Valproate with reference from standard psychiatry book
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have enough comprehensive content from multiple standard psychiatry textbooks. Let me compile the full response.
Valproate (Valproic Acid / Sodium Valproate)
Sources: Kaplan and Sadock's Synopsis of Psychiatry (11th ed.), Stahl's Essential Psychopharmacology (5th ed.), The Maudsley Prescribing Guidelines in Psychiatry (15th ed.)
1. Chemistry and Formulations
Valproate is a simple branched-chain carboxylic acid. It is called valproic acid because it is rapidly converted to the acid form in the stomach. At physiologic pH, valproic acid dissociates into the valproate ion, which is the therapeutically active moiety.
Available formulations (Kaplan & Sadock's Synopsis):
| Formulation | Brand | Notes |
|---|---|---|
| Valproic acid | Depakene | More GI side effects |
| Divalproex sodium | Depakote | Enteric-coated, 1:1 mixture; delayed-release; available as sprinkle capsules |
| Sodium valproate injection | Depacon | IV use |
| Extended-release (CR) | Epilim Chrono | Once-daily dosing possible |
All formulations are therapeutically equivalent as they all yield the same valproate ion.
2. Mechanism of Action
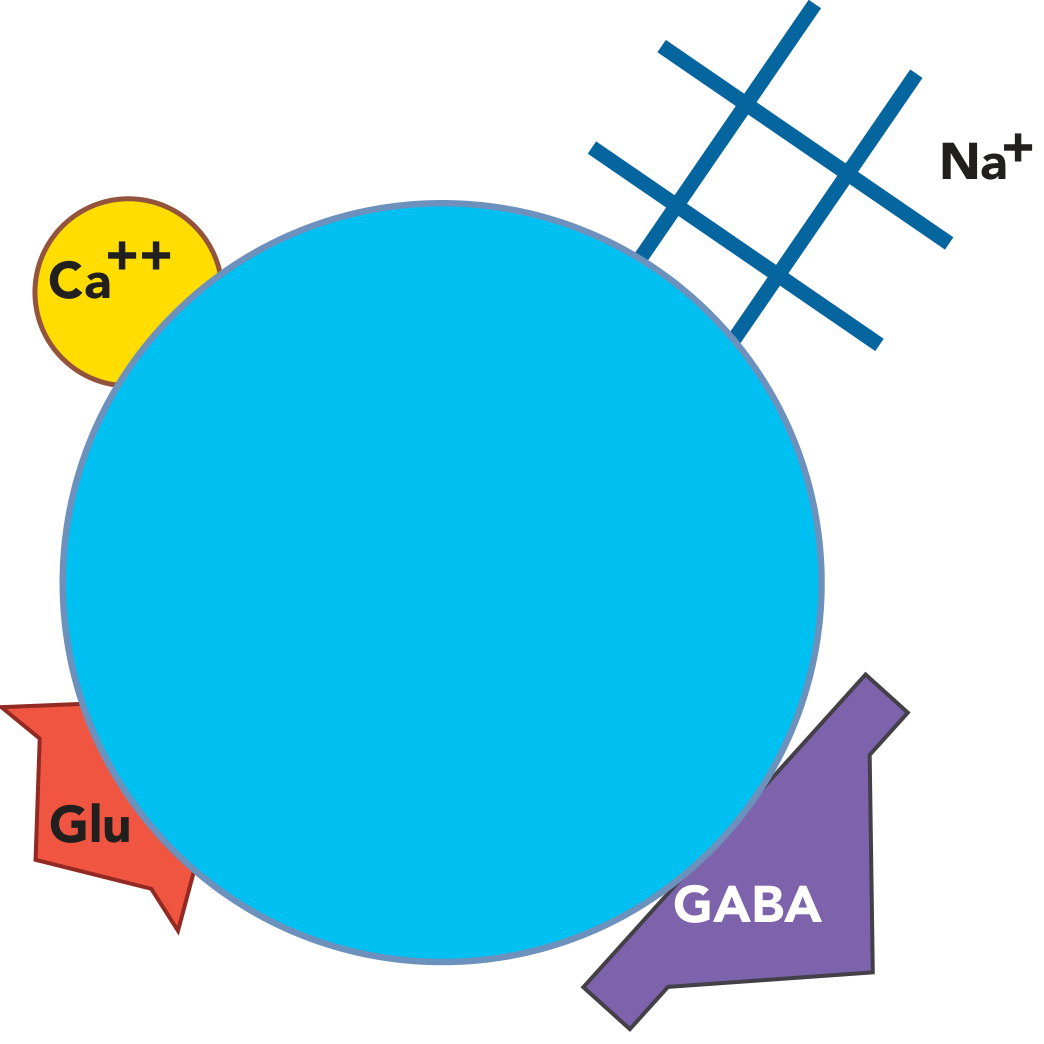
The exact mechanism is uncertain and likely multi-modal. Three main hypotheses are recognized (Stahl's):
-
Inhibition of voltage-sensitive sodium channels (VSSCs): Valproate may change the sensitivity of VSSCs, possibly by directly binding to channel subunits or inhibiting phosphorylating enzymes that regulate their sensitivity. This reduces sodium influx and downstream glutamate excitatory neurotransmission - a possible mechanism for antimanic effects.
