Medical ethics
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
I now have rich content from multiple authoritative textbooks. Let me compile the comprehensive answer.
Medical Ethics: A Comprehensive Overview
Medical ethics is the branch of applied ethics that examines moral principles governing the conduct of healthcare professionals in their dealings with patients, colleagues, and society. It is distinct from medical etiquette (professional courtesy between colleagues) and from the law, though all three interact.
1. Historical Foundations
The roots of medical ethics span thousands of years:
| Milestone | Significance |
|---|---|
| Code of Hammurabi (Babylonia, ~1750 BCE) | One of the earliest documented standards for medical practitioners |
| Sushruta's Oath (~1500 BCE) | From the Sushruta Samhita; foundational ethical standards in ancient Indian surgery |
| Charaka's Oath (~200 BCE) | From the Charaka Samhita; adopted by India's NMC in 2022 for the white coat ceremony |
| Hippocratic Oath (5th century BCE) | Attributed to Hippocrates ("Father of Medicine and Medical Ethics"); established beneficence, non-maleficence, and justice |
| Thomas Percival (1803) | Coined the terms "medical ethics" and "medical jurisprudence"; wrote the first modern code of medical ethics |
| AMA Code of Ethics (1847) | Based on Percival's work; one of the first formal institutional codes |
| Declaration of Geneva (1948, WMA) | Modern restatement of the Hippocratic Oath; amended multiple times (most recently 2017) |
| International Code of Medical Ethics (1949, WMA) | Delineated duties to the sick, to colleagues, and to society |
- The Essentials of Forensic Medicine and Toxicology, 36th edition, block 1
2. The Four Principles (Beauchamp and Childress)
The dominant framework in Western medical ethics was developed by American philosophers Tom Beauchamp and James Childress in Principles of Biomedical Ethics. Their "four principles" approach (sometimes called "principlism") has become the near-universal foundation:
1. Autonomy
Respect for the individual patient's right to make their own informed decisions. It underpins:
- Informed consent - the process of ensuring a patient understands and freely agrees to treatment
- Confidentiality - protecting patient information
- Truth-telling - honesty in disclosing diagnoses and prognoses
"Every human being of adult years and sound mind has a right to determine what shall be done with his own body; and a surgeon who performs an operation without his patient's consent, commits an assault." - Justice Cardozo
- Scott-Brown's Otorhinolaryngology, block 4
Consent requires:
- A persistent sense of self with personal values
- Sufficient understanding of available choices
- Ability to reflect on options and communicate a decision
- Adequate information (what would materially affect the patient's choice)
2. Beneficence
The obligation to act in the patient's best interests and actively do good. It includes promoting health, preventing disease, and removing harm.
3. Non-Maleficence
Primum non nocere - "first, do no harm." Any intervention carries risk; the harm of action must always be weighed against the harm of inaction. This principle underlies:
- Risk-benefit analysis before procedures
- Medical futility decisions (withholding non-beneficial interventions)
4. Justice
Fairness in the distribution of healthcare resources and treatment of individuals. It encompasses:
- Distributive justice: equitable allocation of scarce resources
- Rights-based justice: respect for patient legal rights
- Procedural justice: fair processes in healthcare decisions
"The four principles of medical ethics that command wide consensus... provide an acceptable framework, although close scrutiny of many difficult dilemmas highlights limitations in these principles and apparent conflicts between them." - Emery's Elements of Medical Genetics and Genomics
3. Ethical Frameworks (Beyond Principlism)
Several other approaches are used alongside or in place of the four principles:
| Framework | Core Idea |
|---|---|
| Deontology | Actions are right or wrong regardless of consequences (rule-based duty); underlies much of professional regulatory guidance |
| Consequentialism / Utilitarianism | The rightness of an action is determined by its outcomes (greatest good for the greatest number) |
| Virtue Ethics | Focuses on the character of the practitioner - what would a virtuous person do? |
| Casuistry | Case-based reasoning; objects to abstract top-down principles, focusing on specific circumstances |
| Ethics of Care | Emphasizes empathy, compassion, and relationships; originated with Carol Gilligan |
An important note: ethics and law are related but distinct. Some actions are legal but unethical; others are ethical but illegal (e.g., assisted dying laws vary dramatically between jurisdictions). There is no direct correspondence. - Scott-Brown's Otorhinolaryngology, block 4
4. Informed Consent
Informed consent is the practical operationalization of respect for autonomy. Three components are required:
- Disclosure - The clinician provides sufficient information (diagnosis, proposed treatment, risks, benefits, alternatives)
- Capacity - The patient has decision-making capacity (ability to understand, reason, communicate a stable choice)
- Voluntariness - The decision is made free from coercion
"The doctrine of informed consent operationalizes the duty to respect autonomy; it ensures that the patient is capable..." - Kaplan & Sadock's Comprehensive Textbook of Psychiatry, block 62
Special situations:
- Patients who lack capacity: Decision-making passes to a surrogate (usually next of kin or legal guardian), guided by advance directives or substituted judgment ("what would this patient have wanted?")
