Explain necrosis and it's types
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have all the content and image URLs needed. Let me compile the comprehensive answer.
Necrosis and Its Types
Necrosis is a form of pathologic, unregulated cell death that occurs as a consequence of severe injury. It is distinct from apoptosis (programmed cell death) in that it is accompanied by membrane disruption, leakage of cellular contents, and a local inflammatory reaction.
Definition and Basic Mechanism
Necrosis results when cells suffer irreparable damage. The main causes include:
- Ischemia (loss of oxygen supply)
- Microbial toxins and infections
- Burns and physical/chemical injury
- Active proteases leaking from cells (e.g., in pancreatitis)
These triggers cause denaturation of cellular proteins and damage to plasma and organellar membranes. Lysosomal enzymes leak into the cytoplasm and digest the cell from within. Cellular contents spill into the extracellular space and act as damage-associated molecular patterns (DAMPs) - including ATP and uric acid - which are recognized by macrophage receptors, triggering phagocytosis and cytokine-mediated inflammation.
This is a key distinction: necrosis always elicits inflammation; apoptosis does not.
Morphologic Features of Necrosis
Cytoplasmic Changes
- Increased eosinophilia on H&E staining - due to denatured cytoplasmic proteins binding eosin, plus loss of basophilic RNA
- Glassy, homogeneous appearance - from loss of glycogen particles
- Vacuolated, "moth-eaten" cytoplasm - when organelles are digested by enzymes
- On electron microscopy: discontinuities in membranes, dilated mitochondria with amorphous densities, disrupted lysosomes
Nuclear Changes (3 patterns)
- Pyknosis - nuclear shrinkage and increased basophilia; DNA condenses into a dark mass
