Gastric cancer classification in simple words
Reading File
Finding Sources
Searching the Web
gastric cancer classification Lauren WHO simple overview
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Searching Images
Borrmann classification gastric cancer gross types
Loading Image
Loading Image
Here is a clear, structured overview of gastric cancer classification from the ground up.
Gastric Cancer Classification — Simple Overview
Almost all gastric cancers (>90%) are adenocarcinomas (cancer of gland-forming cells). They are classified in several overlapping ways:
1. By Depth of Invasion (Stage)
The most clinically important split:
| Stage | What it means | Prognosis |
|---|---|---|
| Early gastric cancer (EGC) | Cancer stays in mucosa/submucosa — regardless of lymph node spread | Excellent — ~90% 5-year survival |
| Advanced gastric cancer | Cancer invades into the muscle layer and beyond | Poor — <20% 5-year survival in the West |
2. By Gross (Visible) Appearance — The Japanese & Borrmann Classifications
Early Gastric Cancer (Japanese Classification)
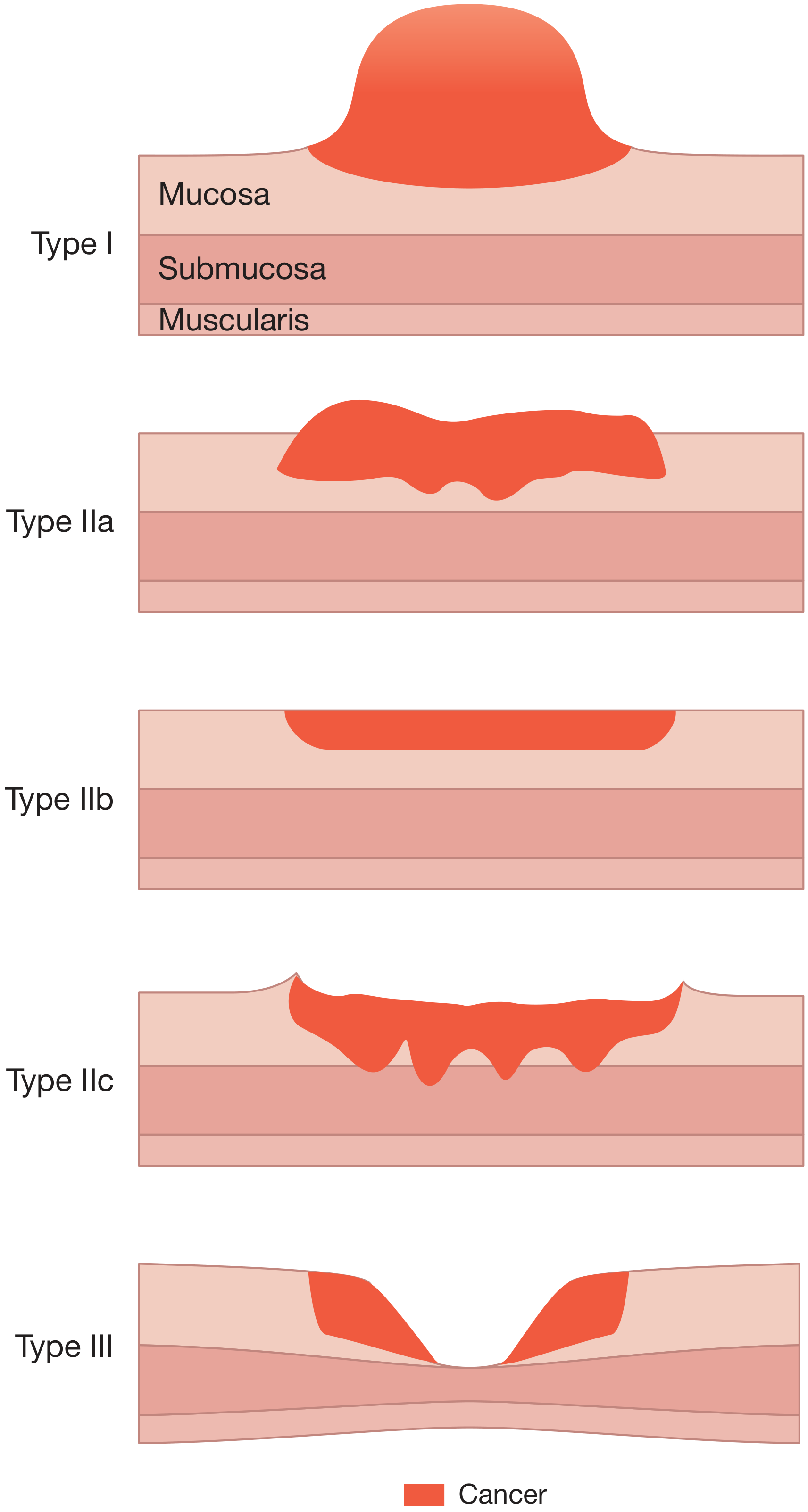
| Type | Appearance |
|---|---|
| Type I | Protruding / polypoid bump |
| Type IIa | Slightly raised |
| Type IIb | Flat |
| Type IIc | Slightly depressed |
| Type III | Ulcerated crater |
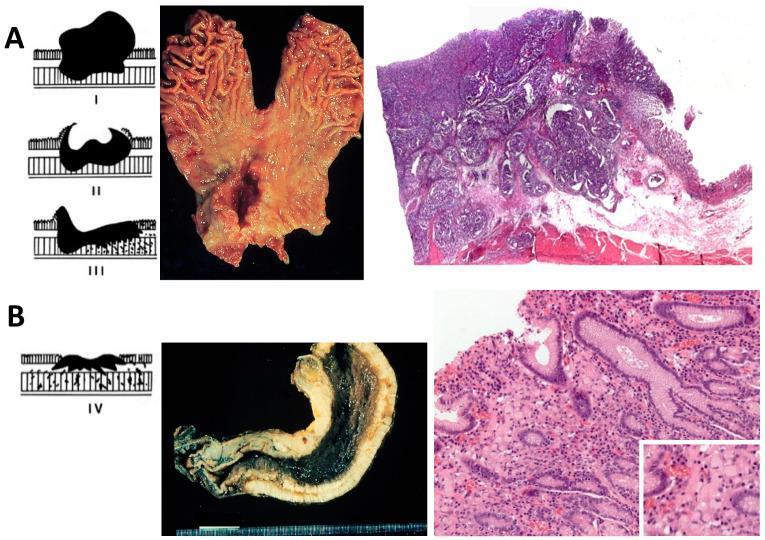
Advanced Gastric Cancer (Borrmann Classification, 1926)
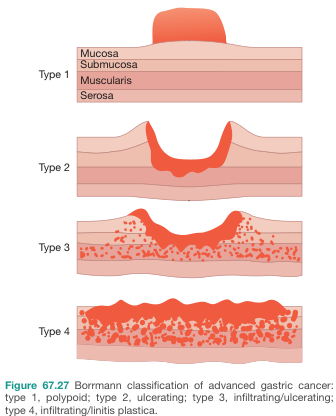
| Type | What it looks like | Key point |
|---|---|---|
| I | Polypoid — mushroom-like mass | Best prognosis |
| II | Ulcerating — deep ulcer with sharp edges | Clearly defined |
| III | Ulcerating + infiltrating — ragged edges | Most common |
| IV | Diffusely infiltrating — "linitis plastica" (leather-bottle stomach) | Worst prognosis |
Types III and IV are usually incurable at diagnosis.
3. By Microscopic Appearance — Laurén Classification (1965)
The most clinically used histological system:
| Feature | Intestinal Type | Diffuse Type |
|---|---|---|
| Cell arrangement | Forms glands (organized) | Loose single cells, no glands |
| Look under microscope | Well-differentiated | Poorly differentiated; signet ring cells (mucin pushes nucleus to side) |
| How it grows | Polypoid or ulcerated mass | Spreads through stomach wall silently |
| Who gets it | Older men, high-incidence areas (Asia, S. America) | Both sexes, younger patients |
