Clinical cases on LFT AND PFT
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
I now have rich source material from Harrison's, Bailey & Love, Murray & Nadel, and Quick Compendium of Clinical Pathology. Let me compile the full clinical cases response.
Clinical Cases: Liver Function Tests (LFT) & Pulmonary Function Tests (PFT)
PART 1 - LIVER FUNCTION TESTS (LFT)
Quick Reference: LFT Pattern Recognition
| Parameter | Hepatocellular Injury | Cholestatic/Obstructive |
|---|---|---|
| ALT / AST | >3x ULN (dominant) | <3x ULN |
| Alkaline Phosphatase (ALP) | <3x ULN | >3x ULN (dominant) |
| GGT | Elevated | Very elevated |
| Serum Cholesterol | Normal | Increased |
| Pruritus | Absent | Present |
| Bilirubin type | Both (conjugated > unconjugated in late) | Conjugated |
Harrison's Principles of Internal Medicine 22E - "patients with a hepatocellular process generally have a rise in the aminotransferases that is disproportionate to that in ALP, whereas patients with a cholestatic process have a rise in ALP that is disproportionate to that of the aminotransferases."
Bilirubin Metabolism - Step-by-Step Causes
| Step Disrupted | Pathologic Cause | Type of Hyperbilirubinemia |
|---|---|---|
| Excess heme conversion | Hemolysis, large hematoma, ineffective erythropoiesis | Unconjugated |
| Excess delivery to liver | Cirrhosis (blood shunting), right heart failure | Unconjugated |
| Poor hepatocyte uptake | Gilbert syndrome, rifampin, probenecid | Unconjugated |
| Impaired conjugation | Crigler-Najjar syndrome, hypothyroidism | Unconjugated |
| Impaired canalicular secretion | Hepatitis, sepsis, estrogen/cyclosporine | Conjugated |
| Benign excretory defects | Dubin-Johnson syndrome, Rotor syndrome | Conjugated |
| Bile duct obstruction (intrahepatic) | Primary biliary cholangitis, alcohol, pregnancy | Conjugated |
| Bile duct obstruction (extrahepatic) | PSC, tumor, stone, stricture, AIDS choledochopathy | Conjugated |
- Quick Compendium of Clinical Pathology 5th ed., p. 5
LFT CLINICAL CASES
CASE 1 - Full Vignette: The Yellow Medical Student
Vignette:
A 21-year-old male medical student presents to the outpatient clinic. He noticed mild yellowing of his eyes during exam season and reports fatigue. He skipped meals for 2 days due to stress. He takes no medications, does not drink alcohol, and has no sick contacts. On examination, he is mildly icteric. There is no hepatomegaly, no tenderness, no splenomegaly, and no signs of chronic liver disease.
LFT Results:
| Test | Value | Reference |
|---|---|---|
| Total Bilirubin | 3.2 mg/dL | <1.2 mg/dL |
| Direct (Conjugated) Bilirubin | 0.3 mg/dL | <0.3 mg/dL |
| Indirect (Unconjugated) Bilirubin | 2.9 mg/dL | <0.9 mg/dL |
| ALT | 22 U/L | 7-56 U/L |
| AST | 24 U/L | 10-40 U/L |
| ALP | 78 U/L | 44-147 U/L |
| Albumin | 4.2 g/dL | 3.5-5.0 g/dL |
| PT/INR | Normal | - |
Q1: What is the LFT pattern here?
Isolated unconjugated (indirect) hyperbilirubinemia with completely normal transaminases, ALP, albumin, and PT.
Q2: What is the most likely diagnosis?
Gilbert Syndrome - the most common benign hereditary cause of unconjugated hyperbilirubinemia. Due to a UGT1A1 promoter mutation causing reduced UDP-glucuronosyltransferase activity. Triggered by fasting, stress, or illness.
Q3: Why is there no jaundice in normal life?