- Karyorrhexis - fragmentation of the pyknotic nucleus
- Karyolysis - fading of basophilia due to DNA digestion by DNase; nucleus dissolves over 1-2 days
Types of Necrosis
There are 6 morphologically distinct patterns of tissue necrosis:
1. Coagulative Necrosis
Most common type. The underlying tissue architecture is preserved for several days after the injury.
- The injury denatures both structural proteins and enzymes, halting proteolysis
- Dead cells appear as eosinophilic, anucleate "ghost cells" that persist for days to weeks
- Eventually digested by leukocyte lysosomal enzymes and cleared by phagocytosis
- Affected tissue takes on a firm texture
Characteristic of: Infarcts in all solid organs except the brain (heart, kidney, spleen, liver)
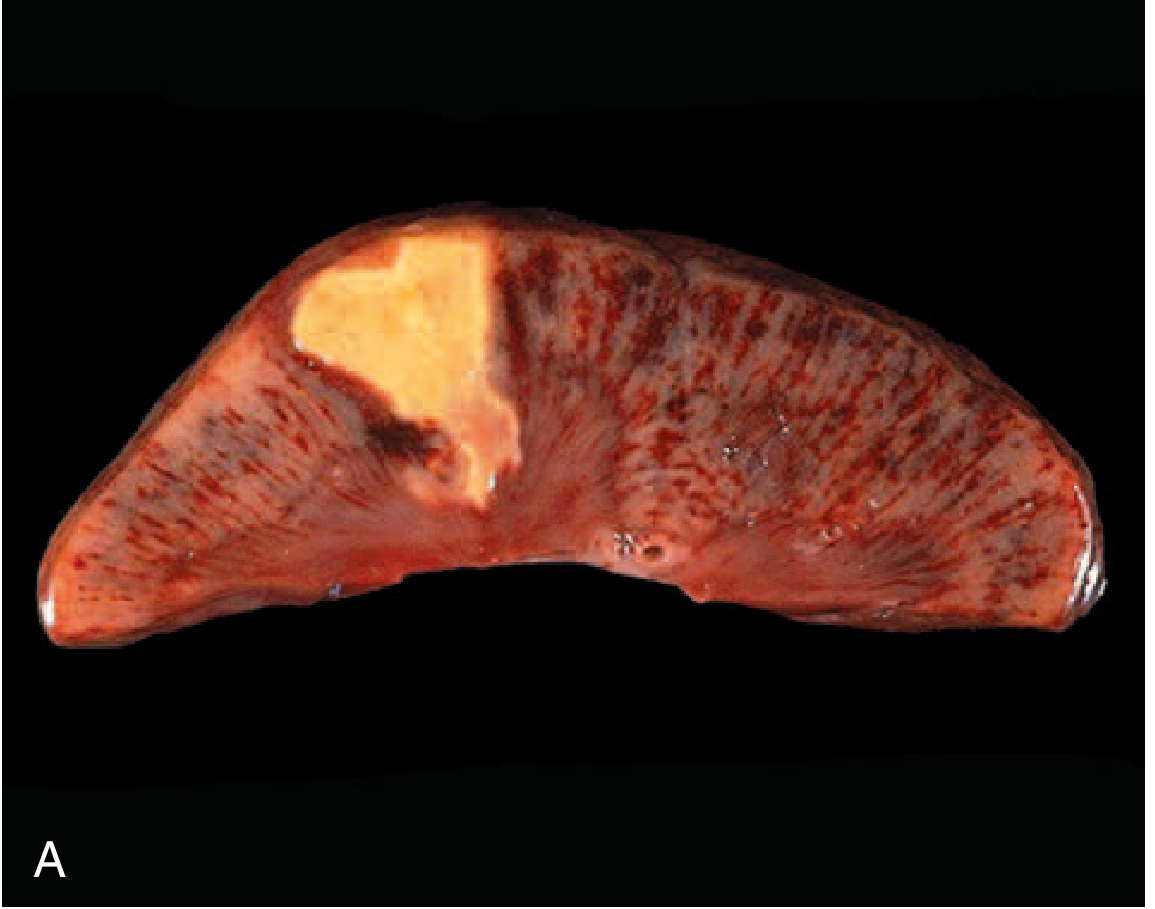
FIG. 1.6 - Coagulative necrosis: a wedge-shaped kidney infarct (yellow) with preserved outline but loss of nuclei.
2. Liquefactive Necrosis
The dead cells are completely digested, transforming tissue into a viscous liquid that is eventually removed by phagocytes.
- Occurs when microbial infections (bacterial or fungal) stimulate accumulation of inflammatory cells, whose enzymes "liquefy" the tissue
- Also occurs in hypoxic death of CNS cells (for unclear reasons - the brain is the exception to coagulative necrosis)
- When initiated by acute inflammation (e.g., bacteria), the liquid material is creamy yellow = pus
- A localized collection of pus = abscess
Characteristic of: Brain infarcts; bacterial/fungal infections (abscesses)

FIG. 1.7 - Liquefactive necrosis: brain infarct showing complete tissue dissolution.
3. Caseous Necrosis
Named from the Latin for "cheese" - the tissue has a friable, yellow-white, cheese-like gross appearance.
- On microscopy: amorphous granular pink (eosinophilic) debris; tissue architecture is completely obliterated (unlike coagulative necrosis)