- Emergencies: Implied consent when a patient cannot consent and delay would cause harm
- Minors: Parental consent required; however, mature minors may give their own consent in many jurisdictions
- Refusal of treatment: A competent adult may refuse any treatment, including life-sustaining treatment - this must be respected
5. Confidentiality
Confidentiality is a cornerstone of the therapeutic relationship, dating to the Hippocratic tradition. It means patient information shared in the clinical encounter is not disclosed without consent. Key exceptions (where disclosure may be justified) include:
- Public health duties: Notifiable/communicable diseases must be reported to health authorities
- Risk of serious harm to third parties: e.g., a patient with homicidal intent (Tarasoff principle)
- Legal requirements: Court orders, statutory duties
- Best interests: When a patient lacks capacity and disclosure serves their welfare
6. End-of-Life Ethics
This is one of the most ethically contested areas in medicine, involving tensions among all four principles:
Advance Directives
Proactive documents stating a patient's wishes if they later lose capacity. Include:
- Living will: Specifies which treatments to accept or refuse
- Do Not Resuscitate (DNR) orders: Instruction to withhold CPR
- Durable Power of Attorney for Healthcare: Names a surrogate decision-maker
Futility and Withholding Treatment
"Futility" refers to interventions unlikely to produce benefit. The AMA's Council on Ethical and Judicial Affairs states CPR may be withheld when judged futile by the treating physician, even if requested. More precise language - "non-beneficial," "low likelihood of success" - is preferred when communicating with families. - Tintinalli's Emergency Medicine, block 3
Euthanasia and Assisted Dying
A spectrum of practices with varying legal and ethical status:
| Term | Definition | Legality |
|---|---|---|
| Passive euthanasia | Withdrawing/withholding life-sustaining treatment | Legal in most jurisdictions with proper consent |
| Palliative sedation | Sedation to relieve intractable suffering at end of life | Ethically accepted; "doctrine of double effect" applies |
| Physician-assisted dying (PAD) | Physician provides means (prescription); patient acts | Legal in some jurisdictions (Netherlands, Canada, some US states) |
| Active euthanasia | Physician directly causes death | Illegal in most countries |
The doctrine of double effect holds that an action with a harmful effect (e.g., opioids that may shorten life) is ethically permissible if: the action itself is not intrinsically wrong, the agent intends good (pain relief, not death), the bad effect is not the means to the good effect, and there is proportionate reason.
7. Research Ethics
Key principles governing medical research on human subjects emerged from historical abuses:
| Document | Key Contribution |
|---|---|
| Nuremberg Code (1947) | Formulated after Nazi medical experiments; emphasized voluntary informed consent |
| Declaration of Helsinki (1964, WMA) | Governs ethical conduct of medical research; distinguishes therapeutic from non-therapeutic research; requires ethics committee review |
| Belmont Report (1979, USA) | Identified three principles: respect for persons, beneficence, justice; led to modern IRB (Institutional Review Board) system |
8. Special Ethical Domains
Confidentiality vs. Disclosure (the Tarasoff dilemma)
When a patient reveals intent to harm an identifiable third party, clinicians face a conflict between confidentiality and the duty to protect. Most jurisdictions impose a duty to warn.
Genetics and Genomics Ethics
Genetic information is unique because it is shared with biological relatives. The principle of individual autonomy may conflict with the interests (and potential for harm) of family members. Key issues include disclosure of incidental findings, predictive testing in minors, and genetic discrimination. - Emery's Elements of Medical Genetics and Genomics, block 3
Resource Allocation (Justice)
Especially relevant in intensive care and organ transplantation. Criteria for allocation must be fair, transparent, and free from bias (age, disability, social worth).
