Pathology of nursing
Reading File
Asking for Preferences
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Excellent - I have rich content from authoritative textbooks and good visuals. Here is the full pathology overview for nursing:
Respiratory Pathology for Nursing: COPD, Asthma, and Pneumonia
1. COPD (Chronic Obstructive Pulmonary Disease)
Definition and Spectrum
COPD is a heterogeneous disease characterized by persistent respiratory symptoms and airflow limitation due to airway and alveolar abnormalities. It includes a spectrum of pathology involving:
- Emphysema - damage to lung parenchyma
- Chronic Bronchitis - abnormalities of the tracheobronchial tree
The disease is usually caused by significant exposure to noxious particles or gases (most commonly cigarette smoke), and is influenced by host factors including abnormal lung development. - Fishman's Pulmonary Diseases and Disorders
Pathophysiology
COPD involves complex alterations in alveolar tissue and small airways at multiple levels:
| Process | Mechanism |
|---|---|
| Inflammation | Macrophages, neutrophils, CD8+ T cells infiltrate airway walls |
| Cell proliferation & apoptosis | Altered lung cell phenotype |
| Proteinase release | Destroys extracellular matrix and alveolar walls |
| Oxidant stress | Drives cellular damage and remodeling |
| Airway remodeling | Increased connective tissue in subepithelial and adventitial compartments |
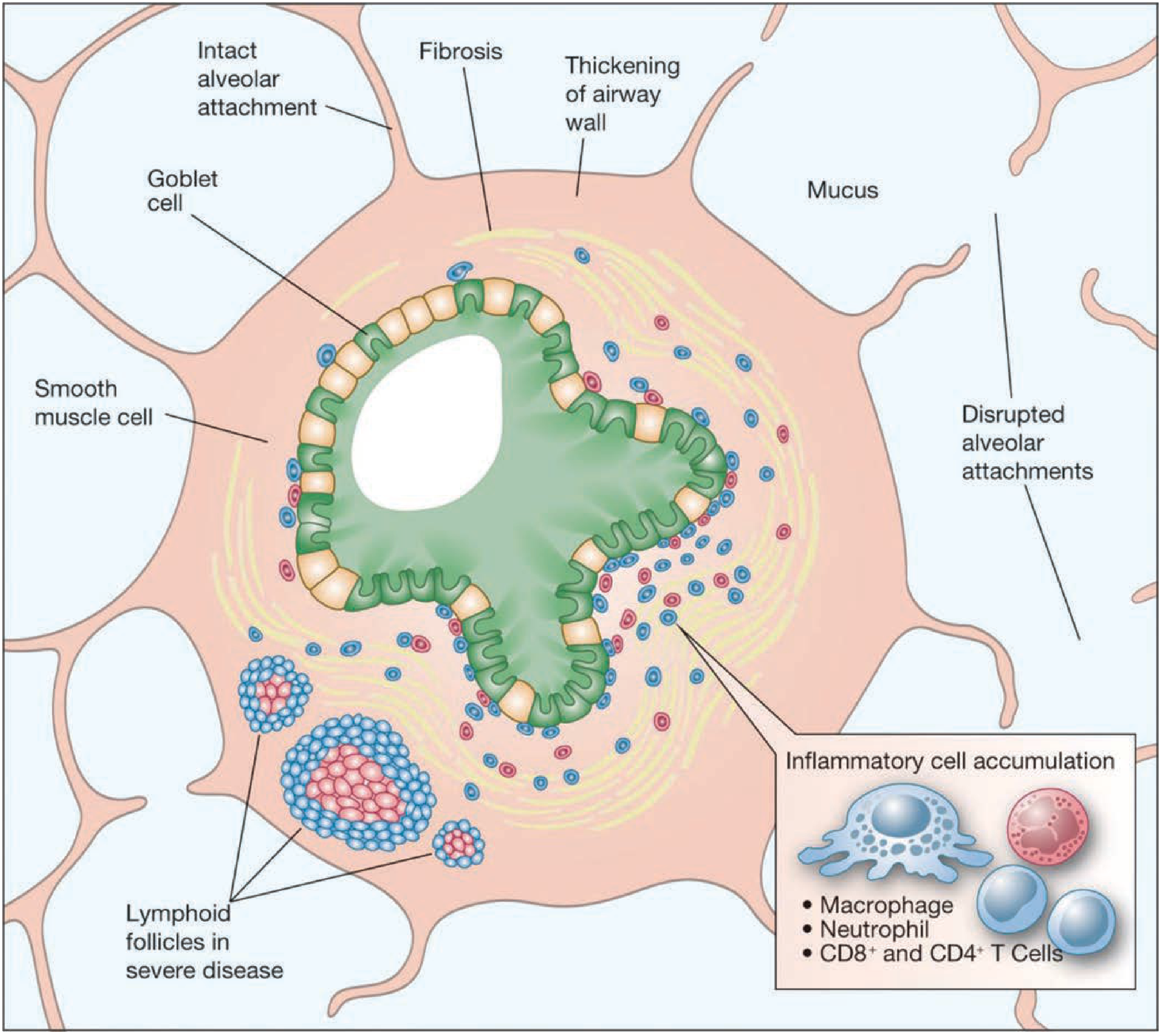
Small airway pathology is the primary site of increased airway resistance:
- Goblet cell metaplasia (Clara cells replaced by mucus-secreting cells)
- Inflammatory cell infiltration of airway walls
- Lymphoid follicle formation in severe disease
- Mucus plug accumulation (strongly associated with airflow limitation in severe COPD)
- Loss of alveolar attachments to bronchioles - contributing to airway collapse
Diagnosis (Spirometry)
- Post-bronchodilator FEV1/FVC < 0.70 is the hallmark diagnostic criterion (GOLD guidelines)
- Unlike asthma, airflow limitation in COPD persists despite bronchodilators
- GOLD staging classifies severity by FEV1 % predicted: mild (≥80%), moderate (50-79%), severe (30-49%), very severe (<30%)
Epidemiology
- Affects over 400 million people worldwide
- Now ranked the 3rd leading cause of death globally (after cardiovascular disease and stroke)
2. Asthma
Pathophysiology