Bilirubin stays below the threshold (~2.5 mg/dL) that causes visible scleral icterus in daily conditions. Fasting reduced hepatic glucuronidation, unmasking the condition.
Key Teaching Point: When unconjugated bilirubin is elevated in isolation with normal liver enzymes and no hemolysis markers, think Gilbert syndrome first. No treatment needed - reassure the patient.
CASE 2 - Short Case: The Alcoholic with Jaundice
Presentation: 48-year-old male, chronic alcohol user, presents with jaundice, nausea, and RUQ discomfort for 2 weeks. Spider naevi and palmar erythema noted.
LFT:
| Test | Value |
|---|---|
| AST | 180 U/L |
| ALT | 75 U/L |
| AST/ALT ratio | ~2.4:1 |
| ALP | 140 U/L (1.3x ULN) |
| Total Bilirubin | 4.5 mg/dL |
| GGT | 310 U/L (very high) |
| Albumin | 2.8 g/dL (low) |
| PT | Prolonged |
Interpretation:
- AST:ALT ratio >2:1 is a classical indicator of alcoholic hepatitis/liver disease
- Hepatocellular pattern: transaminases dominant over ALP
- Low albumin + prolonged PT indicate impaired synthetic function - this is chronic/severe
- Markedly elevated GGT: hallmark of alcohol-related liver damage. GGT is elevated in up to 70% of chronic alcoholics and correlates with alcohol consumption
Key Teaching Point: In alcohol-related liver disease, AST rises more than ALT (mitochondrial damage) and GGT is a sensitive marker for ongoing alcohol use. Low albumin and prolonged PT signal decompensation.
- Quick Compendium of Clinical Pathology 5th ed.; Harrison's 22E
CASE 3 - Short Case: The Itchy Middle-Aged Woman
Presentation: 52-year-old woman presents with fatigue, pruritus for 4 months, and mild jaundice. She has no pain. She takes no hepatotoxic drugs.
LFT:
| Test | Value |
|---|---|
| ALP | 580 U/L (>4x ULN) |
| GGT | 290 U/L |
| ALT | 62 U/L (<2x ULN) |
| AST | 55 U/L |
| Total Bilirubin | 3.8 mg/dL (conjugated) |
| Albumin | 3.9 g/dL (normal) |
| Anti-mitochondrial antibodies (AMA) | Positive |
Interpretation:
- Dominant ALP elevation (cholestatic pattern)
- Normal-range transaminases
- Pruritus + conjugated hyperbilirubinemia + positive AMA = Primary Biliary Cholangitis (PBC)
- Pruritus is classic for cholestasis - retained bile salts deposit in skin
- ALP from biliary epithelium; GGT confirms hepatic origin of ALP
Key Teaching Point: To confirm the source of a raised ALP, check GGT. If GGT is also raised, the ALP is of hepatic (biliary) origin. If GGT is normal, consider bone disease (Paget's disease, growing children, pregnancy).