Professionalism
Medical professionalism encompasses integrity, accountability, altruism, and respect for patients. It forms the ethical backbone that links the principles above to daily clinical practice. - Kaplan & Sadock's, block 65
9. Common Ethical Dilemmas and How to Approach Them
A structured approach to ethical dilemmas:
- Gather facts - clinical details, patient values, social context
- Identify the ethical conflict - which principles are in tension?
- Assess decision-making capacity - is the patient competent?
- Consult relevant parties - patient, family, team, ethics committee
- Consider the legal framework - advance directives, relevant statutes
- Make a reasoned judgment - document reasoning clearly
- Review and learn - debrief after difficult cases
Institutional ethics committees exist to support clinicians in navigating complex cases without clear answers. They are advisory, not directive.
Key Declarations and Codes at a Glance
| Document | Year | Body | Focus |
|---|---|---|---|
| Hippocratic Oath | ~5th c. BCE | Hippocrates | Beneficence, non-maleficence, confidentiality |
| Declaration of Geneva | 1948 (updated 2017) | WMA | Modern physician oath |
| International Code of Medical Ethics | 1949 | WMA | Duties to patients, colleagues, society |
| Nuremberg Code | 1947 | International | Research consent |
| Declaration of Helsinki | 1964 | WMA | Research ethics |
| Belmont Report | 1979 | USA | Research: respect, beneficence, justice |
Sources: The Essentials of Forensic Medicine and Toxicology (36th ed.) | Emery's Elements of Medical Genetics and Genomics | Scott-Brown's Otorhinolaryngology Head & Neck Surgery | Kaplan & Sadock's Comprehensive Textbook of Psychiatry | Tintinalli's Emergency Medicine | Parikh's Textbook of Medical Jurisprudence
Medical code of ethics of mbbs students with images
