Aldosterone escape
Reading File
Finding Sources
Searching PubMed
"aldosterone escape" sodium retention natriuresis
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a thorough breakdown of aldosterone escape.
Aldosterone Escape
Definition
Aldosterone escape is the phenomenon whereby the kidneys escape from the sodium-retaining effects of chronically elevated aldosterone after a period of initial sodium and water retention. Despite the continued presence of high aldosterone levels, urinary sodium excretion returns to match daily sodium intake, and further sodium accumulation stops. Critically, potassium wasting and hypertension persist - only sodium retention is "escaped."
Sequence of Events
-
Initial phase (Days 0-2): High aldosterone (endogenous or exogenous) causes sodium and water retention. Urinary sodium excretion drops sharply. ECF volume begins expanding.
-
Volume expansion: ECF volume rises by ~10-15% above normal.
-
Arterial pressure rise: The expanded volume raises mean arterial pressure by ~15-25 mmHg.
-
Escape (Day 2 onwards): Urinary sodium excretion returns to equal intake. Further sodium accumulation stops despite ongoing high aldosterone. This is the "escape."
-
Steady state: ECF volume remains ~10-15% above baseline, and hypertension persists, but sodium balance is re-established.
The figure below (from Guyton & Hall, Fig. 78.3) shows this perfectly in dogs given supra-physiologic aldosterone infusion:
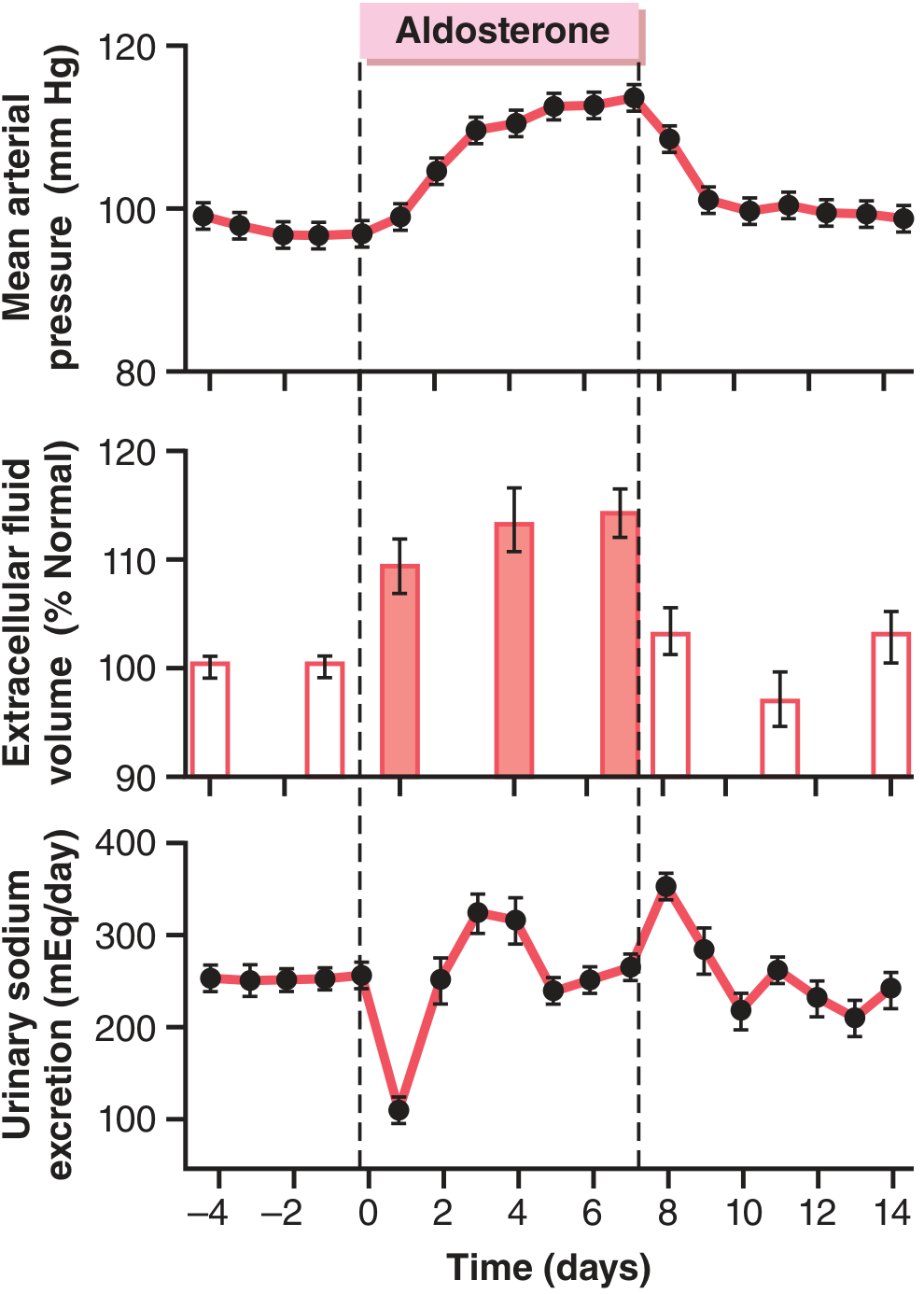
Note: Urinary sodium drops on Day 0, then returns to baseline by Day 2-4, coinciding with rising arterial pressure - the "escape."
