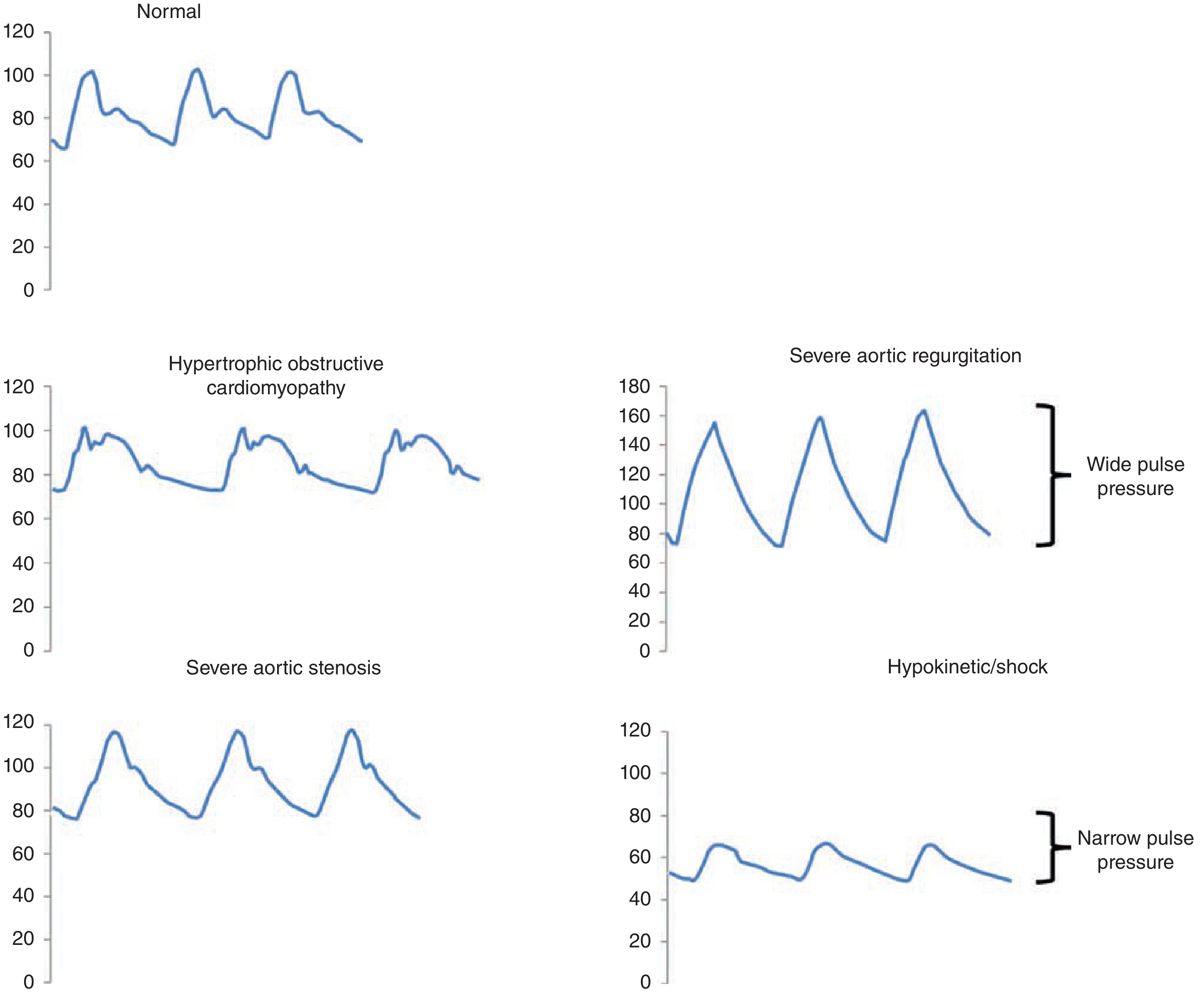
| Parvus et tardus | Reduced amplitude (parvus) + delayed, slurred upstroke with late peak (tardus) | Severe aortic stenosis |
| Corrigan's (water-hammer) pulse | Sharp, rapid rise and rapid fall-off ("collapsing") | Chronic severe aortic regurgitation |
| Bisferiens pulse | Two systolic peaks | Severe AR, HOCM |
| Pulsus alternans | Beat-to-beat variation in amplitude (regular rhythm) | Severe LV systolic dysfunction |
| Pulsus paradoxus | >10 mmHg systolic drop with inspiration | Cardiac tamponade, massive PE, severe obstructive lung disease |
| Small, thready pulse | Narrow pulse pressure | Cardiogenic shock, severe AS, tamponade |
| Jerky pulse | Sharp rise, sudden late collapse | HOCM |
Simultaneous radial-femoral palpation: a femoral delay suggests coarctation of the aorta.
