Explain me 10 common heart disease with ECG diagram and ECG images of those disease
Reading File
Finding Sources
Searching the Web
ECG diagrams 10 common heart diseases atrial fibrillation MI heart block LBBB images
Finding Sources
Searching the Web
ECG normal sinus rhythm atrial fibrillation myocardial infarction diagram labeled wikimedia
Finding Sources
Loading Image
Finding Sources
Searching the Web
ECG images ventricular tachycardia heart block STEMI LBBB Wolff-Parkinson-White clinical wikimedia commons
Finding Sources
Loading Image
Loading Image
Searching the Web
ECG STEMI heart attack ST elevation complete heart block third degree ventricular fibrillation torsades de pointes images
Loading Image
Reading Web Page
https://litfl.com/av-block-3rd-degree-complete-heart-block
Loading Image
Searching the Web
ECG left bundle branch block LBBB right bundle branch block RBBB hypertrophic cardiomyopathy Wolff-Parkinson-White delta wave clinical ECG strip
Loading Image
Loading Image
Loading Image
Loading Image
Here is a thorough guide to 10 common heart diseases with their ECG features and available images.
ECG Basics - Understanding the Waveform
Before diving into the diseases, here is the normal ECG waveform for reference:

| Waveform | What It Represents |
|---|---|
| P wave | Atrial depolarization (SA node firing) |
| PR interval | Conduction from atria to ventricles (0.12-0.20 s) |
| QRS complex | Ventricular depolarization (<0.12 s) |
| ST segment | Isoelectric period between depolarization and repolarization |
| T wave | Ventricular repolarization |
| QT interval | Total ventricular electrical activity |
10 Common Heart Diseases with ECG Findings
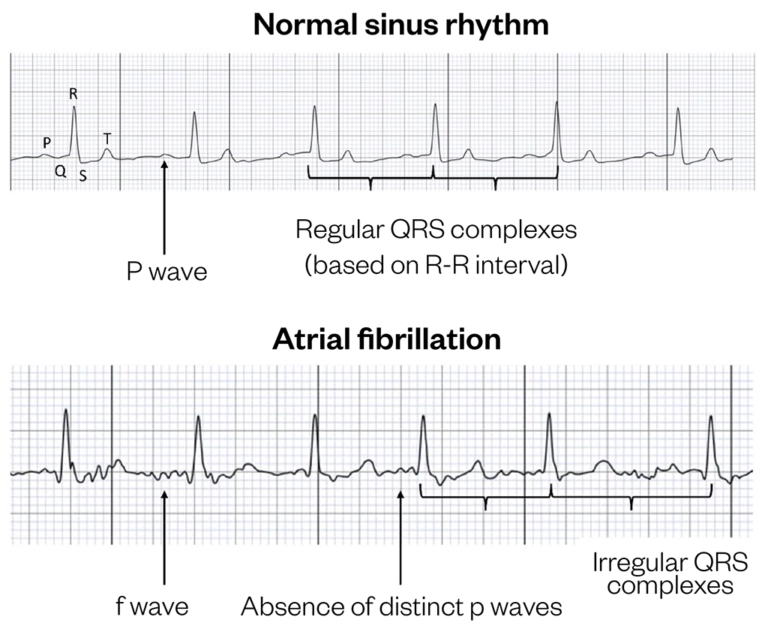
1. Atrial Fibrillation (AF)
What it is: The most common cardiac arrhythmia. Disorganized electrical activity in the atria causes rapid, chaotic impulses (350-600/min) that produce an irregular ventricular response.
Causes: Hypertension, heart failure, valvular disease, thyrotoxicosis, alcohol excess, sleep apnea.
Symptoms: Palpitations, shortness of breath, fatigue, stroke risk (5x increased).
ECG Features:
- No visible P waves - replaced by fibrillatory (f) waves
- Irregularly irregular RR intervals (no pattern)
- Narrow QRS (unless aberrant conduction or bundle branch block present)
- Ventricular rate typically 100-160 bpm if uncontrolled
2. ST-Elevation Myocardial Infarction (STEMI)
What it is: A complete occlusion of a coronary artery causing full-thickness (transmural) myocardial infarction. A true cardiac emergency requiring immediate revascularization.
Causes: Rupture of atherosclerotic plaque with thrombosis.
Symptoms: Severe crushing chest pain, diaphoresis, nausea, radiation to arm/jaw.
