
Ans the laq
transverse section thorax T4 level anatomy labelled diagram structures
https://mapkmc.manipal.edu/specimen/anat231
A clean, detailed, labelled anatomical diagram of a transverse section (cross-section) of the thorax at the level of T4 vertebra (sternal angle / angle of Louis). Show the following structures clearly labelled: Sternum (anteriorly), Body of T4 vertebra (posteriorly), Spinal cord within vertebral canal, Right and left lungs (in pleural cavities), Superior mediastinum contents: Arch of Aorta (left side), Superior Vena Cava (right side), Trachea bifurcating into Right and Left principal bronchi (carina at T4), Oesophagus (posterior to trachea), Azygos vein (right side, posteriorly), Left phrenic nerve, Right phrenic nerve, Left vagus nerve, Right vagus nerve, Thoracic duct, Parietal pleura lining the cavity. Draw on a white background with clear black labels and arrows, anatomical orientation (anterior at top, posterior at bottom, right on left side of diagram, left on right side). Medical textbook style diagram.
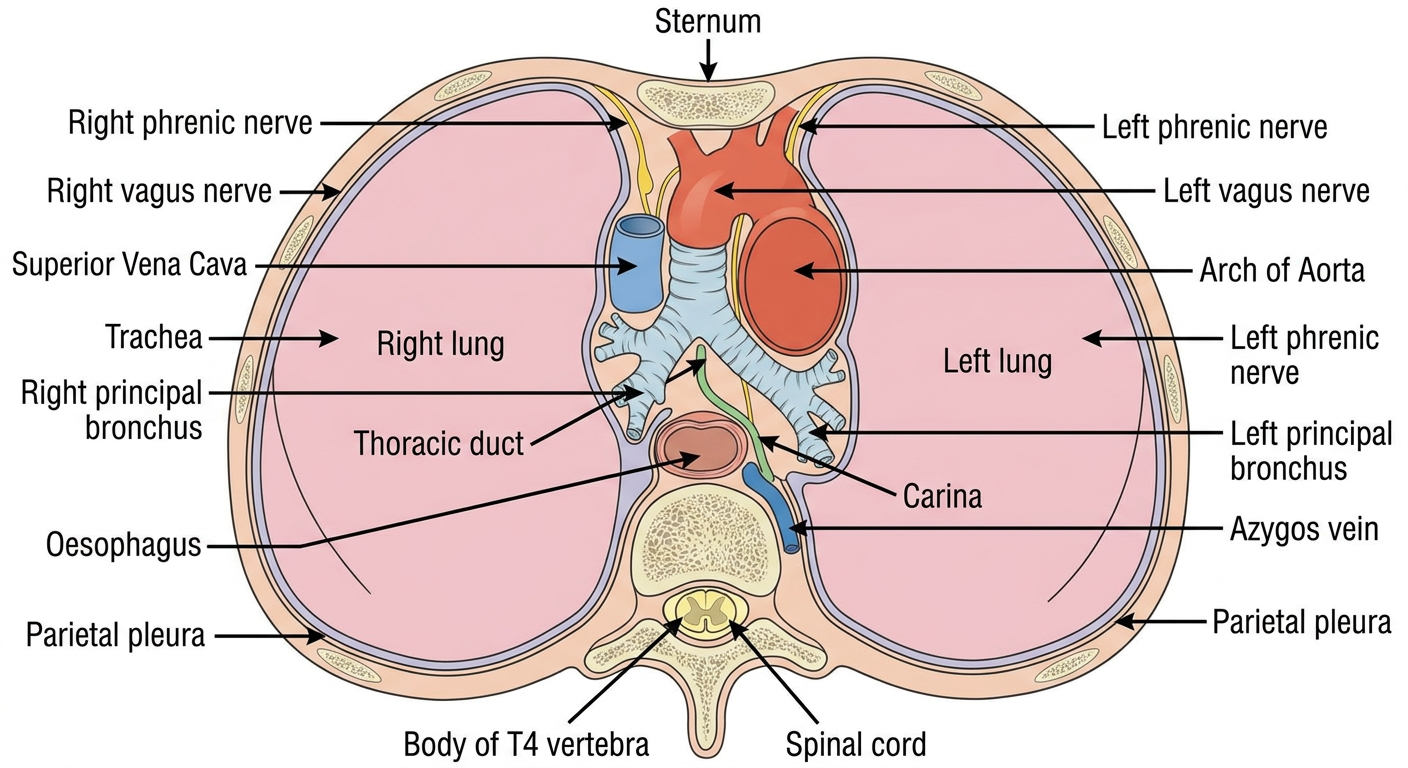
- The bifurcation of the trachea (carina) into right and left principal bronchi
- The beginning and end of the arch of aorta
- The junction between the superior and inferior mediastinum
- The level of the 2nd costal cartilage anteriorly (sternal angle)
| Structure | Position |
|---|---|
| Sternum | Anterior |
| T4 vertebral body + spinal cord | Posterior |
| Arch of Aorta | Left side of superior mediastinum |
| Superior Vena Cava (SVC) | Right side, anterior mediastinum |
| Tracheal bifurcation / Carina | Central, posterior |
| Right & Left principal bronchi | Diverging laterally from carina |
| Oesophagus | Posterior to trachea, anterior to vertebra |
| Azygos vein | Right side, posteriorly |
| Thoracic duct | Left side, posterior |
| Right & Left phrenic nerves | Lateral to pericardium |
| Right & Left vagus nerves | Posterior, on either side of trachea |