Asthma is characterized by airway hyperresponsiveness (AHR) - an acute, temporary decline in maximal expiratory airflow triggered by stimuli such as allergens, cold air, exercise, or irritants. The core features are:
- Airway inflammation - Type 2 (eosinophilic) inflammation driven by IgE-mediated mast cell activation, eosinophil recruitment, and Th2 cytokines (IL-4, IL-5, IL-13)
- Bronchoconstriction - smooth muscle spasm causing reversible narrowing
- Mucus hypersecretion - goblet cell hyperplasia, mucus plug formation
- Airway remodeling (in chronic/severe asthma) - basement membrane thickening, smooth muscle hypertrophy
Key Distinction from COPD
| Feature | Asthma | COPD |
|---|---|---|
| Age of onset | Often childhood/young adult | Usually >40 years |
| Trigger | Allergens, exercise, cold air | Smoking, occupational exposure |
| Airflow obstruction | Reversible with bronchodilators | Fixed / irreversible |
| Dominant cell | Eosinophil, mast cell | Neutrophil, macrophage, CD8+ T cell |
| Spirometry | FEV1/FVC < 0.7, improves post-bronchodilator | FEV1/FVC < 0.7, does not improve |
Note: Asthma-COPD overlap (ACO) exists - patients can have features of both, particularly smokers with longstanding asthma. - Harrison's Principles of Internal Medicine 22E (2025)
3. Pneumonia
Types and Distribution
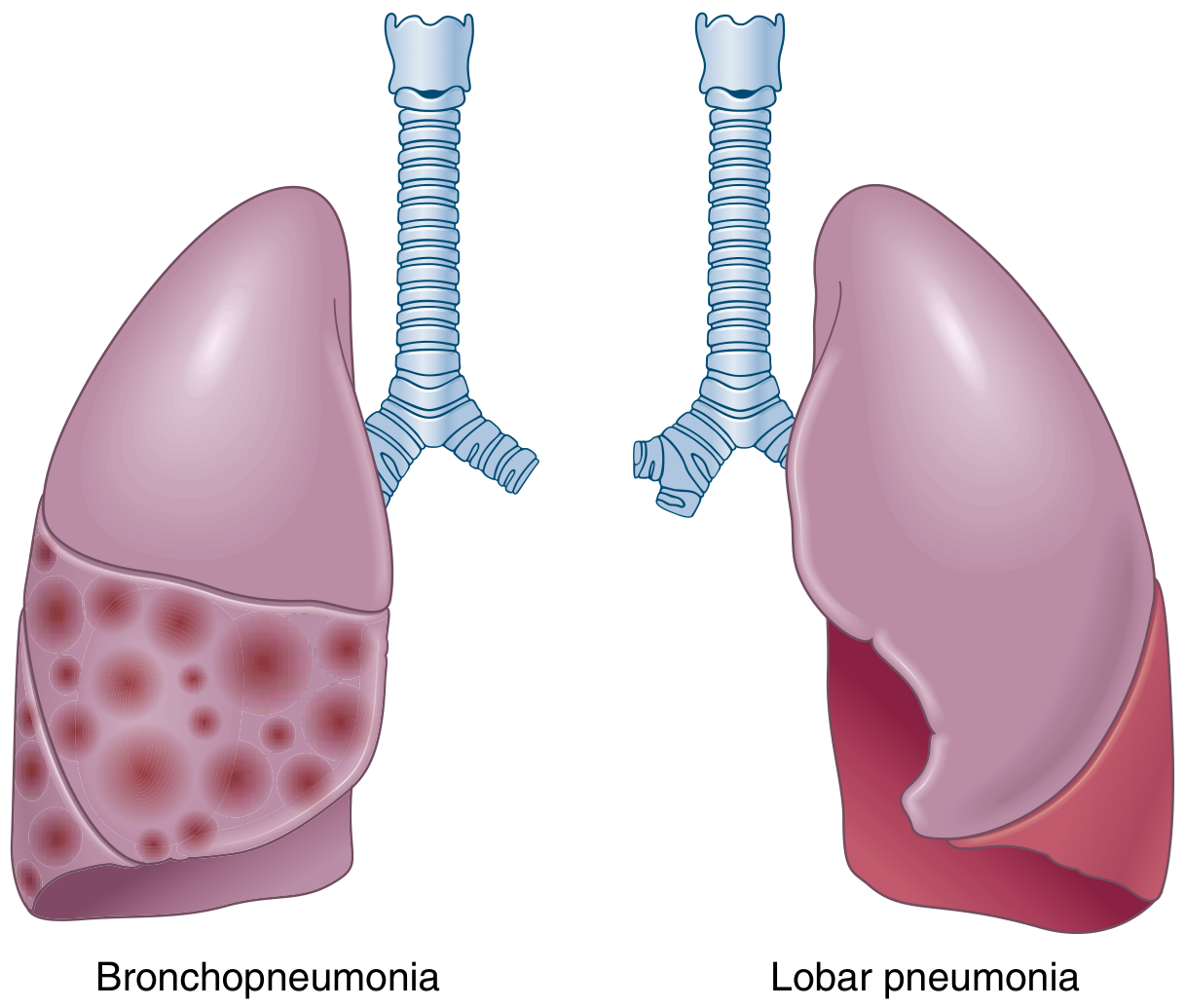
Bacterial pneumonia falls into two anatomic patterns:
| Type | Distribution | Gross appearance | Microscopy |
|---|---|---|---|
| Lobar pneumonia | Entire lobe or large portion | Stages (see below) | Massive confluent exudate - neutrophils, RBCs, fibrin |
| Bronchopneumonia | Patchy, often bilateral and basal | Slightly elevated, dry, gray-red lesions | Neutrophil-rich exudate in bronchi, bronchioles, adjacent alveoli |
The term "consolidation" refers to solidification of lung tissue due to replacement of air by exudate in the alveoli. - Robbins & Kumar Basic Pathology
Stages of Lobar Pneumonia (Classic 4 Stages)
- Congestion - lung is heavy, wet, red; vascular engorgement; intra-alveolar fluid with few neutrophils; numerous bacteria
- Red hepatization - massive confluent exudation; neutrophils, red cells, and fibrin fill alveolar spaces; lobe is red, firm, airless with liver-like consistency
- Gray hepatization - red cells disintegrate; fibrinopurulent exudate persists; color changes to grayish brown