ECG Features (sequential evolution):
- Hyperacute T waves - earliest sign (tall, broad T waves)
- ST elevation ≥1 mm in 2 contiguous limb leads, or ≥2 mm in 2 contiguous precordial leads
- Pathological Q waves develop over hours to days (>40ms wide, >25% of R wave height)
- T wave inversion follows reperfusion or infarct evolution
- Reciprocal ST depression in opposite leads
- Lead localization: V1-V4 = anterior (LAD); II, III, aVF = inferior (RCA); I, aVL, V5-V6 = lateral (LCx)
Source: Harrison's Principles of Internal Medicine 22E - "ECG findings are ST elevation suggesting infarction, but also include conduction block, tachyarrhythmias, and nonspecific ST-T changes."
3. Left Bundle Branch Block (LBBB)
What it is: Failure of conduction down the left bundle branch. The left ventricle is depolarized late via the right ventricle, producing a wide, abnormal QRS.
Causes: Coronary artery disease, hypertension, aortic stenosis, cardiomyopathy. New LBBB with chest pain is a STEMI-equivalent until proven otherwise.
Symptoms: Often asymptomatic; may cause reduced cardiac output in diseased hearts.
ECG Features (use the WiLLiaM MaRRoW mnemonic):
- QRS duration ≥120 ms (broad)
- V1: Dominant S wave (rS or QS pattern) - deep, broad
- V6/I/aVL: Broad, notched or "M-shaped" R wave - no Q waves in lateral leads
- ST and T wave changes are discordant (opposite to QRS direction)
- No septal Q waves in lateral leads
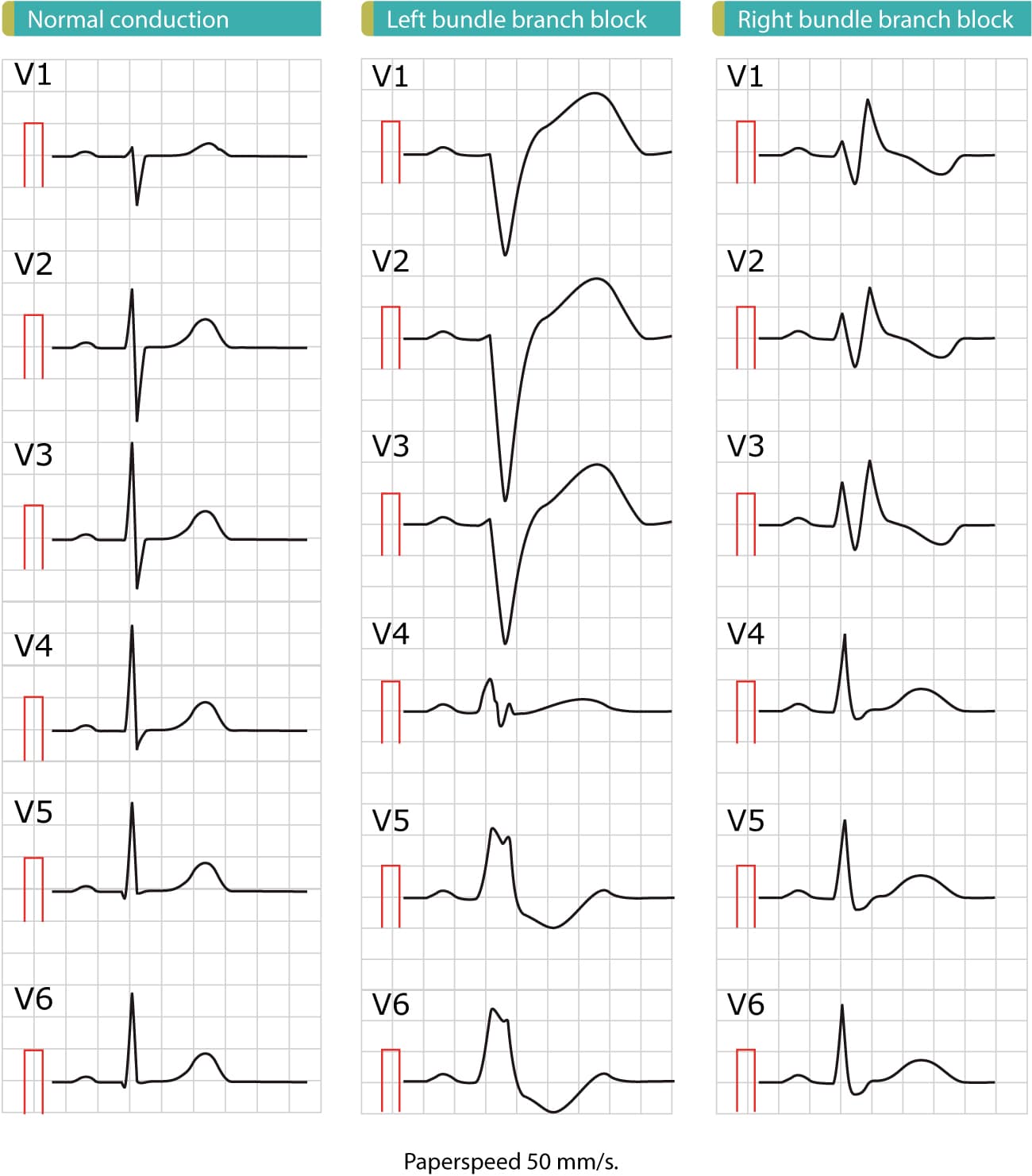
4. Right Bundle Branch Block (RBBB)
What it is: Conduction block in the right bundle branch. The right ventricle depolarizes late, producing a characteristic "M-shaped" pattern in V1.