-
Potentiation of GABAergic neurotransmission: Valproate inhibits the catabolism of GABA, thereby increasing GABAergic inhibition.
-
Downstream signal transduction regulation (Maudsley): Valproate reduces protein kinase C, activates the extracellular signal-regulated kinase (ERK) pathway, promotes BDNF (brain-derived neurotrophic factor) expression, reduces turnover of arachidonic acid, and alters synaptic plasticity. It also depletes inositol and influences non-GABA pathways.
It is not known which of these actions specifically explains mood stabilization vs. anticonvulsant vs. anti-migraine effects.
3. Indications (Psychiatric)
A. Mania / Bipolar I Disorder - Acute Mania
- Approved for manic episodes associated with Bipolar I Disorder (Kaplan & Sadock's).
- About two-thirds of patients with acute mania respond to valproate.
- Response usually within 1-4 days after achieving serum concentrations above 50 µg/mL.
- Optimal therapeutic range: 50-125 µg/mL for antimanic response; levels >94 mg/L associated with the most robust response (Maudsley).
- Rapid oral loading strategies can achieve therapeutic serum concentrations in 1 day and control manic symptoms within 5 days.
- NNT = 2-4 for acute mania (Maudsley).
- The irritable manic subtype responds significantly better to valproate than lithium or placebo (Kaplan & Sadock's).
- Preferred over lithium for acute mania in children and elderly due to more favorable cognitive, dermatologic, thyroid, and renal adverse effect profile.
B. Bipolar Depression
- Valproate has some activity in bipolar depressive episodes, but far less pronounced than for mania.
- More useful for agitation than dysphoria within depressive episodes.
- A 2020 meta-analysis placed divalproex 5th out of 21 treatments for bipolar depression (Maudsley).
- In clinical practice, most often used as add-on therapy to an antidepressant to prevent mania or rapid cycling.
C. Prophylaxis (Maintenance)
- Useful in prophylaxis of Bipolar I disorder - fewer, less severe, shorter manic episodes.
- At least as effective as lithium in prophylaxis and better tolerated (Kaplan & Sadock's).
- Particularly useful in:
- Rapid-cycling and ultrarapid-cycling bipolar disorders
- Dysphoric or mixed mania
- Mania due to a general medical condition
- Comorbid substance use disorders or panic attacks
- Incomplete response to lithium
- NICE (UK) recommends valproate as a first-line option for acute mania, bipolar depression (with antidepressant), and prophylaxis - but NOT in women of child-bearing potential (Maudsley).
- A Cochrane review noted that evidence supporting prophylactic use is limited.
D. Other Psychiatric Uses
- Schizophrenia/Schizoaffective disorder: May accelerate response to antipsychotic therapy; not effective alone for psychotic symptoms (Kaplan & Sadock's).
- Aggression/Behavioral agitation: Some evidence for reduction of aggressive behavior in various psychiatric conditions; one RCT failed to show advantage over risperidone alone in schizophrenia (Maudsley).
- Studied (weak evidence) in: alcohol withdrawal, panic disorder, PTSD, impulse control disorder, borderline personality disorder (Kaplan & Sadock's).