- Cellular outlines cannot be discerned
- Typically surrounded by a rim of macrophages and other inflammatory cells = granuloma
Characteristic of: Tuberculous infections (most classic), some fungal infections
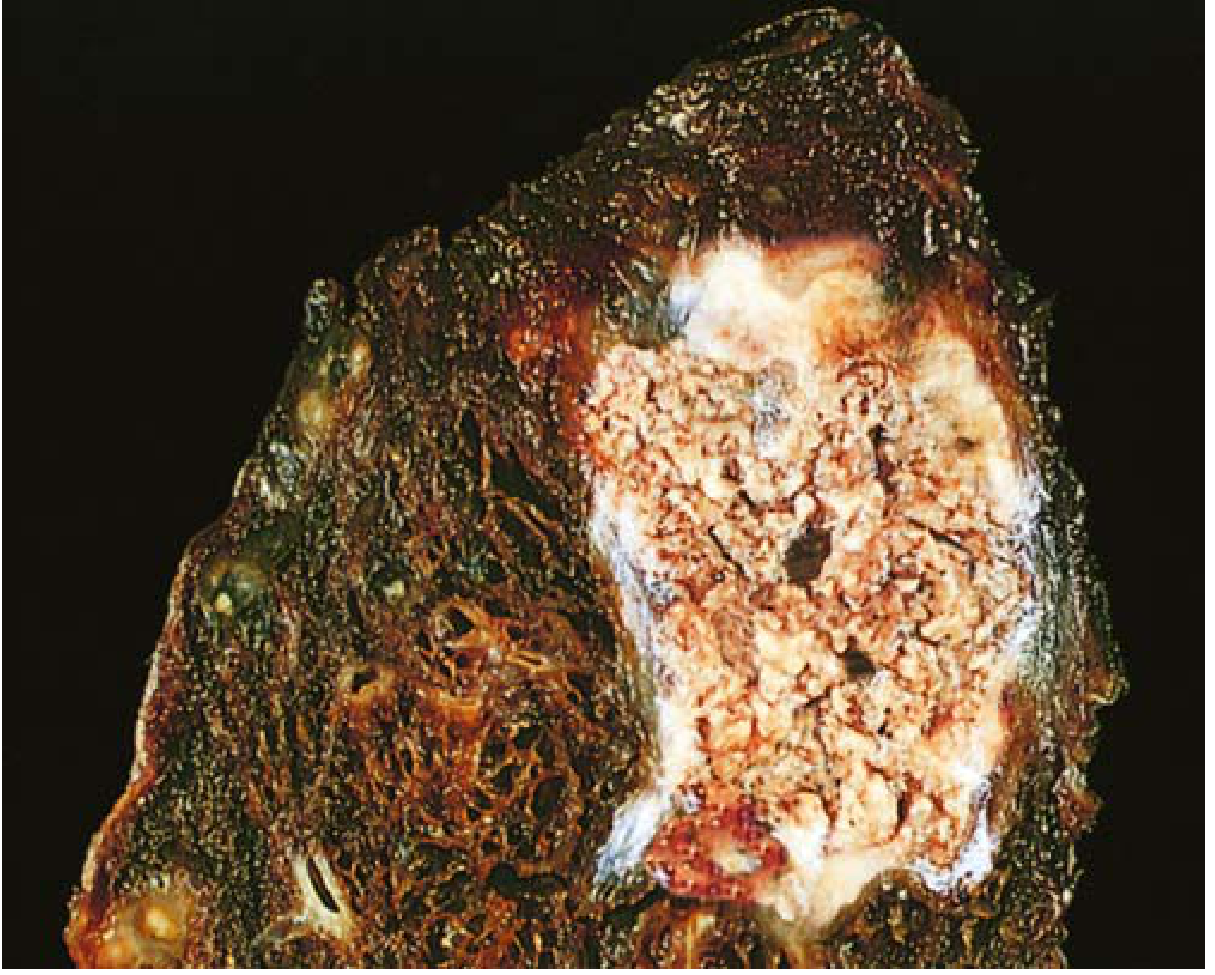
FIG. 1.8 - Caseous necrosis: tuberculosis of the lung with a large area of cheesy necrotic debris.
4. Fat Necrosis
Focal areas of fat destruction. Two main mechanisms:
- Traumatic fat necrosis - direct physical trauma to fatty tissue (e.g., breast)
- Enzymatic fat necrosis - in acute pancreatitis, lipases leak from damaged pancreatic acinar cells and ducts and digest peritoneal fat cells, releasing fatty acids which combine with calcium to form chalky white deposits (saponification)
- On histology: shadowy outlines of necrotic fat cells surrounded by granular basophilic calcium deposits and inflammation
Characteristic of: Acute pancreatitis (mesentery/omentum), breast trauma
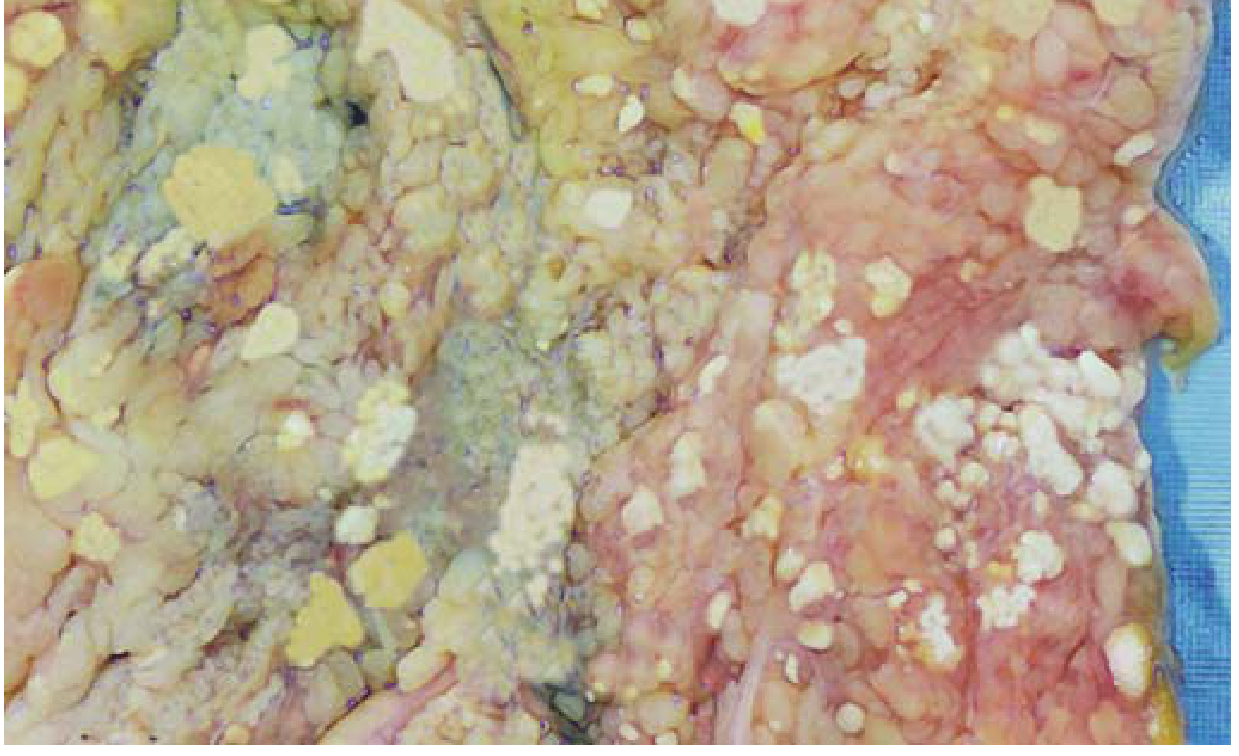
FIG. 1.9 - Fat necrosis in acute pancreatitis: white chalky deposits = saponification.
5. Gangrenous Necrosis
Not a histologically distinct pattern - rather a clinical term referring to necrosis of a limb (usually lower leg) that has lost its blood supply.
- Dry gangrene = coagulative necrosis without bacterial superinfection; tissue is dry, dark, and mummified
- Wet gangrene = when bacterial infection is superimposed, the appearance becomes liquefactive due to destruction by bacterial enzymes and leukocytes; tissue is moist and malodorous
- Gas gangrene = caused by Clostridium species; gas bubbles form in the tissue due to fermentation
Characteristic of: Diabetic foot, peripheral vascular disease, frostbite
6. Fibrinoid Necrosis
Detected only by microscopy (no gross appearance). A special form seen in vessel walls.
