Uric acid in joints treatment
Reading File
Finding Sources
Searching PubMed
"gout"[MeSH Terms] AND "treatment"[MeSH Terms]
Searching the Web
gout uric acid joints treatment 2025 guidelines
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a complete guide to treating uric acid deposits in joints (gout), compiled from authoritative rheumatology and pharmacology textbooks.
Treatment of Uric Acid in Joints (Gout)
What Happens in the Joint
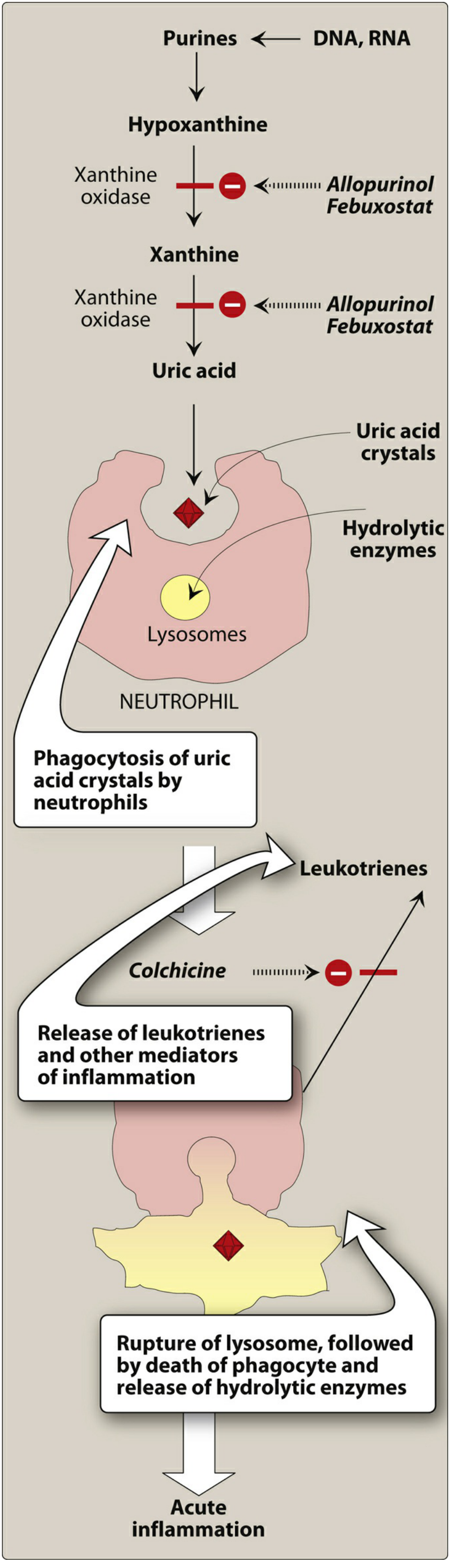
Gout occurs when uric acid (urate) accumulates in the blood beyond its saturation point (~6 mg/dL), causing sodium urate crystals to deposit in joints. Neutrophils phagocytize these crystals, releasing hydrolytic enzymes and leukotrienes that trigger acute inflammation. This cycle is illustrated below:
PART 1 - Treatment of an Acute Gout Attack
The goal during an acute flare is to suppress inflammation and control pain as quickly as possible. The attack will resolve on its own over days, but prompt treatment can abort it within hours. Do NOT start urate-lowering therapy during an acute attack - sudden changes in uric acid levels can worsen or prolong it.
1. NSAIDs (First-Line)
| Drug | Dose |
|---|---|
| Indomethacin | 50 mg PO three times daily |
| Ibuprofen | 800 mg PO three times daily |
| Naproxen | 500 mg twice daily |
| Meloxicam | 15 mg daily |
- Indomethacin is the classic NSAID of choice for gout.
- Avoid in CKD, peptic ulcer disease, or patients on anticoagulation.
2. Colchicine
Dose: 1.2 mg PO, followed by 0.6 mg one hour later.
- A plant alkaloid; it works by binding to tubulin (a microtubular protein), causing depolymerization. This disrupts neutrophil migration into the inflamed joint.
- Most effective when started within 24-36 hours of attack onset; usually alleviates pain within 12 hours.
- Also used as prophylaxis when starting urate-lowering therapy.
- Adverse effects: Nausea, vomiting, diarrhea, abdominal pain. Chronic use can cause myopathy, neutropenia, aplastic anemia.
- Avoid in CKD; avoid concomitant use with carvedilol or grapefruit juice (both raise colchicine blood levels). Dose-adjust with CYP3A4 inhibitors (e.g., clarithromycin) or P-gp inhibitors (e.g., amiodarone, verapamil).