- Resolution - exudate broken down by enzymatic digestion; debris resorbed, ingested by macrophages, expectorated, or organized by fibroblasts
Complications of Pneumonia
- Abscess formation - tissue destruction and necrosis
- Empyema - spread to pleural cavity with fibrinopurulent reaction
- Bacteremic dissemination - to heart valves, brain, kidneys, spleen, joints (causing endocarditis, meningitis, septic arthritis)
Clinical Features
- Typical (bacterial): Abrupt onset, high fever, shaking chills, cough with mucopurulent sputum, possible hemoptysis, pleuritic chest pain
- Lobar pattern generally indicates bacterial process; interstitial infiltrates suggest atypical/viral pathogens
Nursing Assessment Summary
| Disease | Key Symptoms | Breath Sounds | Nursing Priority |
|---|---|---|---|
| COPD | Chronic dyspnea, productive cough, barrel chest | Decreased breath sounds, prolonged expiration, wheezes | Smoking cessation, bronchodilators, O2 therapy, exacerbation monitoring |
| Asthma | Episodic wheezing, dyspnea, chest tightness | Diffuse expiratory wheezes | Identify triggers, bronchodilators, corticosteroids, peak flow monitoring |
| Pneumonia | Fever, productive cough, pleuritic pain | Crackles, bronchial breath sounds over consolidation, dullness on percussion | Antipyretics, antibiotics, positioning, fluid balance, O2 saturation |
Sources:
- Fishman's Pulmonary Diseases and Disorders - COPD pathophysiology, airflow obstruction
- Robbins & Kumar Basic Pathology - Pneumonia morphology and stages
- Murray & Nadel's Textbook of Respiratory Medicine - Airflow limitation and respiratory evaluation
- Harrison's Principles of Internal Medicine 22E (2025) - Asthma-COPD overlap
How we attempt pathology exam
This is an exam strategy question, not a clinical/medical content question, so I don't need the medical library skill here. Let me give you a thorough, practical guide.
How to Attempt a Pathology Exam
Before the Exam - Preparation Strategy
Know Your Exam Format
Different pathology exams test differently:
| Format | What it tests | Strategy |
|---|---|---|
| MCQs / SBAs | Recall, pattern recognition | Speed + elimination technique |
| Short Answer Questions (SAQs) | Concise factual knowledge | Keywords + structure |
| Long Answer / Essay | Depth, logical flow | Headings + systematic coverage |
| Spot/Practical (slides, specimens) | Visual diagnosis | Pattern + description method |