CASE 4 - Comparison Table: Common Causes at a Glance
| Condition | ALT/AST | ALP | Bilirubin | Albumin | PT | Other |
|---|---|---|---|---|---|---|
| Viral Hepatitis (acute) | ↑↑↑ | Normal/↑ | Both ↑ | Normal | Normal/↑ | IgM anti-HAV, HBsAg |
| Alcoholic Hepatitis | ↑↑ (AST>ALT) | ↑ | ↑ | ↓ | ↑ | GGT ↑↑↑ |
| Obstructive Jaundice (stone/tumor) | Normal/↑ | ↑↑↑ | Conjugated ↑↑ | Normal | Normal | Pruritus, dark urine |
| Primary Biliary Cholangitis | ↑ | ↑↑↑ | Conjugated ↑ | Normal early | Late ↑ | AMA positive |
| Gilbert Syndrome | Normal | Normal | Unconjugated ↑ | Normal | Normal | Stress/fasting trigger |
| Cirrhosis (end-stage) | ↑ or normal | ↑ | Both ↑ | ↓↓ | ↑↑ | Low platelets |
| Liver Metastases | Moderate ↑ | ↑↑↑ | Variable | ↓ | Variable | ALP most sensitive |
ALP is the most sensitive marker of hepatic metastases compared with other hepatic chemistry analytes. - Quick Compendium of Clinical Pathology
PART 2 - PULMONARY FUNCTION TESTS (PFT)
Quick Reference: PFT Interpretation Algorithm
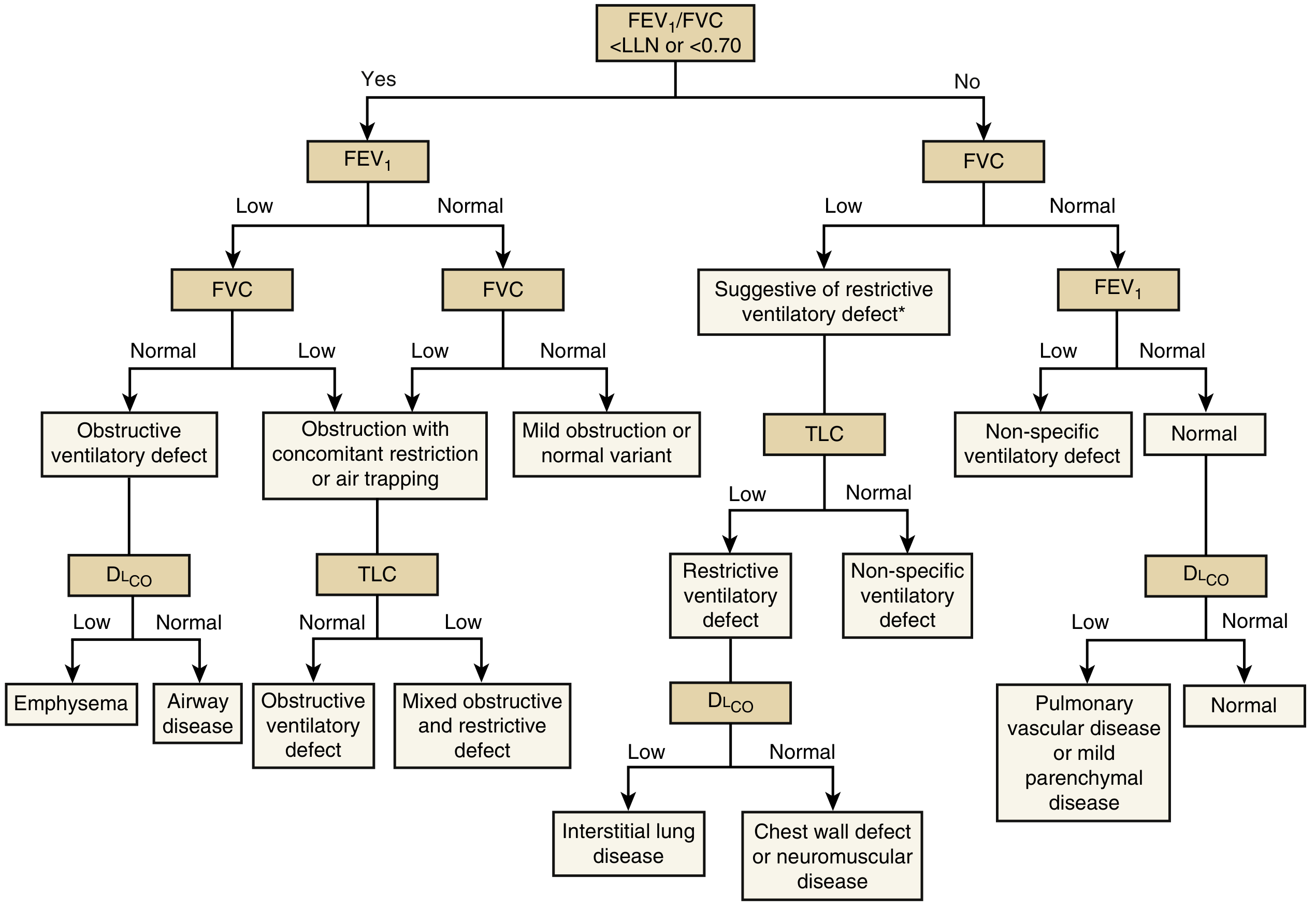
Algorithm for interpretation of pulmonary function tests. - Murray & Nadel's Textbook of Respiratory Medicine
Key Parameters & Normal Values
| Parameter | Meaning | Normal |
|---|---|---|
| FEV₁ | Forced Expiratory Volume in 1 second | >80% predicted |
| FVC | Forced Vital Capacity | >80% predicted |
| FEV₁/FVC ratio | Obstructive vs restrictive discriminator | >70% (0.70) |
| TLC | Total Lung Capacity | 80-120% predicted |
| DLCO | Diffusing capacity for CO (alveolar-capillary transfer) | >75% predicted |
| PEFR | Peak Expiratory Flow Rate | Age/height referenced |
Pattern Summary Table
| Pattern | FEV₁ | FVC | FEV₁/FVC | TLC | DLCO | Examples |
|---|---|---|---|---|---|---|
| Obstructive | ↓↓ | Normal or ↓ | <0.70 | Normal or ↑ | ↓ (emphysema) or Normal (asthma) | Asthma, COPD, emphysema, bronchiectasis |
| Restrictive | Normal or ↓ | ↓↓ | >0.70-0.80 | ↓ (confirms it) | ↓ (ILD) or Normal (chest wall) | IPF, sarcoidosis, kyphoscoliosis, obesity |