3. Corticosteroids
- Intra-articular: Triamcinolone or methylprednisolone - 40 mg for large joints, 10-20 mg for small joints. Best for monoarticular attacks; effective in ~90% of patients within 24 hours. Rule out septic arthritis first.
- Oral: Prednisone 40-60 mg once daily until flare begins to resolve, then taper over 7-10 days. Use when NSAIDs and colchicine are contraindicated. Use with caution in poorly controlled diabetes.
4. IL-1 Inhibitor (Anakinra) - for refractory cases
Dose: 100 mg subcutaneously once daily for 3 days (every other day if CrCl <30). Reserved for cases where standard therapy is contraindicated or ineffective. Avoid in active infection. Canakinumab is another IL-1 inhibitor option in patients who cannot tolerate NSAIDs or colchicine.
PART 2 - Urate-Lowering Therapy (ULT) for Long-Term Management
When to Start ULT
ULT is indicated when:
- Two or more acute flares per year
- Presence of tophi (urate crystal deposits in joints, bones, cartilage)
- Urate nephropathy or kidney stones
- Radiographic joint damage
- First gout attack with uric acid >9 mg/dL, or CKD stage ≥3
Timing: Start at least 2 weeks after the acute attack resolves. If a patient is already on ULT, do NOT stop it during an attack.
Uric Acid Targets (Treat-to-Target)
- No tophi: target uric acid <6 mg/dL
- With tophi: target <5 mg/dL
Drug Options
Xanthine Oxidase Inhibitors (First-Line)
Allopurinol
- Starting dose: 100 mg/day (50 mg/day in CKD stage 4+). Titrate by 100 mg increments every 2-5 weeks up to 800 mg/day if needed.
- Mechanism: competitively inhibits xanthine oxidase, blocking the last two steps in uric acid biosynthesis (hypoxanthine → xanthine → uric acid).
- Preferred over febuxostat and probenecid as first-line agent.
- Screen for HLA-B*5801 in African Americans and Southeast Asians before starting - positive carriers have a high risk of severe cutaneous reactions (allopurinol hypersensitivity syndrome, ~25% mortality).
- Important interaction: Blocks metabolism of azathioprine and 6-mercaptopurine - reduce those doses by 60-75%.
- Side effects: diarrhea, nausea, transaminitis, rash.
Febuxostat
- Dose: 40-80 mg/day. 40 mg is roughly equivalent to 300 mg allopurinol.
- Second-line; more expensive than allopurinol.
- Associated with higher rate of cardiovascular events.
- Side effects: transaminitis.
Uricosuric Agents (Second-Line)
Probenecid
- Increases uric acid excretion via renal tubule. For patients intolerant of or with inadequate response to xanthine oxidase inhibitors.
- Dose: 500 mg/day initially, titrate up weekly; usual dose 1-1.5 g/day in divided doses; max 3 g/day.
- Requires normal renal function - not suitable in CKD.
Lesinurad - 200 mg/day; often combined with a xanthine oxidase inhibitor.
Uricase (Last Resort)
Pegloticase
- 8 mg IV every 2 weeks.
- Reserved for uncontrolled gout when all other agents fail and patient continues to have 2+ flares/year or persistent tophi.
- ACR guidelines strongly recommend against using as first-line therapy.
PART 3 - Prophylaxis During ULT Initiation
Starting ULT can trigger an acute attack (due to rapid shifts in serum urate levels). To prevent this, use one of the following for at least 6 months when initiating ULT:
- Low-dose colchicine
- Low-dose NSAIDs
- Low-dose corticosteroids
PART 4 - Lifestyle Modifications
- Avoid high-purine foods: organ meats, shellfish, red meat
- Limit alcohol (especially beer)
- Stay well hydrated (promotes uric acid excretion)
- Avoid fructose-rich drinks
- Manage contributing medications (e.g., diuretics raise uric acid)
- Weight loss if overweight
Summary Table
| Phase | Treatment | Goal |
|---|---|---|
| Acute attack | NSAIDs, Colchicine, Corticosteroids, IL-1 inhibitors | Suppress inflammation |
| Long-term (1st line) | Allopurinol or Febuxostat | Uric acid <6 mg/dL (<5 if tophi) |
| Long-term (2nd line) | Probenecid, Lesinurad | If XO inhibitors fail/not tolerated |
| Refractory | Pegloticase IV | Uncontrolled gout only |
| Prophylaxis (during ULT) | Low-dose colchicine/NSAID | Prevent flares for ≥6 months |
Sources: Lippincott Illustrated Reviews Pharmacology; The Washington Manual of Medical Therapeutics; ACR Gout Guidelines
This is a shared conversation. Sign in to Orris to start your own chat.