Causes: Pulmonary embolism (acute RBBB), right heart strain, congenital heart disease, after cardiac surgery, can be a normal variant.
ECG Features (MaRRoW mnemonic for V1):
- QRS duration ≥120 ms
- V1: RSR' pattern - "M-shaped" or "rabbit ears" (rSR')
- V5-V6/I: Wide, slurred S wave (the late right ventricular activation)
- ST/T wave changes in V1-V3 (secondary)
- Right axis deviation may be present
(The LBBB vs RBBB comparison image above shows both patterns clearly across V1-V6)
5. Complete (Third-Degree) Heart Block
What it is: Complete dissociation between atria and ventricles. No atrial impulse conducts to the ventricles. The ventricles are maintained by an escape rhythm (junctional or ventricular).
Causes: Inferior STEMI (RCA occlusion), degenerative conduction system disease (Lenegre/Lev disease), medications (beta-blockers, digoxin), Lyme disease, post-cardiac surgery.
Symptoms: Syncope (Stokes-Adams attacks), extreme bradycardia, heart failure, sudden death.
ECG Features:
- P waves and QRS complexes march independently - complete AV dissociation
- P waves at their own rate (usually sinus, ~60-100 bpm)
- QRS at a slower escape rate (junctional = narrow QRS at 40-60 bpm; ventricular = wide QRS at 20-40 bpm)
- No consistent PR interval - it changes with every beat
- PP intervals are regular; RR intervals are regular - but they are NOT related to each other
6. Ventricular Tachycardia (VT)
What it is: A dangerous arrhythmia originating in the ventricles at a rate >100 bpm (usually 120-250 bpm). Can degenerate into ventricular fibrillation and cardiac arrest.
Causes: Ischemic heart disease (most common), cardiomyopathy, electrolyte disturbances (hypokalemia, hypomagnesemia), drugs (QT-prolonging agents), channelopathies.
Symptoms: Palpitations, presyncope, syncope, hemodynamic collapse.
ECG Features:
- Wide QRS complexes (>120ms), bizarre morphology
- Rate 120-250 bpm, regular
- AV dissociation (P waves visible, marching independently) - pathognomonic when seen
- Fusion beats and capture beats (specific signs of VT, not SVT)