| Mixed | ↓↓ | ↓↓ | <0.70 | ↓ | ↓ | Combined fibrosis + emphysema |
- Bailey and Love's Surgery 28th Ed.; Murray & Nadel's Respiratory Medicine
PFT CLINICAL CASES
CASE 5 - Full Vignette: The Wheezing Young Woman
Vignette:
A 24-year-old woman presents to a clinic with episodic breathlessness, chest tightness, and wheezing that worsens at night and with exercise. She has eczema and allergic rhinitis. Her mother has asthma. Examination reveals mild bilateral expiratory wheezes. SpO₂ = 96% at rest.
PFT Results (pre-bronchodilator):
| Parameter | Measured | % Predicted |
|---|---|---|
| FEV₁ | 1.8 L | 62% |
| FVC | 3.2 L | 88% |
| FEV₁/FVC | 0.56 | - |
| PEFR | ↓↓ | 54% |
| DLCO | Normal | - |
Post-bronchodilator (salbutamol 400 mcg):
| Parameter | Measured | % Predicted | Change |
|---|---|---|---|
| FEV₁ | 2.45 L | 84% | +36% / +650 mL |
| FVC | 3.3 L | 91% | Unchanged |
Q1: What is the pattern?
Obstructive pattern: FEV₁/FVC <0.70. Normal DLCO (airway disease, not parenchymal destruction).
Q2: What does the post-bronchodilator response tell you?
A >12% and >200 mL increase in FEV₁ after bronchodilator is a significant bronchodilator response, confirming reversible airway obstruction = Asthma.
Q3: How does this differ from COPD/emphysema?
In COPD/emphysema, obstruction is not fully reversible. Also, in emphysema, DLCO is reduced (destroyed alveolar-capillary surface area). In asthma, DLCO is normal.
| Feature | Asthma | COPD/Emphysema |
|---|---|---|
| Age | Young (<40 typically) | Older, smoking history |
| Reversibility | Yes (>12%, >200 mL) | Minimal (<12%) |
| DLCO | Normal | Low (emphysema) |
| TLC | Normal or mildly ↑ | Markedly ↑ (hyperinflation) |
CASE 6 - Short Case: The Progressive Breathlessness in a Fibrosing Lung
Presentation: 62-year-old non-smoker male presents with progressively worsening exertional dyspnea and dry cough for 18 months. On exam: fine bibasal "velcro" crackles. SpO₂ drops to 90% on exertion.