Peripheral vascular examination: auscultate for bruits (carotid, subclavian, renal, femoral). A bruit extending into diastole or a palpable thrill indicates severe obstruction. The ankle-brachial index (ABI) - lower ankle pressure divided by the higher arm pressure - quantifies peripheral arterial disease.
- Fuster & Hurst's The Heart, 15th Edition, p. 81-82
5. Inspection and Palpation of the Precordium
Inspection
- Apex beat: normally visible in the 5th intercostal space, midclavicular line in thin adults
- Visible pulsations elsewhere = abnormal
- Left anterior chest wall heave: enlarged/hyperdynamic LV or RV
- Right upper parasternal pulsation: ascending aortic aneurysm
Palpation
Patient in supine position (30°); enhanced by left lateral decubitus position.
Apex beat assessment:
- Normal: <2 cm diameter, brief outward movement
- Displaced laterally/downward: LV cavity enlargement
- Sustained/heaving: pressure overload (AS, hypertension)
- Palpable S4 (presystolic impulse): reduced LV compliance, ischemia, LVH
- Palpable S3: rapid early filling, heart failure
- Ectopic impulse: LV aneurysm (dyskinetic, separate from apex)
- Triple cadence (triple ripple): HOCM - palpable S4 + bisferiens systolic pulse
Right ventricular assessment:
- Parasternal lift/heave: RV pressure or volume overload
- Confirmed by: loud/palpable P2 (pulmonary hypertension) or CV waves in JVP (TR)
- Subxiphoid palpation can also detect RV impulse
Thrills: palpable turbulence, indicating grade ≥4 murmur. Location identifies murmur origin.
- Harrison's Principles of Internal Medicine 22E, p. 1906-1907
6. Cardiac Auscultation
Heart Sounds
First Heart Sound (S1)
- Mitral + tricuspid valve closure
- Loud S1: early rheumatic MS, hyperkinetic states, short PR interval, tachycardia
- Soft S1: advanced calcified MS, long PR interval, beta-blockers, LV contractile dysfunction
- Intensity also reduced by: obesity, COPD, pericardial effusion, pneumothorax
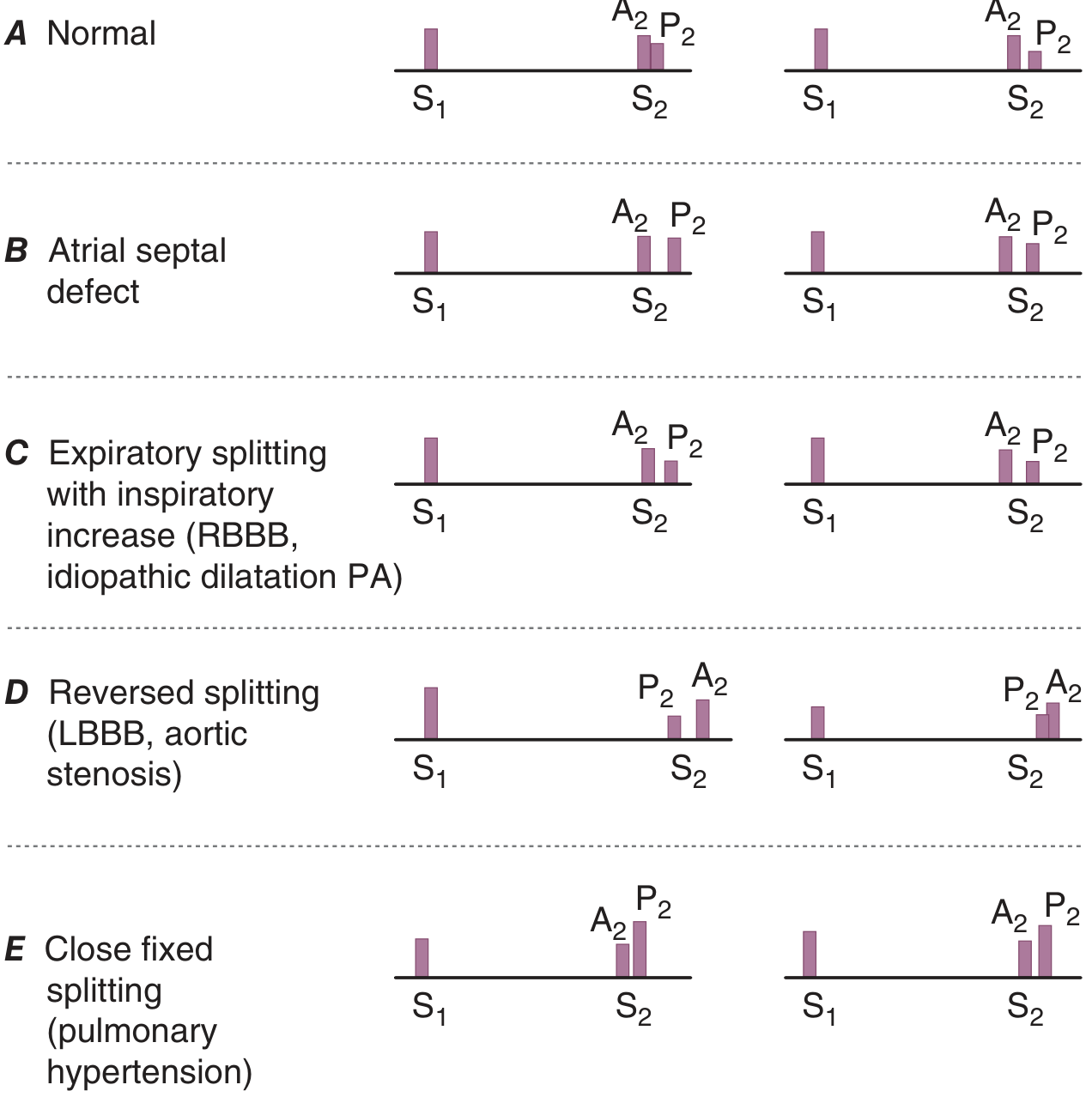
Second Heart Sound (S2)
- Aortic (A2) + pulmonic (P2) valve closure
- A2 heard best at the right upper sternal border; P2 at the left upper sternal border
| S2 Splitting Pattern | Mechanism | Conditions |
|---|---|---|