4. Pharmacokinetics
- Pharmacokinetics are complex, following a three-compartmental model with protein-binding saturation (Maudsley).
- Highly protein-bound (~90-95%); can be displaced by other protein-bound drugs (e.g., aspirin).
- Hepatically metabolized - primarily by glucuronide conjugation and beta-oxidation; CYP enzymes play a minor role.
- Plasma half-life: approximately 9-16 hours (varies by formulation and age).
- Therapeutic range: 50-125 µg/mL (trough, 12 hours post-dose).
- Serum levels <55 mg/L are no more effective than placebo in acute mania (Maudsley).
5. Dosing
- Start low and titrate upwards against response and adverse effects.
- Loading dose regimens (e.g., 20-30 mg/kg/day) are generally well tolerated and achieve therapeutic levels rapidly.
- Controlled-release sodium valproate (Epilim Chrono) can be given once daily; other formulations require at least twice daily dosing.
- Typical maintenance doses: 750-2,000 mg/day in divided doses.
Pre-treatment work-up (Maudsley Table 2.3):
- Full blood count (FBC) and liver function tests (LFTs)
- Baseline weight measurement
- In women: pregnancy test + contraception counseling
On-treatment monitoring:
- LFTs and FBC at 6 months; BMI monitoring
- More frequent LFTs during the first 6 months; albumin and clotting if enzyme levels are abnormal
- Plasma level monitoring: useful to detect non-compliance or toxicity
6. Adverse Effects
Serious / Black Box Warnings (Kaplan & Sadock's)
| Organ | Effect |
|---|---|
| Liver | Fatal hepatotoxicity (risk highest in children <3 years + polypharmacy; rate 0.85/100,000 in adults on monotherapy) |
| Pancreas | Pancreatitis (rare, usually within first 6 months; can be fatal) |
| Hematologic | Thrombocytopenia, platelet dysfunction (especially at high doses; prolongs bleeding time); more likely at levels ≥110 µg/mL (women), ≥135 µg/mL (men) |
| Teratogenicity | Neural tube defects (1-4%), cardiac malformations; cognitive impairment in child exposed in utero; increased autism risk |
Common Adverse Effects
| System | Effects |
|---|---|
| GI | Nausea, vomiting, dyspepsia, diarrhea - most common in first month; improved with enteric-coated formulations |
| Neurological | Sedation, ataxia, dysarthria, tremor (dose-related; up to 25% of patients; may respond to beta-blockers or gabapentin) |
| Weight | Weight gain - common in long-term use; exacerbated by co-prescription of clozapine or olanzapine |
| Hair | Hair loss / alopecia in 5-10%; rare complete loss; may respond to zinc/selenium supplements |
| Liver enzymes | Mild transaminase elevation (5-40% of patients) - usually asymptomatic and reversible |
| Metabolic | Hyperammonemia (can cause encephalopathy); polycystic ovarian syndrome (PCOS) in young women; menstrual irregularities, hirsutism, insulin resistance |
| CNS | Cognitive decline occasionally with parkinsonism; hyperammonemia-induced encephalopathy |
7. Teratogenicity and Use in Women
- Established human teratogen (Maudsley) - contraindicated in women of child-bearing potential in many countries.
- Neural tube defects (e.g., spina bifida): ~1-4% risk in first trimester; risk reduced with folic acid 1-4 mg/day.
- Cognitive effects in offspring: Lower IQ at age 6 years; dose-dependent reduction in cognitive abilities across multiple domains.
- Autism spectrum disorder: Increased risk with in utero exposure.
- Folic acid supplementation is mandatory in all women of child-bearing potential on valproate.
- PCOS: Reported particularly in adolescents and young women; driven by metabolic syndrome/insulin resistance.
- Breastfeeding: Infant serum levels reach 1-10% of maternal; not contraindicated but caution advised.