| Right & Left lungs | Lateral (in pleural cavities) |
| Parietal & visceral pleura | Lining pleural cavities |
- Trachea bifurcates
- Arch of aorta begins/ends
- Superior/inferior mediastinum junction
- Sternal angle (angle of Louis) anteriorly
Ans 1 question
1
Q1. Submandibular Salivary Gland
a) External Features
- Shape: Irregular, roughly the size of a walnut
- Has a larger superficial part and a smaller deep part, both continuous around the posterior border of mylohyoid muscle
- Partially enclosed between two layers of deep cervical fascia (from the greater cornu of hyoid bone)
- It is a mixed but predominantly serous gland (~90% serous, 10% mucous)
- The superficial part lies in the digastric triangle
- Wharton's duct (~5 cm long) opens at the sublingual papilla beside the frenulum of the tongue
- The lingual nerve crosses the duct laterally on the hyoglossus muscle (crosses it twice - hooks around it)
b) Relations
| Surface | Relations |
|---|---|
| Inferior | Skin, platysma, deep fascia; crossed by facial vein + cervical branch of facial nerve |
| Lateral | Submandibular fossa of mandible + medial pterygoid (mandibular attachment) |
| Medial - anterior part | Mylohyoid muscle |
| Medial - posterior part | Styloglossus muscle |
| Medial - intermediate part | Hyoglossus, separated from it by: lingual nerve, submandibular ganglion, hypoglossal nerve, deep lingual vein |
- Lies between mylohyoid (inferolaterally) and hyoglossus/styloglossus (medially)
- Extends forwards to the posterior end of the sublingual gland
c) Nerve Supply
- Pre-ganglionic fibres: CN VII (facial nerve) → Chorda tympani → joins Lingual nerve → Submandibular ganglion (synapse here)
- The ganglion is a small fusiform body suspended from the lingual nerve, lying on hyoglossus muscle
- Post-ganglionic fibres from the ganglion supply the submandibular and sublingual glands