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Searching the Web
NMC medical code of ethics MBBS students India Declaration of Geneva Charaka oath white coat ceremony
Reading File
Reading Web Page
NMC new physician pledge MBBS students oath code of ethics
Generating Image
Generating Image
?
Generating Image
Generating Image
Retry
Generating Image
Generating Image
Generating Image
Here is the complete guide to the Medical Code of Ethics for MBBS Students, with images:
Medical Code of Ethics for MBBS Students
1. Historical Evolution of Medical Ethics Oaths
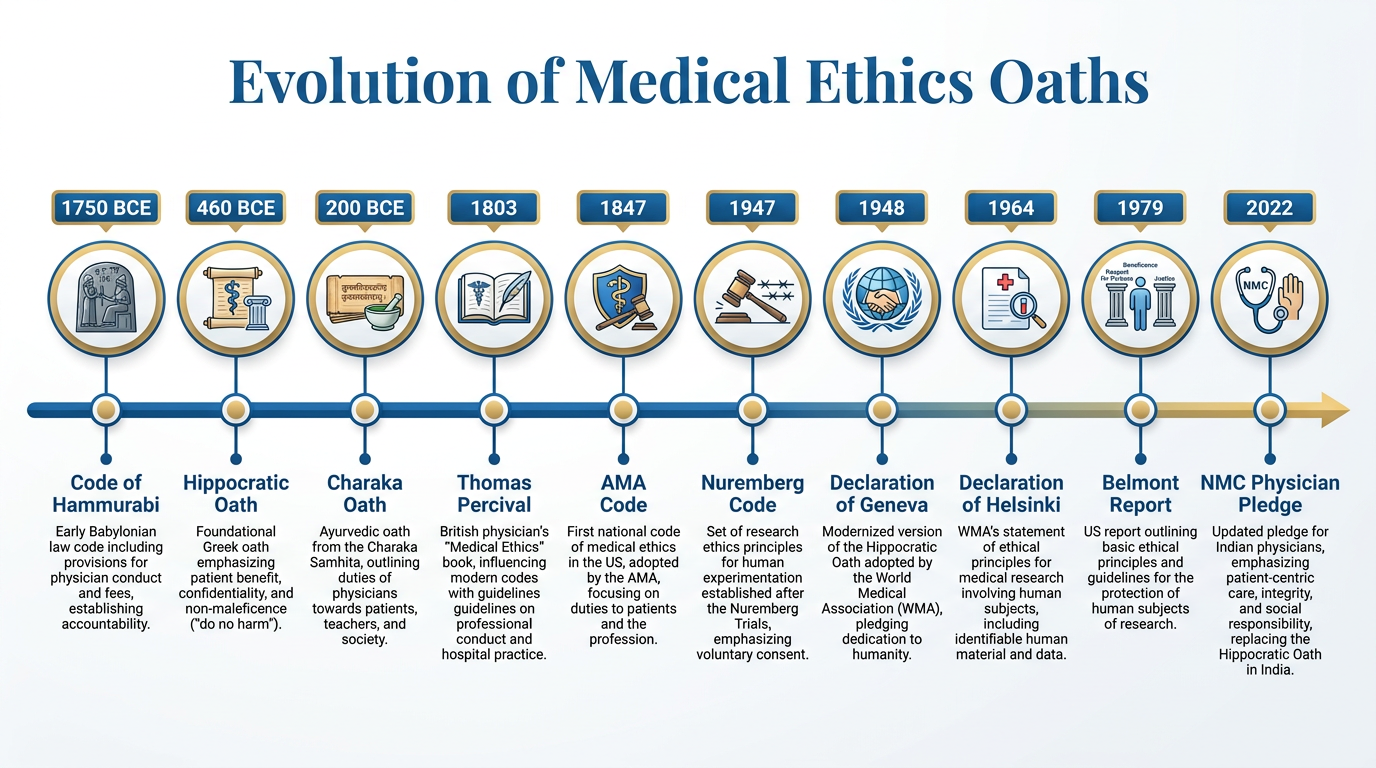
| Milestone | Year | Significance |
|---|---|---|
| Code of Hammurabi | ~1750 BCE | Earliest documented medical practitioner standards (Babylonia) |
| Sushruta's Oath | ~1500 BCE | Sushruta Samhita - Father of Indian Surgery |
| Charaka's Oath | ~200 BCE | Charaka Samhita - Father of Indian Medicine; adopted by NMC in 2022 for white coat ceremony |
| Hippocratic Oath | 5th century BCE | Foundation of Western medical ethics (beneficence, non-maleficence, confidentiality) |
| Thomas Percival | 1803 | Coined "medical ethics" and "medical jurisprudence"; wrote the first modern code |
| AMA Code of Ethics | 1847 | First institutional code; based on Percival's work |
| Nuremberg Code | 1947 | Research ethics; voluntary informed consent after Nazi experiments |
| Declaration of Geneva | 1948 (updated 2017) | Modern Hippocratic Oath; issued by the World Medical Association |
| Declaration of Helsinki | 1964 | Ethical principles for human experimentation |
| Belmont Report | 1979 | Research ethics: respect for persons, beneficence, justice |
| NMC Physician's Pledge | 2022 | Replaced Charaka Shapath and Hippocratic Oath for Indian MBBS students |
- The Essentials of Forensic Medicine and Toxicology, 36th edition