| Associated with | H. pylori, intestinal metaplasia, atrophic gastritis | CDH1 mutation; blood type A |
| Metastasis pattern | Tends to go to liver | Tends to go to peritoneum |
| Prognosis | Better | Worse |
There is also a Mixed type (both components → intermediate-poor prognosis) and an Indeterminate type.
4. By WHO Microscopic Subtypes (2019)
The WHO gives more detail, but roughly maps back to Laurén:
| WHO Subtype | Frequency | Corresponds to Laurén |
|---|---|---|
| Tubular adenocarcinoma | Most common (45–64%) | Intestinal |
| Papillary adenocarcinoma | 3–10%; higher liver mets risk | Intestinal |
| Poorly cohesive (incl. signet ring cell) | 20–54% | Diffuse |
| Mucinous adenocarcinoma | 2–8% | Mixed |
| Mixed-pattern | 6–22%; poor prognosis | Mixed |
5. By Location in the Stomach
| Location | Notes |
|---|---|
| Cardia / proximal | Common in low-incidence regions (UK, N. America); linked to GERD |
| Distal (antrum/body) | Common in high-incidence regions (Asia, Eastern Europe); linked to H. pylori |
In high-incidence areas, 80% are distal. In the West, 50–60% are proximal/cardia.
6. By Molecular Subtype — TCGA Classification (2014)
The Cancer Genome Atlas divided gastric cancer into 4 molecular subtypes with different drivers and treatment implications:
| Subtype | Key feature | Histology link |
|---|---|---|
| EBV-positive | Epstein-Barr virus in tumor cells; good response to immunotherapy | Good prognosis |
| MSI (Microsatellite unstable) | DNA mismatch repair defects; responds well to checkpoint inhibitors | Intestinal-like |
| CIN (Chromosomal instability) | TP53 mutations; most common | Intestinal type |
| GS (Genomically stable) | CDH1 / RHOA mutations | Diffuse type; worst prognosis |
Quick Summary Table
| System | What it tells you |
|---|---|
| Early vs Advanced | Depth of wall invasion → prognosis & curability |
| Japanese classification | Shape of early lesions → guides endoscopic treatment |
| Borrmann | Shape of advanced lesions → gross surgical/endoscopic description |
| Laurén | Intestinal vs diffuse → biology, epidemiology, spread pattern |
| WHO | Detailed microscopic subtypes |
| TCGA molecular | Genetic drivers → targeted therapies, immunotherapy eligibility |
Sources: Bailey & Love's Short Practice of Surgery (28th ed.), Sabiston Textbook of Surgery, Yamada's Textbook of Gastroenterology (7th ed.)
This is a shared conversation. Sign in to Orris to start your own chat.