PFT Results:
| Parameter | Measured | % Predicted |
|---|---|---|
| FEV₁ | 1.9 L | 72% |
| FVC | 2.1 L | 65% |
| FEV₁/FVC | 0.90 | - |
| TLC | 3.4 L (↓) | 58% |
| DLCO | 42% predicted | Markedly ↓ |
Interpretation:
- FEV₁/FVC >0.80 = Restrictive pattern
- Low TLC confirms true restriction (not just effort-dependent)
- Markedly reduced DLCO confirms parenchymal disease (thickened alveolar membrane)
- Clinical + PFT pattern = Idiopathic Pulmonary Fibrosis (IPF)
Key Teaching Point: Restrictive PFT (↓FVC, ↓TLC, normal or high FEV₁/FVC) + markedly reduced DLCO = interstitial lung disease until proven otherwise. TLC measured by plethysmography is the gold standard for confirming restriction.
CASE 7 - Short Case: The Chain Smoker with Hyperinflation
Presentation: 67-year-old male, 45 pack-years, barrel chest, pursed-lip breathing. Reports morning cough with sputum for >3 years and increasing exertional dyspnea.
PFT Results:
| Parameter | Measured | % Predicted |
|---|---|---|
| FEV₁ | 1.1 L | 38% |
| FVC | 2.7 L | 78% |
| FEV₁/FVC | 0.41 | - |
| TLC | 7.2 L (↑↑) | 135% |
| RV | 4.1 L (↑↑) | - |
| DLCO | 35% predicted | Markedly ↓ |
| Post-bronchodilator FEV₁ change | +5% | Not significant |
Interpretation:
- Severe obstructive pattern: FEV₁/FVC 0.41, FEV₁ 38% predicted = GOLD Stage III (Severe COPD)
- TLC markedly elevated = air trapping and hyperinflation (emphysema)
- Markedly reduced DLCO = destruction of alveolar-capillary surface area
- Minimal bronchodilator response = irreversible obstruction
GOLD COPD Severity by FEV₁ % predicted:
| Stage | FEV₁ % predicted |
|---|---|
| GOLD I (Mild) | ≥80% |
| GOLD II (Moderate) | 50-79% |
| GOLD III (Severe) | 30-49% |
| GOLD IV (Very Severe) | <30% |
CASE 8 - Comparison: Mixed Obstructive + Restrictive Pattern
Scenario: Combined pulmonary fibrosis and emphysema (CPFE) - a recognized but underdiagnosed entity.
PFT Finding:
- FEV₁/FVC: borderline low (<0.70)
- FVC: low
- TLC: near normal (hyperinflation from emphysema "cancels out" restriction from fibrosis)
- DLCO: markedly low (below what volumes alone would predict)
"In cases of combined pulmonary fibrosis and emphysema, lung volumes may appear within normal range due to combined hyperinflation and restriction, but a markedly impaired diffusing capacity can be seen." - Fishman's Pulmonary Diseases and Disorders
Teaching Point: A near-normal TLC with markedly reduced DLCO in a smoker should raise suspicion for CPFE. The PFT "looks deceptively normal" in volumes, but DLCO unmasks the true severity.