2. The Four Core Principles of Medical Ethics
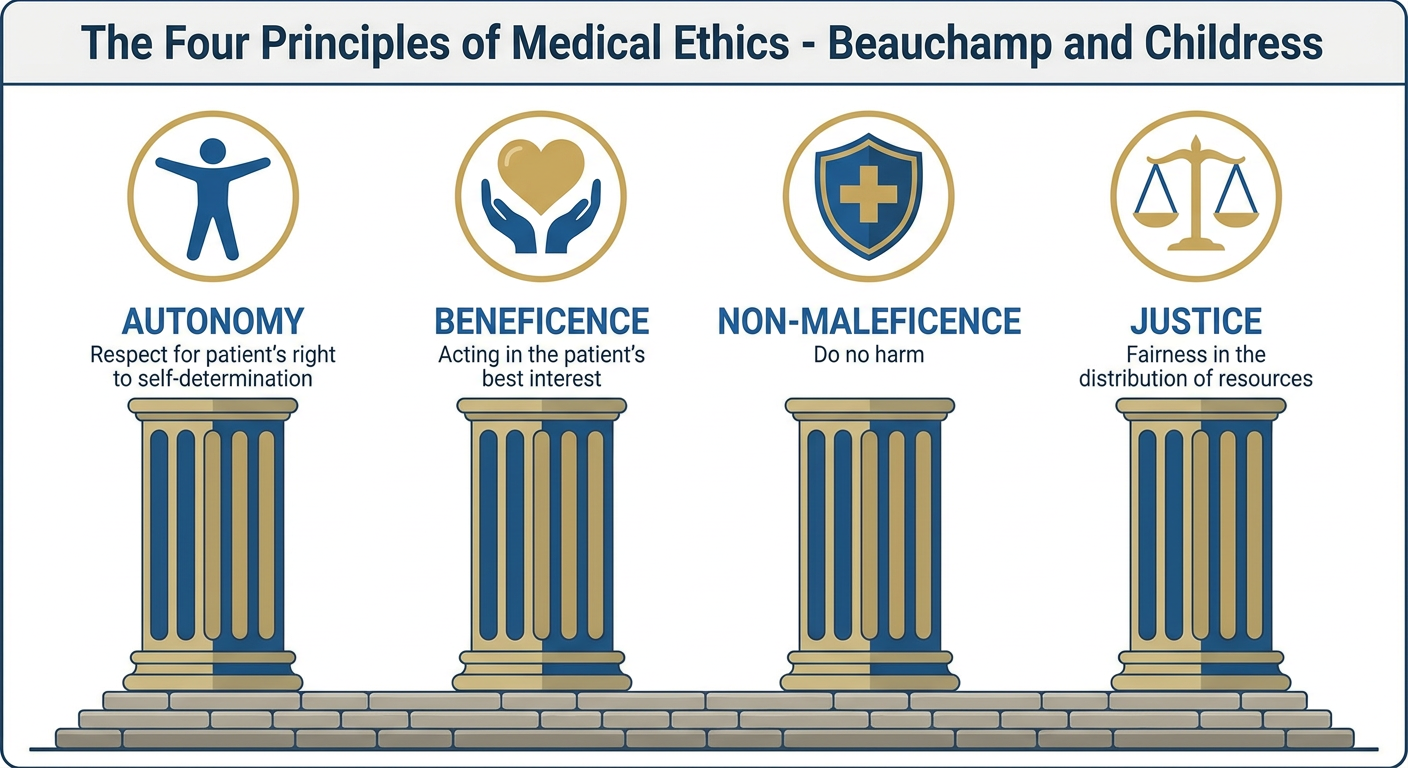
Developed by Tom Beauchamp and James Childress (Principles of Biomedical Ethics), these four principles form the universal framework:
🔵 1. Autonomy
- Respect for the patient's right to make their own decisions
- Requires informed consent: disclosure + understanding + voluntary choice
- Covers confidentiality, truth-telling, and the right to refuse treatment
- Decisional capacity must be assessed - if lacking, a surrogate decides
🟢 2. Beneficence
- Act in the patient's best interest and actively do good
- Promote health, prevent disease, relieve suffering
- Underpins clinical duty of care
🔴 3. Non-Maleficence
- Primum non nocere - "first, do no harm"
- Every intervention carries risk; harm of action must be weighed against harm of inaction
- Basis for medical futility decisions and risk-benefit analysis
🟡 4. Justice
- Fairness in treatment and resource distribution
- Includes distributive justice (fair allocation of resources), patient rights, and non-discrimination
- No patient may be denied care on grounds of race, religion, gender, nationality, or social status
3. The Hippocratic Oath (Full Text)
The oldest and most revered code, still taught to MBBS students:
"I will prescribe regimen for the good of my patients according to my ability and my judgment and never do harm to anyone. To please no one will I prescribe a deadly drug, nor give advice which may cause his death... In every house where I come I will enter only for the good of my patients, keeping myself far from all intentional ill-doing... All that may come to my knowledge in the exercise of my profession... I will keep secret and will never reveal. If I keep this oath faithfully, may I enjoy my life and practice my art, respected by all men and in all times."