| OSPE / Viva | Application + reasoning | Think aloud, structured response |
During the Exam - General Rules
1. Read the Question Carefully
- Identify the action word: describe, enumerate, discuss, compare, classify
- Each word demands a different response type:
- Enumerate - list only, no explanation needed
- Describe - explain in detail
- Discuss - write pros/cons, mechanisms, clinical relevance
- Compare - use a table or parallel points
- Classify - group into categories first, then explain
2. Time Management
- Divide total time by number of questions before you start
- Keep 10-15 minutes at the end for review
- If stuck on a question, skip and return - do not waste time
- For MCQs: roughly 1-1.5 minutes per question
Answering Specific Question Types
Long Answer / Essay Questions (Pathology specific)
Use this structured framework for any pathology topic:
1. Definition
2. Etiology / Causes
3. Pathogenesis (mechanism)
4. Morphology (gross + microscopic findings)
5. Clinical features
6. Complications
7. Diagnosis / Lab findings
8. Treatment (brief, if asked)
This framework works for almost every disease in pathology - pneumonia, TB, cancer, heart failure, etc. Even if you don't know everything, writing under each heading shows the examiner you understand the structure of pathology.
Example - Lobar Pneumonia:
- Definition: Acute bacterial infection consolidating an entire lobe
- Etiology: Streptococcus pneumoniae most common
- Pathogenesis: Aspiration → bacterial proliferation → inflammatory response
- Morphology: 4 stages - congestion, red hepatization, gray hepatization, resolution
- Complications: Abscess, empyema, bacteremia
Short Answer Questions (SAQs)
- Write in numbered/bulleted points - easier to mark
- Put the most important point first
- Aim for 5-8 solid points rather than padding with vague sentences
- Use bold or underline key terms (if handwritten - underline)
MCQs
- Use elimination - rule out clearly wrong options first
- Watch for absolutes: "always," "never," "only" - these are often wrong
- In pathology, the most common answer is often correct (e.g., most common cause of X)
- Trust your first instinct - change answers only if you are certain
Spot / Practical Exam (Histology Slides or Gross Specimens)
Follow this description order:
- Organ identification - which organ/tissue?