- Caused by deposition of antigen-antibody complexes (immune complexes) or plasma proteins that have leaked into vessel walls, often in severe hypertension
- Appears as a bright pink, amorphous material in the vessel wall on H&E - resembling fibrin ("fibrin-like" = fibrinoid)
Characteristic of: Certain forms of vasculitis, malignant hypertension, transplant rejection

FIG. 1.10 - Fibrinoid necrosis in an artery.
Summary Table
| Type | Mechanism | Gross Appearance | Location/Cause |
|---|---|---|---|
| Coagulative | Protein denaturation preserves architecture | Firm, pale, "ghost cells" | Infarcts - heart, kidney, spleen (not brain) |
| Liquefactive | Enzymatic digestion liquefies tissue | Fluid-filled cavity / pus | Brain infarcts, bacterial abscesses |
| Caseous | Combination of coagulation + liquefaction | Friable, yellow-white, cheese-like | Tuberculosis, some fungi |
| Fat | Lipase digestion of fat | White chalky deposits (saponification) | Pancreatitis, breast trauma |
| Gangrenous | Ischemia ± bacterial infection | Dry/mummified (dry) or wet/malodorous (wet) | Diabetic foot, PVD |
| Fibrinoid | Immune complex deposition in vessels | Bright pink, amorphous (microscopy only) | Vasculitis, malignant hypertension |
Clinical Relevance: Biomarkers of Necrosis
Necrosis-associated leakage of intracellular proteins into the circulation forms the basis for clinical blood tests:
- Cardiac troponins - detect myocardial necrosis (elevated as early as 2 hours after MI); central to MI diagnosis
- Transaminases (ALT, AST) - detect hepatocyte necrosis
- Alkaline phosphatase - bile duct epithelial necrosis
Sources: Robbins & Kumar Basic Pathology, 11th ed., pp. 21-23; Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 1377-1388
This is a shared conversation. Sign in to Orris to start your own chat.