- P.C. Dikshit Textbook of Forensic Medicine and Toxicology
4. The Declaration of Geneva (1948, Updated 2017)
The modern physician's oath, administered to MBBS students at admission/graduation:
"AS A MEMBER OF THE MEDICAL PROFESSION:
- I SOLEMNLY PLEDGE to dedicate my life to the service of humanity
- THE HEALTH AND WELL-BEING OF MY PATIENT will be my first consideration
- I WILL RESPECT the autonomy and dignity of my patient
- I WILL MAINTAIN the utmost respect for human life
- I WILL NOT PERMIT considerations of age, disease or disability, creed, ethnic origin, gender, nationality, political affiliation, race, sexual orientation, or social standing to intervene between my duty and my patient
- I WILL RESPECT the secrets that are confided in me, even after the patient has died
- I WILL PRACTISE my profession with conscience and dignity and in accordance with good medical practice
- I WILL FOSTER the honour and noble traditions of the medical profession
- I WILL GIVE to my teachers, colleagues, and students the respect and gratitude that is their due
- I WILL SHARE my medical knowledge for the benefit of the patient and the advancement of healthcare
- I WILL ATTEND TO my own health, well-being, and abilities in order to provide care of the highest standard
- I WILL NOT USE my medical knowledge to violate human rights and civil liberties, even under threat
- I MAKE THESE PROMISES solemnly, freely, and upon my honour."**
This is the oath now included in the NMC Draft RMP Regulations as "The Physician's Pledge," replacing both the Hippocratic Oath and the Charaka Shapath for Indian MBBS students. - Medical Dialogues
5. Professional Misconduct - What MBBS Students Must Avoid
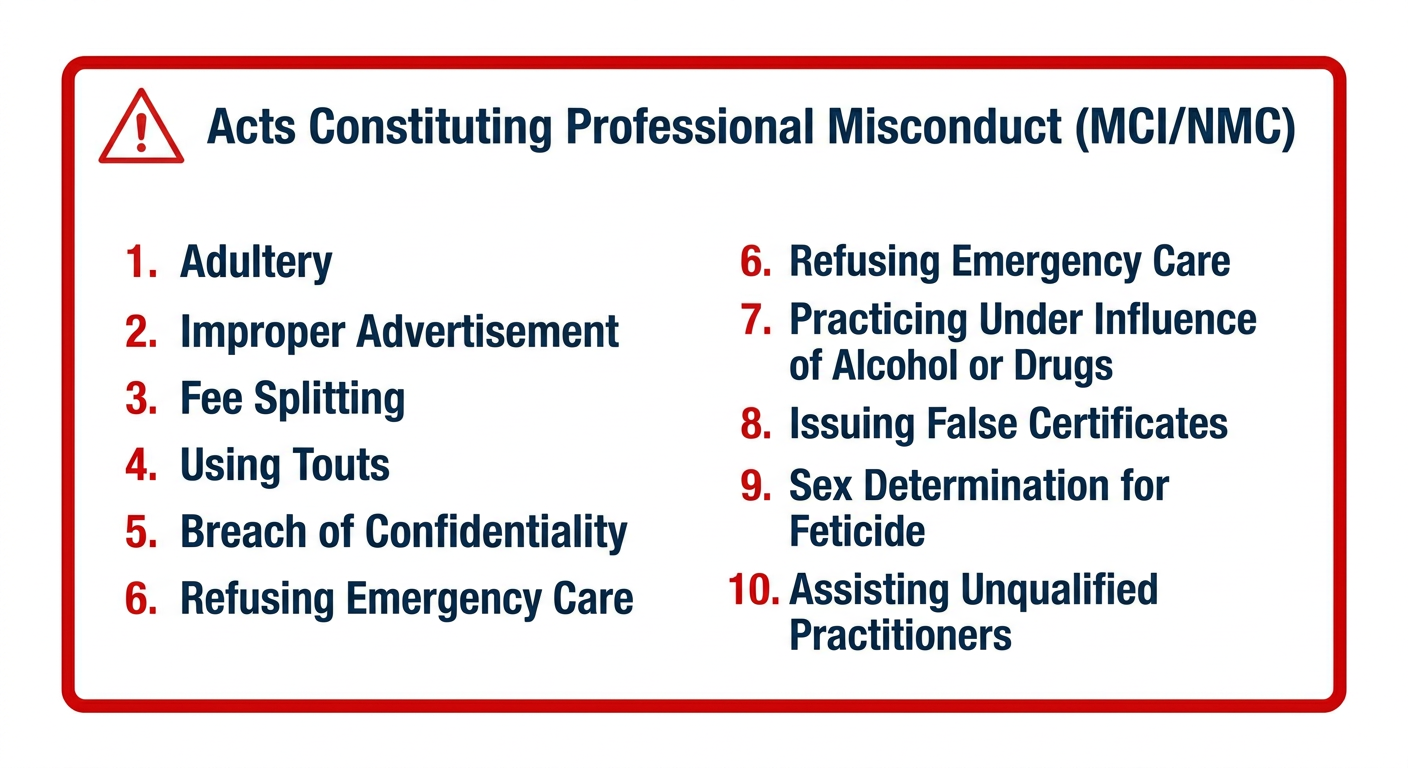
The MCI/NMC Code of Medical Ethics lists acts that constitute professional misconduct. Violation leads to disciplinary action including erasure from the medical register:
| # | Prohibited Act |
|---|---|
| 1 | Adultery - sexual relations with a patient |
| 2 | Improper advertisement - unusual signboards, self-promotion through pharmaceutical firms |
| 3 | Fee splitting / dichotomy - receiving or giving commissions from colleagues or drug manufacturers |
| 4 | Using touts and agents to fetch patients |
| 5 | Breach of confidentiality - disclosing patient secrets without consent |
| 6 | Refusal to treat on religious grounds |
| 7 | Practicing under influence of alcohol or addictive drugs |
| 8 | Issuing false certificates (for insurance, passport, sick benefits, etc.) |
| 9 | Sex determination tests with intent to destroy the female fetus |
| 10 | Assisting unqualified practitioners |
| 11 | Not reporting notifiable diseases to health authorities |
| 12 | Association with pharmaceutical firms (ownership, rebates) |
- P.C. Dikshit Textbook of Forensic Medicine and Toxicology
6. IMC Regulations 2002 - Key Salient Points (Now Under NMC)
These regulations are binding on all registered doctors in India:
- Doctors may choose their patients but must not refuse emergency care
- Refer only when absolutely necessary; avoid unnecessary investigations