| Physiologic (normal) | Widens on inspiration, narrows on expiration | Normal |
| Wide splitting | Delayed P2 or early A2 | RBBB (delayed P2), severe MR (early A2) |
| Fixed splitting | Wide, does not change with respiration | Atrial septal defect (ASD) |
| Reversed (paradoxical) splitting | P2 precedes A2; widens on expiration | LBBB, RV pacing, severe AS, HOCM, acute ischemia |
| Narrow/single S2 | A2 and P2 fused | Pulmonary arterial hypertension (loud P2), severe AS or PS |
S3 (Third Heart Sound)
- During rapid diastolic filling
- Normal: children, adolescents, young adults, athletes, pregnancy
- Abnormal in adults: heart failure (equally common in HFrEF and HFpEF), volume overload (MR, AR, VSD)
- Left-sided S3: low-pitched, best at the apex; Right-sided S3: lower left sternal border, increases with inspiration
- Predictive of cardiovascular morbidity and mortality in chronic heart failure
S4 (Fourth Heart Sound)
- During atrial systole (presystolic)
- Indicates reduced ventricular compliance requiring increased atrial contribution
- Heard in: LVH, active ischemia/infarction, hypertrophic cardiomyopathy, AS
- Not present in atrial fibrillation (no atrial contraction)
Additional Sounds
| Sound | Timing | Features | Cause |
|---|---|---|---|
| Ejection click | Early systole (sharp, high-pitched) | Correlates with carotid upstroke; pulmonic click decreases with inspiration | Bicuspid aortic/pulmonary valve, aortic/pulmonary root dilation |
| Mid-systolic click | Mid-systole | May be multiple; best at apex | Mitral valve prolapse (MVP) |
| Opening snap (OS) | Early diastole (high-pitched, after S2) | Short A2-OS interval = severe MS | Mitral stenosis (pliable leaflets) |
| Pericardial knock (PK) | Early diastole (high-pitched, slightly later than OS) | Coincides with rapid y descent in JVP | Constrictive pericarditis |
| Tumor plop | Diastole (lower-pitched) | Positional | Left atrial myxoma |
- Harrison's Principles of Internal Medicine 22E, p. 1907-1908
7. Cardiac Murmurs
Murmurs are caused by turbulent blood flow. Graded 1-6 (thrill present at grade ≥4). Characterize each murmur by: timing, location, radiation, intensity, quality (pitch/character), and response to maneuvers.