- Concordance in precordial leads (all QRS positive or all negative)
- Brugada criteria / RBBB with left axis deviation patterns
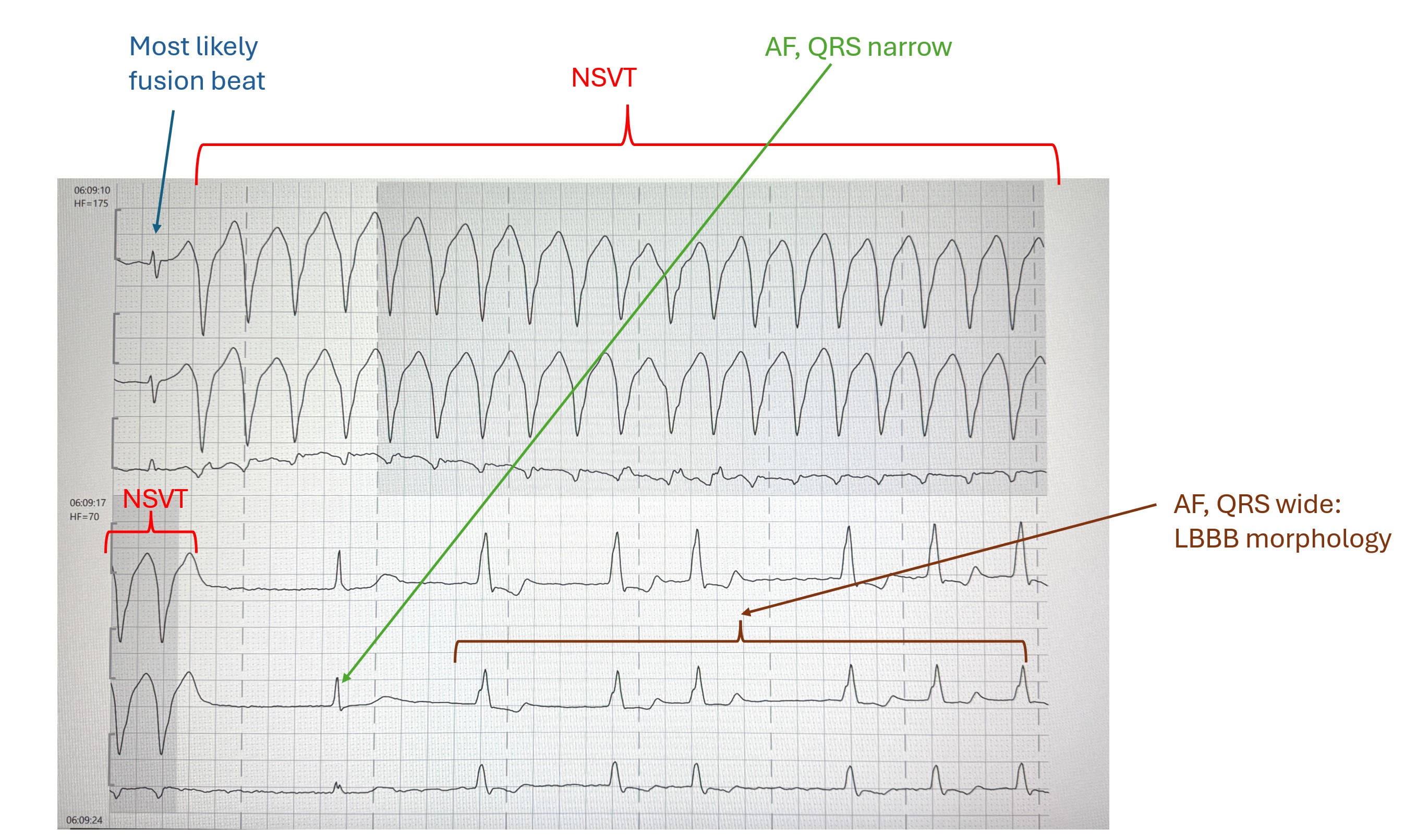
(Above: Non-sustained VT (NSVT) shown with wide-complex tachycardia, transitioning to AF with LBBB morphology)
7. Wolff-Parkinson-White (WPW) Syndrome
What it is: A pre-excitation syndrome caused by an accessory pathway (Bundle of Kent) that bypasses the AV node, allowing early ventricular activation (pre-excitation). Can cause life-threatening tachyarrhythmias including AF with rapid ventricular conduction.
Causes: Congenital - the accessory pathway is present from birth.
Symptoms: Palpitations, syncope, sudden cardiac death (especially in athletes).
ECG Features (the "delta wave triad"):
- Short PR interval (<120 ms) - bypass tract skips slow AV node conduction
- Delta wave - slurred upstroke at the start of the QRS (early ventricular activation)
- Wide QRS (>120 ms) - because ventricular muscle is depolarized via slow muscle-to-muscle spread
- Pseudo-LBBB or RBBB pattern depending on pathway location
- ST/T wave changes opposite to QRS (discordant)
- Risk: AF in WPW can conduct 1:1 via the accessory pathway → rapid VF → sudden death
8. Ventricular Fibrillation (VF)
What it is: Completely disorganized ventricular electrical activity with no effective contraction. Produces no cardiac output. Rapidly fatal without immediate defibrillation.
Causes: Acute STEMI (most common), VT degeneration, electrocution, hypokalemia/hypomagnesemia, drug toxicity, hypothermia, Brugada syndrome.
ECG Features:
- Chaotic, irregular, high-frequency oscillations - no recognizable P waves, QRS, or T waves
- Variable amplitude waveforms (coarse VF = larger amplitude, finer VF = smaller amplitude)
- No organized rhythm whatsoever
- Coarse VF is more likely to respond to defibrillation than fine VF
- Diagnosis is clinical + ECG - no pulse, no output
LITFL ECG Library: "Ventricular fibrillation is the most important shockable cardiac arrest rhythm. It is invariably fatal unless advanced life support is rapidly instituted."