- Once a case is accepted, the patient must not be abandoned without notice
- Fees and charges must be displayed clearly
- No endorsement of medications or equipment for financial gain
- Prescribe drugs by generic name as far as possible
- No sex determination tests for feticide
- Patients must not be subjected to trials except under ICMR guidelines
- Maintain patient records for a minimum of 3 years for inpatients
7. Key WMA Declarations Every MBBS Student Should Know
| Declaration | Year | Topic |
|---|---|---|
| Declaration of Geneva | 1948 (2017) | Modern physician oath |
| Declaration of Helsinki | 1964 | Human experimentation ethics |
| Declaration of Sydney | 1968 | Death certification and organ harvesting |
| Declaration of Oslo | 1970 | Therapeutic abortion |
| Declaration of Tokyo | 1975 | Prohibition of torture |
| Declaration of Lisbon | 1981 | Rights of patients |
| Declaration of Madrid | 1983 | Euthanasia is unethical |
| Declaration of Malta | 1991 | Management of hunger strikers |
- The Essentials of Forensic Medicine and Toxicology, 36th edition
8. Informed Consent - A Core Duty
Informed consent is the practical application of autonomy. Three components are required:
| Component | What it means |
|---|---|
| Disclosure | Patient receives full information about diagnosis, treatment, risks, benefits, alternatives |
| Capacity | Patient can understand, reason, and communicate a stable decision |
| Voluntariness | Decision is free from coercion or undue influence |
Special situations:
- Emergencies - implied consent applies when delay would be harmful
- Minors - parental/guardian consent required; mature minors may consent in some jurisdictions
- Unconscious patients - surrogate/next-of-kin decides; advance directives are honored
- Refusal of treatment - a competent adult has the absolute right to refuse, even life-saving treatment
9. Quick Memory Aid for MBBS Exams
B - Beneficence → Do Good
N - Non-maleficence → Do No Harm
A - Autonomy → Respect Patient's Choice
J - Justice → Be Fair to All
"BNAJ" or remember as the "4 pillars" of bioethics - every clinical decision should be tested against all four.
Sources: P.C. Dikshit Textbook of Forensic Medicine and Toxicology | The Essentials of Forensic Medicine and Toxicology (36th ed., 2026) | Parikh's Textbook of Medical Jurisprudence | Emery's Elements of Medical Genetics | NMC Draft RMP Regulations (2022)
Genrate same for all medical health care professionals like ahs
Finding Sources
Finding Sources
Searching the Web
code of ethics allied health professionals AHS nursing pharmacy physiotherapy dentistry India WHO 2024
Reading Web Page
code of ethics allied health professionals duties obligations conduct
Finding Sources
Finding Sources
Searching the Web
NCAHP India RAHP professional conduct ethics regulations 2026 allied health professions code duties
Finding Sources
Generating Image
Generating Image
Genrate same for all medical health care professionals like ahs
Generating Image
Generating Image
Generating Image
This is a shared conversation. Sign in to Orris to start your own chat.