Systolic Murmurs
| Murmur | Timing | Location | Radiation | Key Features |
|---|---|---|---|---|
| Aortic stenosis (AS) | Mid-systolic (crescendo-decrescendo) | Right upper sternal border | Carotids, occasionally apex (Gallavardin) | Parvus et tardus pulse, soft A2, S4 |
| Mitral regurgitation (MR) - holosystolic | Holosystolic | Apex | Left axilla (posterior leaflet lesion radiates anteriorly/base; anterior leaflet radiates posteriorly) | Soft S1, S3, displaced apex |
| Tricuspid regurgitation (TR) | Holosystolic or early systolic | Lower left sternal border | Right | Increases with inspiration (Carvallo's sign), CV waves in JVP |
| VSD | Holosystolic | Left sternal border | Right | Harsh, loud; thrill common |
| HOCM | Mid-systolic | Lower left sternal border / apex | Decreases with squatting/handgrip; increases with Valsalva/standing | Jerky pulse, double apical impulse |
| Pulmonary stenosis (PS) | Mid-systolic | Left upper sternal border | Left shoulder | Ejection click, soft P2 |
| MVP | Late systolic (preceded by click) | Apex | — | Click moves earlier with standing/Valsalva |
Diastolic Murmurs (always pathological)
| Murmur | Timing | Location | Key Features |
|---|---|---|---|
| Aortic regurgitation (AR) | Early diastolic (decrescendo, high-pitched, blowing) | Left sternal border (lean forward, expiration) | Wide pulse pressure, Corrigan's pulse, Austin Flint murmur (functional MS at apex) |
| Mitral stenosis (MS) | Mid-diastolic (rumble, low-pitched) | Apex (left lateral decubitus) | Opening snap precedes it, loud S1, presystolic accentuation if sinus rhythm |
| Tricuspid stenosis (TS) | Mid-diastolic | Lower left sternal border | Increases with inspiration |
| PR (Graham Steell murmur) | Early diastolic | Left upper sternal border | Pulmonary hypertension, high-pitched |
Continuous Murmurs
- PDA: machinery murmur, left infraclavicular area
- AV fistula, ruptured sinus of Valsalva
8. Dynamic Auscultation - Bedside Maneuvers
| Maneuver | Effect on Preload/Afterload | Murmurs that increase | Murmurs that decrease |
|---|---|---|---|
| Valsalva (strain phase) | ↓ Preload | HOCM, MVP (click moves earlier) | AS, MR, TR, VSD |
| Standing | ↓ Preload | HOCM, MVP | AS, MR |
| Squatting | ↑ Preload + ↑ Afterload | AS, MR, AR, VSD | HOCM, MVP (click moves later) |
| Handgrip (isometric) | ↑ Afterload | MR, AR, VSD | AS, HOCM |
| Inspiration | ↑ RV filling | TR, TS, PS (right-sided murmurs) - Carvallo's sign | Left-sided murmurs |
| Amyl nitrite | ↓ Afterload, ↑ HR | AS, HOCM | MR, VSD |
9. Peripheral Signs of Specific Cardiac Conditions
| Sign | Description | Condition |
|---|---|---|
| Corrigan's (water-hammer) pulse | Bounding, rapidly collapsing | Aortic regurgitation |
| de Musset's sign | Head nodding with pulse | Severe AR |
| Quincke's sign | Visible capillary pulsation in nail bed | AR |
| Duroziez's sign | Systolic/diastolic femoral bruit with compression | AR |
| Hill's sign | Popliteal BP > brachial BP by >20 mmHg | AR |
| Malar flush | Mitral facies, bluish-red cheeks | Mitral stenosis |
| Cannon a waves | Large JVP a waves | AV dissociation (VT) |
| Kussmaul's sign | Paradoxical rise in JVP with inspiration | Constrictive pericarditis, RV failure |
Summary: Sequence of CVS Examination
- General inspection - dyspnea, cyanosis, peripheral signs, body habitus
- Hands - clubbing, splinter hemorrhages, peripheral perfusion (CRT)
- Face - malar flush, xanthelasma, corneal arcus, central cyanosis (tongue)
- Neck - JVP (height + waveform), carotid pulse (character), thyroid
- Chest - inspect, palpate (apex, thrills, heaves, RV impulse), auscultate (4 areas + axilla + back)
- Abdomen - hepatomegaly (pulsatile in TR), ascites, aortic aneurysm
- Legs - peripheral pulses, edema, ABI if PAD suspected
- BP - both arms; pulsus paradoxus if tamponade/COPD suspected
Sources:
- Harrison's Principles of Internal Medicine 22E (2025) - Chapter 246: Cardiovascular Examination, pp. 1904-1909
- Fuster & Hurst's The Heart, 15th Edition - Chapter 2: Clinical Cardiovascular Examination, pp. 56-82
This is a shared conversation. Sign in to Orris to start your own chat.