Mechanisms of Escape
Three overlapping mechanisms drive the escape:
| Mechanism | How it works |
|---|---|
| Pressure natriuresis / diuresis | Rising arterial pressure directly increases sodium and water excretion by the kidney, the most dominant mechanism |
| Suppression of angiotensin II | Volume expansion suppresses renin → less Ang II → less tubular sodium reabsorption (proximal tubule) and less stimulation of aldosterone synthesis |
| Natriuretic peptides (ANP/BNP) | Atrial stretch from volume expansion releases ANP, which directly inhibits sodium reabsorption in the collecting duct and counteracts aldosterone |
"The primary reasons for this escape are suppression of Ang II formation and the pressure natriuresis and diuresis that occur when the arterial pressure rises."
- Guyton and Hall Textbook of Medical Physiology
What Does NOT Escape
| Effect | Escapes? |
|---|---|
| Sodium retention | YES - returns to normal |
| Hypertension | NO - persists throughout |
| Hypokalemia | NO - potassium continues to be lost |
| Metabolic alkalosis | NO - continues |
This is why primary hyperaldosteronism (Conn syndrome) presents with hypertension + hypokalemia, but NOT edema - the kidneys escaped the sodium retention, but potassium wasting and the resultant hypertension remain uncorrected.
Clinical Relevance
1. Primary hyperaldosteronism (Conn syndrome)
- Aldosterone escape explains the absence of edema despite massive sodium-retaining stimulus
- Hypertension develops and is sustained because pressure natriuresis maintains sodium balance at the cost of a higher blood pressure set-point
2. Heart failure and cirrhosis - FAILURE of aldosterone escape
- In these states, aldosterone escape is impaired
- Reduced cardiac output / portal hypertension → reduced renal perfusion → diminished distal tubular sodium delivery → the rise in arterial pressure cannot overcome sodium retention
- Natriuretic peptides are also blunted due to downregulation of receptors
- Result: continued sodium and water accumulation → edema and ascites
Goldman-Cecil Medicine notes that in heart failure, "arterial underfilling leads to diminished distal tubular sodium and water delivery, impaired aldosterone escape, and resistance to natriuretic peptide hormone."
3. RAAS blockade (ACE inhibitors, ARBs, aliskiren) - "Aldosterone escape" with drugs
- A different use of the same term: with chronic ACE inhibitor/ARB therapy, aldosterone levels initially fall but may rise again over months (via Ang II-independent pathways such as elevated potassium, ACTH, endothelin)
- This "aldosterone escape" from RAAS blockade is associated with accelerated progression of diabetic nephropathy and worse cardiovascular outcomes
- It is one rationale for adding an MRA (spironolactone/eplerenone) to ACE inhibitor therapy
Summary
| Feature | Detail |
|---|---|
| What escapes | Sodium retention |
| What does not escape | K+ wasting, hypertension, alkalosis |
| Primary mechanism | Pressure natriuresis |
| Supporting mechanisms | Ang II suppression, ANP/BNP release |
| Clinical model | Conn syndrome (no edema, but hypertension + hypokalemia) |
| Failure states | Heart failure, cirrhosis, nephrotic syndrome |
- Guyton and Hall Textbook of Medical Physiology, pp. 946-947
- Goldman-Cecil Medicine, p. 1194-1195
- Goodman & Gilman's The Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.