CASE 9 - Quick Spirometry Patterns Table
| Spirometry | Obstructive (asthma) | Obstructive (COPD) | Restrictive (ILD) | Mixed | Normal |
|---|---|---|---|---|---|
| FEV₁ | ↓↓ | ↓↓↓ | N or ↓ | ↓↓ | Normal |
| FVC | N or ↓ | N or ↓ | ↓↓ | ↓↓ | Normal |
| FEV₁/FVC | <0.70 | <0.70 | >0.70-0.80 | <0.70 | >0.70 |
| TLC | N or ↑ | ↑↑ | ↓↓ | ~Normal | Normal |
| DLCO | Normal | ↓↓ (emphysema) | ↓↓ (ILD) or N (chest wall) | ↓↓↓ | Normal |
| Reversibility | ✓ Significant | ✗ Minimal | ✗ | ✗ | - |
Sources: Bailey and Love's Surgery 28E; Murray & Nadel's Respiratory Medicine
PART 3 - INTEGRATED CASES (LFT + PFT Together)
CASE 10 - The Patient with Sarcoidosis
Presentation: 34-year-old Black female with dyspnea, skin nodules, and elevated ACE level. Chest X-ray shows bilateral hilar lymphadenopathy.
LFT:
| Test | Value |
|---|---|
| ALP | 210 U/L (slightly elevated) |
| ALT/AST | Mildly elevated |
| Total Bilirubin | 1.4 mg/dL |
| Albumin | 3.7 g/dL |
PFT:
| Parameter | Value |
|---|---|
| FEV₁ | 72% predicted |
| FVC | 68% predicted |
| FEV₁/FVC | 0.79 |
| DLCO | 60% predicted (↓) |
Integration:
- PFT: Restrictive pattern with reduced DLCO = pulmonary sarcoidosis (granulomatous infiltration)
- LFT: Mildly elevated ALP = hepatic sarcoidosis (granulomas in liver, usually asymptomatic)
- Combined organ involvement is common in sarcoidosis
CASE 11 - The Patient with Alpha-1 Antitrypsin Deficiency
Presentation: 38-year-old non-smoker with early-onset emphysema and unexplained liver disease.
LFT:
| Test | Value |
|---|---|
| ALT | 95 U/L |
| AST | 80 U/L |
| ALP | 130 U/L |
| GGT | 110 U/L |
| Albumin | 3.2 g/dL |
PFT:
| Parameter | Value |
|---|---|
| FEV₁ | 52% predicted |
| FVC | 80% predicted |
| FEV₁/FVC | 0.55 |
| DLCO | 50% predicted |
| TLC | Elevated (air trapping) |
Integration:
- PFT: Obstructive pattern + low DLCO + no smoking history = should raise alpha-1 antitrypsin (A1AT) deficiency
- LFT: Hepatocellular pattern - A1AT accumulates in hepatocytes (PAS-positive globules), causing cirrhosis
- Key: Emphysema at young age + unexplained liver disease = always check serum A1AT level
Summary: Key Rules to Remember
LFT Rules:
- Unconjugated hyperbilirubinemia + normal enzymes = pre-hepatic (hemolysis) or Gilbert's
- Conjugated hyperbilirubinemia + high ALP = cholestatic/obstructive
- Conjugated + high transaminases = hepatocellular
- AST:ALT >2:1 + high GGT = alcoholic liver disease
- Low albumin + prolonged PT = impaired synthetic function (chronic/severe)
- ALP most sensitive marker for liver metastases
PFT Rules:
- FEV₁/FVC <0.70 = obstructive; check reversibility to distinguish asthma vs COPD
- FEV₁/FVC ≥0.70 + low FVC + low TLC = restrictive
- Low DLCO + obstructive = emphysema (not pure asthma)
- Low DLCO + restrictive = interstitial lung disease
- Normal DLCO + restrictive = chest wall disease or neuromuscular disease
- Near-normal volumes + markedly low DLCO in smoker = consider CPFE
Sources: Harrison's Principles of Internal Medicine 22E; Bailey and Love's Surgery 28E; Murray & Nadel's Textbook of Respiratory Medicine; Quick Compendium of Clinical Pathology 5E; Fishman's Pulmonary Diseases and Disorders
This is a shared conversation. Sign in to Orris to start your own chat.