8. Drug Interactions
| Interaction | Mechanism | Effect |
|---|---|---|
| Aspirin | Displaces valproate from protein binding + inhibits metabolism | Increased free valproate - toxicity |
| Lamotrigine | Valproate inhibits glucuronidation | 2x increase in lamotrigine levels - toxicity risk |
| TCAs (esp. clomipramine) | Valproate inhibits glucuronidation | Raised TCA levels |
| Quetiapine | Inhibits glucuronidation | Raised quetiapine levels |
| Phenobarbital | Inhibits glucuronidation | Raised phenobarbital levels |
| Warfarin | Displaces warfarin from protein binding | Higher free warfarin - bleeding risk |
| Olanzapine | Mechanism unknown | Significantly lowers olanzapine levels |
| Erythromycin, fluoxetine, cimetidine | Inhibit CYP enzymes | Increased valproate levels |
| Antipsychotics | Pharmacodynamic antagonism | Antagonise anticonvulsant effect (seizure threshold lowering) |
9. Contraindications
- Hepatic disease or severe hepatic impairment
- Personal or family history of severe hepatic dysfunction
- Women of child-bearing potential (UK/EU regulatory guidance)
- Known hypersensitivity to valproate
- Mitochondrial disorders (e.g., Alpers' syndrome) - especially in children
10. Discontinuation
- If discontinuing, taper slowly over at least 1 month (preferably longer) to avoid precipitating mood episodes (Maudsley).
- Limited data on whether abrupt discontinuation worsens the natural course of bipolar illness as markedly as with lithium, but caution is warranted.
- In epilepsy, withdrawal of valproate is associated with depression, falls, and hospital admissions.
Summary: Valproate at a Glance
| Feature | Detail |
|---|---|
| Class | Branched-chain fatty acid / Mood stabilizer / Anticonvulsant |
| Primary psychiatric indication | Bipolar I disorder (mania, prophylaxis) |
| Therapeutic range | 50-125 µg/mL |
| Dosing | 750-2,000 mg/day (divided doses); CR formulation once daily |
| Key monitoring | LFTs, FBC, weight, plasma levels |
| Main risks | Hepatotoxicity, teratogenicity, pancreatitis, thrombocytopenia, weight gain, PCOS |
| Contraindicated in | Liver disease, women of child-bearing potential |
| Key interactions | Lamotrigine (raise levels), aspirin (raises valproate), olanzapine (lowers olanzapine) |
References:
- Kaplan and Sadock's Synopsis of Psychiatry (11th ed.), Chapter 21, pp. 1979-1990
- Stahl's Essential Psychopharmacology (5th ed., Neuroscientific Basis), Chapter 7, pp. 363-370
- The Maudsley Prescribing Guidelines in Psychiatry (15th ed.), Chapter 2 (Valproate), pp. 314-316
20 marks answer for valproate with reference from standard psychiatry book
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
I now have everything needed to write a comprehensive, well-structured 20-mark exam answer. Let me compose it.
VALPROATE
20-Mark Answer
References: Kaplan and Sadock's Synopsis of Psychiatry (11th ed.) | Stahl's Essential Psychopharmacology (5th ed.) | The Maudsley Prescribing Guidelines in Psychiatry (15th ed.)
I. INTRODUCTION
Valproate (valproic acid / sodium valproate / divalproex sodium) is a simple branched-chain fatty acid and one of the most widely prescribed mood stabilizers in psychiatry. It is approved for the treatment of manic episodes associated with Bipolar I Disorder, has a rapid onset of action, and is generally well-tolerated. Numerous studies demonstrate that it reduces the frequency and intensity of recurrent manic episodes over extended periods.
(Kaplan & Sadock's Synopsis of Psychiatry, p. 1979)
II. CHEMISTRY AND FORMULATIONS
Valproate is a simple-chain carboxylic acid. It is called "valproic acid" because it is rapidly converted to the acid form in the stomach. At physiologic pH, it dissociates into the valproate ion, which is the therapeutically active moiety common to all formulations.
| Formulation | Brand Name | Notes |
|---|---|---|
| Valproic acid | Depakene | Higher GI side effects |
| Divalproex sodium | Depakote | Enteric-coated, delayed-release; 1:1 mixture; sprinkle capsules available |
| Sodium valproate injection | Depacon | IV use |
| Controlled-release (CR) | Epilim Chrono | Once-daily dosing possible |
All preparations are therapeutically equivalent.