9. Atrial Flutter
What it is: A macro-reentrant tachyarrhythmia originating in the right atrium, circulating around the tricuspid valve annulus at approximately 300 bpm. Typically conducts to ventricles with a fixed block (2:1, 3:1, or 4:1).
Causes: Same as atrial fibrillation - structural heart disease, hypertension, post-cardiac surgery, pulmonary disease.
Symptoms: Palpitations, dyspnea, reduced exercise tolerance.
ECG Features:
- "Sawtooth" flutter waves (F waves) at ~300 bpm - best seen in II, III, aVF and V1
- Regular ventricular rate (common 2:1 block → ventricular rate ~150 bpm)
- No isoelectric baseline between flutter waves
- Narrow QRS (unless aberrant conduction)
- 2:1 block: ventricular rate exactly 150 bpm should always raise suspicion for flutter
- Variable block (4:1, 3:1) produces slower ventricular rates
10. Left Ventricular Hypertrophy (LVH)
What it is: Pathological thickening of the left ventricular wall due to chronic pressure overload (hypertension, aortic stenosis) or volume overload. Associated with increased risk of arrhythmia, heart failure, and sudden death.
Causes: Hypertension (most common), aortic stenosis, hypertrophic cardiomyopathy, athletic remodeling (physiologic LVH).
Symptoms: Often asymptomatic; may cause exertional dyspnea, angina (from subendocardial ischemia).
ECG Features (Sokolow-Lyon criteria most commonly used):
- Increased QRS voltage:
- S wave in V1 + R wave in V5 or V6 ≥35 mm (Sokolow-Lyon)
- R wave in aVL ≥11 mm (Cornell criterion)
- R wave in V5 or V6 ≥26 mm
- "Strain pattern" - ST depression and T wave inversion in lateral leads (I, aVL, V5-V6)
- Left axis deviation
- Prolonged QRS (slight widening, but <120ms)
- Wide P wave or notched P wave (left atrial enlargement often coexists)
The 12-lead ECG below (from stemlynsblog) shows a patient with LVH - note the tall R waves in lateral leads and deep S waves in V1-V3:

Summary Table
| # | Disease | Key ECG Finding | Heart Rate | Rhythm |
|---|---|---|---|---|
| 1 | Atrial Fibrillation | No P waves, f waves, irregular RR | 100-160 (uncontrolled) | Irregularly irregular |
| 2 | STEMI | ST elevation + pathological Q waves | Variable | Regular (unless arrhythmia) |
| 3 | LBBB | Wide QRS, dominant S in V1, broad R in V6 | Variable | Regular |
| 4 | RBBB | Wide QRS, RSR' in V1 ("rabbit ears"), slurred S in V6 | Variable | Regular |
| 5 | Complete Heart Block | P and QRS dissociated; slow QRS escape | 20-60 bpm (ventricles) | Regular but dissociated |
| 6 | Ventricular Tachycardia | Wide QRS, AV dissociation, fusion beats | 120-250 bpm | Regular |
| 7 | WPW Syndrome | Short PR, delta wave, wide QRS | Variable | Variable |
| 8 | Ventricular Fibrillation | Chaotic, no recognizable waveforms | Undetectable | Absent |
| 9 | Atrial Flutter | Sawtooth F waves ~300 bpm, regular ventricular rate | ~150 bpm (2:1) | Regular |
| 10 | LVH | Tall voltage, strain pattern, LAD | Variable | Regular |
Clinical Pearls
- Any wide complex tachycardia (WCT) = VT until proven otherwise - do not assume it is SVT with aberrancy
- New LBBB + chest pain = STEMI equivalent - treat accordingly
- Ventricular rate exactly 150 bpm should always raise suspicion for atrial flutter with 2:1 block
- WPW + AF is dangerous - avoid AV node blocking drugs (adenosine, verapamil, digoxin) as they may accelerate conduction via the accessory pathway and trigger VF
- Complete heart block post-inferior MI is usually transient; post-anterior MI complete heart block is an ominous sign
Sources: Harrison's Principles of Internal Medicine 22E; Goldman-Cecil Medicine; Tintinalli's Emergency Medicine; Guyton and Hall Medical Physiology; LITFL ECG Library
This is a shared conversation. Sign in to Orris to start your own chat.