- Post-ganglionic fibres from superior cervical ganglion via plexus on the facial artery
- Effect: vasoconstriction, reduces secretion
- Lingual nerve (branch of V3 - mandibular division of trigeminal)
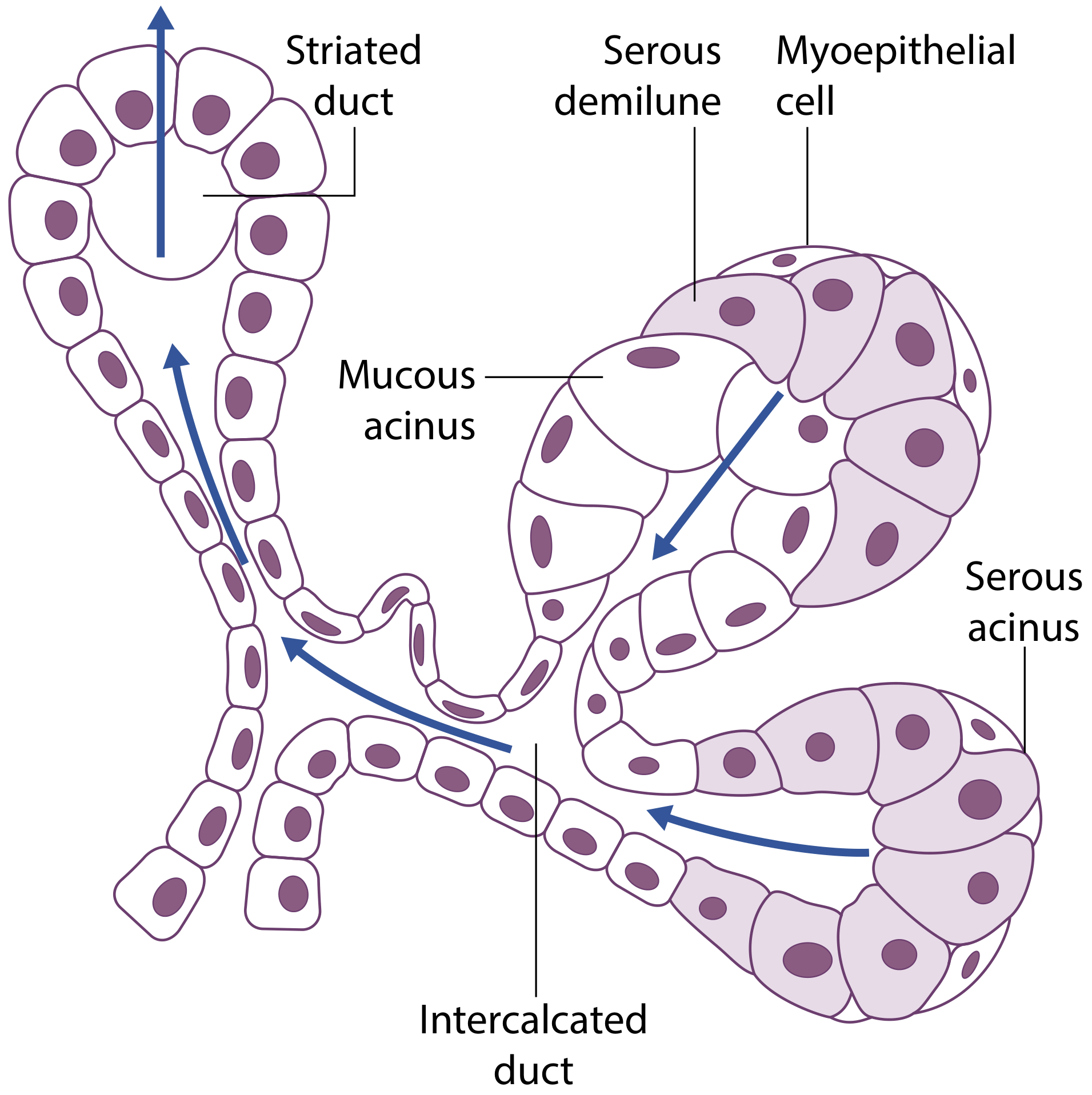
d) Micro-anatomy (Histology)
| Cell Type | Granules | Product |
|---|---|---|
| Serous | Small, dense | Proteins, enzymes (amylase) |
| Mucous | Large, pale | Mucoproteins |
| Seromucinous | Intermediate | Mixed |
- Intercalated ducts - low cuboidal epithelium; surrounded by myoepithelial cells
- Striated ducts - columnar cells with basal folding (striations); active water and electrolyte transport
- Excretory ducts - tall columnar epithelium
- Wharton's duct - main duct opening at sublingual papilla
e) Clinical Anatomy
-
Sialolithiasis (Calculi) - ~80% of all salivary calculi occur in Wharton's duct. Reasons:
- Duct is long (5 cm) and runs upward against gravity
- Saliva is viscous and alkaline
- Causes: painful swelling at mealtimes ("dinner-time syndrome")
-
Submandibular sialadenitis - Chronic inflammation, often secondary to stones; gland becomes densely fibrotic and tethered
-
Nerves at risk in submandibulectomy:
- Marginal mandibular nerve (runs ~2 cm below mandible over facial vessels) → damage = drooping corner of mouth
- Lingual nerve → damage = loss of taste + sensation to anterior 2/3 of tongue
- Hypoglossal nerve → damage = ipsilateral tongue paralysis and wasting
-
Tumours - ~50% of submandibular gland tumours are malignant (much higher malignancy rate than parotid). Total excision is always indicated.
-
Ludwig's angina - Severe bilateral cellulitis of submandibular and sublingual spaces, usually from lower molar infections; can cause fatal airway obstruction.
-
Frey's syndrome - Rare after submandibulectomy; aberrant regeneration of parasympathetic fibres causing gustatory sweating.
Facial → Chorda tympani → Lingual → Submandibular ganglion → Gland "Fools Can Love Salivary Glands"