(Kaplan & Sadock's Synopsis, p. 1979; Maudsley, p. 313)
III. MECHANISM OF ACTION
The mechanism is complex and not fully understood. At least three major mechanisms are proposed (Stahl's Essential Psychopharmacology, p. 363):
A. Inhibition of Voltage-Sensitive Sodium Channels (VSSCs)
Valproate may change the sensitivity of VSSCs, either by directly binding to channel subunits or by inhibiting phosphorylating enzymes that regulate channel sensitivity. This reduces sodium influx and downstream glutamate excitatory neurotransmission, a possible mechanism for antimanic effects.
B. Potentiation of GABAergic Neurotransmission
Valproate inhibits the catabolism of GABA (gamma-aminobutyric acid), thereby increasing GABAergic inhibitory tone in the brain. It may also enhance GABA synthesis and reduce GABA turnover.
C. Downstream Signal Transduction Regulation
Valproate:
- Activates the ERK (extracellular signal-regulated kinase) pathway, altering synaptic plasticity
- Promotes BDNF (brain-derived neurotrophic factor) expression
- Reduces protein kinase C levels
- Reduces turnover of arachidonic acid
- Interferes with intracellular signaling and gene expression (transcription regulation, cytoskeletal modifications, ion homeostasis)
- Depletes inositol (similar to lithium)
- May also interact with voltage-sensitive calcium channels and indirectly reduce glutamate activity
(Maudsley Prescribing Guidelines, p. 313; Stahl's, p. 363-366)
IV. PHARMACOKINETICS
- Pharmacokinetics follow a three-compartmental model with protein-binding saturation (Maudsley, p. 315)
- Highly protein-bound (~90-95%); can be displaced by other protein-bound drugs (e.g., aspirin, warfarin)
- Hepatically metabolized - primarily via glucuronide conjugation and beta-oxidation; CYP enzymes play a minor role
- Half-life: approximately 9-16 hours (varies by formulation and age)
- Bioavailability: nearly 100% on oral administration
- Therapeutic plasma range: 50-125 µg/mL (trough level, drawn 12 hours post-dose)
- Levels <55 mg/L are no more effective than placebo in acute mania
- Levels >94 mg/L are associated with the most robust antimanic response
- Maintenance phase optimal levels: likely ≥50 mg/L
- Total (rather than free) valproate concentration is the standard monitoring method and is adequate in most situations
(Maudsley Prescribing Guidelines, p. 315)
V. INDICATIONS AND CLINICAL USE
A. Bipolar I Disorder - Acute Mania (PRIMARY INDICATION)
- About two-thirds of patients with acute mania respond to valproate (Kaplan & Sadock's, p. 1984)
- Response usually occurs within 1-4 days after achieving serum concentrations >50 µg/mL
- Rapid oral loading strategies achieve therapeutic levels in 1 day, controlling mania within 5 days
- NNT = 2-4 for acute mania (Maudsley, p. 314)
- Antimanic effects can be augmented with lithium, carbamazepine, second-generation antipsychotics (SGAs), or dopamine receptor antagonists (DRAs)
- The irritable manic subtype responds significantly better to valproate than to lithium or placebo
- Preferred over lithium in children and elderly due to more favorable cognitive, dermatologic, thyroid, and renal adverse effect profile
B. Bipolar Depression
- Has some short-term efficacy in bipolar depressive episodes, but far less pronounced than for mania (Kaplan & Sadock's, p. 1984)
- More useful for agitation than dysphoria
- A 2020 meta-analysis placed divalproex 5th out of 21 treatments for bipolar depression
- Commonly used as add-on therapy to an antidepressant to prevent switch to mania or rapid cycling
C. Prophylaxis (Maintenance Therapy)
- Results in fewer, less severe, shorter manic episodes (Kaplan & Sadock's, p. 1984)
- At least as effective as lithium and better tolerated in prophylaxis
- Particularly useful in:
- Rapid-cycling and ultrarapid-cycling bipolar disorder
- Dysphoric or mixed mania
- Mania secondary to a general medical condition
- Comorbid substance use disorders or panic disorder
- Incomplete response to lithium
- NICE (UK) recommends valproate as a first-line option for mania, bipolar depression, and prophylaxis - but NOT in women of child-bearing potential (Maudsley, p. 314)
- BALANCE study found lithium numerically superior to valproate alone; the combination of lithium + valproate was statistically superior to valproate alone
D. Schizophrenia and Schizoaffective Disorder
- May accelerate response to antipsychotic therapy
- Not effective alone for psychotic symptoms; typically used in combination (Kaplan & Sadock's, p. 1984)
E. Other Psychiatric Uses (Weak Evidence)
- Alcohol withdrawal and relapse prevention
- Panic disorder
- PTSD
- Impulse control disorder
- Borderline personality disorder
- Behavioral agitation in dementia (one Cochrane review found it ineffective and associated with higher adverse effects)
- Aggression in various psychiatric disorders
(Kaplan & Sadock's Synopsis, p. 1984-1985)
VI. DOSING AND MONITORING
Dosing
| Phase | Dose | Notes |
|---|---|---|
| Starting dose | 250 mg TDS or 500 mg BD | Titrate against response and side effects |
| Therapeutic range | 750-2,000 mg/day | Divided doses |
| Loading dose | 20-30 mg/kg/day | For rapid control of acute mania; generally well tolerated |
| CR preparation | Once daily | Produces lower peak plasma levels; better tolerated |
Pre-treatment Work-up (NICE/Maudsley, p. 315-316)
- Full blood count (FBC)
- Liver function tests (LFTs)
- Baseline weight / BMI
- In women: pregnancy test + contraception counseling + folic acid prescription
On-treatment Monitoring
- LFTs and FBC repeated at 6 months; more frequently in first 6 months if enzyme levels are elevated
- Albumin and clotting measured if LFT abnormality persists
- BMI monitored throughout
- Plasma levels for compliance check, toxicity detection, or dose optimization
- Free valproate levels indicated when significant hypoalbuminaemia is present
VII. ADVERSE EFFECTS
(Kaplan & Sadock's Table 21-33, p. 1988-1990; Maudsley, p. 315)
Common
| System | Effect |
|---|---|
| GI | Nausea, vomiting, dyspepsia, diarrhea - most frequent in first month; reduced with enteric-coated formulations |
| Neurological | Sedation, ataxia, dysarthria, tremor (dose-related; up to 25% of patients; typically intention/postural; may respond to beta-blockers or gabapentin) |
| Weight | Weight gain - especially in long-term use; worsened by co-prescription with clozapine or olanzapine |
| Hair | Alopecia (5-10% of patients); rare complete loss; may respond to zinc and selenium supplements; curly regrowth is characteristic |
Uncommon
- Persistent elevation of hepatic transaminases (5-40%; usually asymptomatic, reversible)
- Hyperammonaemia (can cause encephalopathy, confusion, lethargy)
- Peripheral oedema
Serious / Black Box Warnings
| Complication | Details |
|---|---|
| Fatal hepatotoxicity | Rate = 0.85/100,000 on monotherapy; risk highest in children <3 years, polypharmacy, inborn errors of metabolism; no deaths in adults >10 years on monotherapy reported |
| Pancreatitis | Rare; usually in first 6 months; can be fatal; monitor serum amylase |
| Thrombocytopenia | Platelet dysfunction; prolonged bleeding times; more likely at levels ≥110 µg/mL (women), ≥135 µg/mL (men) |
| Teratogenicity | Neural tube defects (1-4%), cardiac malformations; cognitive impairment in child; increased autism risk |
| Polycystic Ovarian Syndrome (PCOS) | Particularly in adolescents and young women; driven by insulin resistance and hyperinsulinemia; menstrual irregularities, hirsutism, hyperandrogenism |
| Encephalopathy / coma | Rare; associated with hyperammonaemia |
| Suicidal behaviour | Associated risk; not consistent across studies; higher in those with comorbid depression |
VIII. TERATOGENICITY AND USE IN WOMEN
Valproate is an established human teratogen and is now contraindicated in women of child-bearing potential in the UK, EU, and many other countries (Maudsley, p. 316).
- Neural tube defects (e.g., spina bifida): 1-4% risk with first-trimester exposure
- Cognitive effects in offspring: Children exposed in utero have lower IQ scores at age 6 years; dose-dependent reduction across multiple cognitive domains
- Autism spectrum disorder: Increased risk with prenatal valproate exposure
- PCOS in young women on long-term therapy
- Folic acid 1-4 mg/day must be prescribed to all women of child-bearing potential
- Breastfeeding: Infant serum levels reach 1-10% of maternal concentration; not absolutely contraindicated but caution advised
(Kaplan & Sadock's Synopsis, p. 1987-1988)
IX. DRUG INTERACTIONS
(Kaplan & Sadock's Synopsis, p. 1990; Maudsley, p. 315)
| Drug | Mechanism | Effect |
|---|---|---|
| Lamotrigine | Valproate inhibits glucuronidation | Doubles lamotrigine levels; increases risk of Stevens-Johnson syndrome and toxic epidermal necrolysis |
| Aspirin | Displaces valproate from protein binding + inhibits metabolism | Increased free valproate - toxicity |
| Warfarin | Valproate displaces warfarin from protein binding | Raised free warfarin - bleeding risk |
| TCAs (clomipramine, amitriptyline, nortriptyline) | Inhibits glucuronidation | Raised TCA plasma levels |
| Quetiapine | Inhibits glucuronidation | Raised quetiapine levels |
| Phenobarbital | Inhibits glucuronidation | Raised phenobarbital levels; increased sedation |
| Olanzapine | Mechanism unknown | Significantly lowers olanzapine concentrations |
| Carbamazepine | Induces CYP enzymes | Lowers valproate levels |
| Fluoxetine, erythromycin, cimetidine | Inhibit CYP enzymes | Increase valproate levels |
| Diazepam, phenytoin | Displaced from protein binding | May have altered free-fraction levels |
| Lithium | Pharmacodynamic | Exacerbation of tremor; otherwise generally safe combination |
| Antipsychotics | Pharmacodynamic | Increased sedation; lowered seizure threshold antagonizes valproate's anticonvulsant effect |
X. CONTRAINDICATIONS
- Hepatic disease or severe hepatic impairment
- Personal or family history of severe hepatic dysfunction
- Women of child-bearing potential (UK/EU regulatory contraindication)
- Known hypersensitivity to valproate
- Mitochondrial disorders (e.g., Alpers-Huttenlocher syndrome) - particularly in children
- Urea cycle disorders (risk of fatal hyperammonaemic encephalopathy)
XI. DISCONTINUATION
- If discontinuing, taper slowly over at least 1 month (preferably longer) to avoid precipitating mood relapse (Maudsley, p. 316)
- Whether abrupt withdrawal worsens the natural course of bipolar illness as severely as lithium withdrawal is unknown; caution is prudent
- In epilepsy, valproate withdrawal is associated with depression, falls, and hospital admissions
XII. SUMMARY TABLE
| Feature | Detail |
|---|---|
| Drug class | Branched-chain fatty acid / Mood stabilizer / Anticonvulsant |
| Primary indication | Bipolar I disorder - acute mania |
| Mechanism | VSSCs inhibition, GABA potentiation, signal transduction modulation |
| Therapeutic plasma level | 50-125 µg/mL |
| Onset of action | 1-4 days (therapeutic levels); rapid loading achieves this in 1 day |
| Dosing | 750-2,000 mg/day; loading dose 20-30 mg/kg/day |
| Key monitoring | LFTs, FBC, BMI, plasma levels |
| Serious adverse effects | Hepatotoxicity, teratogenicity, pancreatitis, thrombocytopenia, PCOS |
| Absolute contraindication | Liver disease; women of child-bearing potential (UK/EU) |
| Critical drug interaction | Lamotrigine (raises levels 2x - risk of SJS/TEN) |
REFERENCES
- Sadock BJ, Sadock VA, Ruiz P. Kaplan and Sadock's Synopsis of Psychiatry. 11th ed. Wolters Kluwer; 2015. Chapter 21, pp. 1979-1990.
- Stahl SM. Stahl's Essential Psychopharmacology: Neuroscientific Basis and Practical Application. 5th ed. Cambridge University Press; 2021. Chapter 7, pp. 363-370.
- Taylor D, Barnes TRE, Young AH. The Maudsley Prescribing Guidelines in Psychiatry. 15th ed. Wiley-Blackwell; 2021. Chapter 2 (Valproate), pp. 313-317.
This is a shared conversation. Sign in to Orris to start your own chat.