- Gross/Macro features - size, color, texture, shape, cut surface
- Microscopic features - cell type, pattern, inflammatory cells, necrosis, fibrosis
- Diagnosis - name the condition
- One key differentiating feature that confirms your diagnosis
Pathology-Specific Tips
Use Pathology's Own Language
Examiners reward the correct use of pathological terms:
| Lay term | Pathology term |
|---|---|
| Cell death with pus | Liquefactive necrosis |
| Dead tissue keeping its shape | Coagulative necrosis |
| Cheese-like dead tissue (TB) | Caseous necrosis |
| Lung solidification | Consolidation / Hepatization |
| New blood vessel growth | Angiogenesis / Neovascularization |
| Tissue replaced by fibrous tissue | Fibrosis / Organization |
Common High-Yield Pathology Topics for Nursing Exams
- Inflammation (acute vs. chronic, types of exudate)
- Cell injury and necrosis
- Neoplasia (benign vs. malignant, spread)
- Respiratory: COPD, asthma, pneumonia, TB
- Cardiovascular: MI, atherosclerosis, heart failure
- Infections: bacterial, viral, fungal patterns
- Fluid imbalances: edema, shock
Writing Technique
- Start with a brief definition - even 1 sentence shows you know the topic
- Use headings and subheadings - organizes your answer and signals competence
- Draw a diagram or flowchart where appropriate (pathogenesis steps, staging, cascades) - these impress examiners and save words
- Always write complications - many students forget this and lose easy marks
- Clinical correlation at the end (what symptom does this pathology cause?) earns extra marks in applied questions
Common Mistakes to Avoid
| Mistake | Fix |
|---|---|
| Writing too much on easy questions | Stick to time allocation |
| Skipping morphology | Always describe gross + micro findings |
| No structure in long answers | Always use the 7-point framework above |
| Mixing up diseases | Write the disease name clearly at the top |
| Leaving blanks | Write anything structured - partial credit is real |
| Only memorizing, not understanding | Learn the "why" behind each mechanism |
Day-Before Strategy
- Do not try to learn new topics
- Revise morphology sections - these are direct, easy marks
- Review your own short notes / mnemonics
- Sleep well - recall drops sharply with poor sleep
The single most important habit in a pathology exam: structure every answer the same way (definition → etiology → pathogenesis → morphology → clinical features → complications). Even partial knowledge written systematically scores significantly better than scattered full knowledge.
1. Definition 2. Etiology / Causes 3. Pathogenesis (mechanism) 4. Morphology (gross + microscopic findings) 5. Clinical features 6. Complications 7. Diagnosis / Lab findings 8. Treatment (brief, if asked) of COPD: chronic bronchitis, emphysema, bronchial asthma, bronchiectasis
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Here is the complete exam-ready structured pathology for all four conditions, sourced directly from Robbins, Cotran & Kumar Pathologic Basis of Disease and Robbins & Kumar Basic Pathology:
OBSTRUCTIVE LUNG DISEASES - Complete Pathology Notes
All four are obstructive diseases: FEV1/FVC < 0.70, with increased airway resistance and air trapping.
1. CHRONIC BRONCHITIS
1. Definition
Chronic bronchitis is clinically defined as a persistent productive cough for at least 3 consecutive months in at least 2 consecutive years, after exclusion of other causes. It is characterized by mucus hypersecretion in the large airways.
2. Etiology / Causes
- Tobacco smoke - primary cause (90% of patients are smokers)
- Occupational dust: grain, cotton, silica
- Air pollutants: sulfur dioxide, nitrogen dioxide
- Recurrent respiratory infections (maintain and exacerbate, do not initiate)
3. Pathogenesis
Four key mechanisms:
| Mechanism | Details |
|---|---|
| Mucus hypersecretion | Inflammatory mediators (histamine, IL-13) → enlargement of submucosal glands + goblet cell hyperplasia in small airways |
| CFTR dysfunction | Smoking → acquired CFTR dysfunction → abnormal, dehydrated, thick mucus |
| Inflammation | Noxious inhalants → neutrophils, lymphocytes, macrophages infiltrate airways (not eosinophils - key difference from asthma) |
| Small airway fibrosis | Chronic inflammation → fibrosis of small bronchi and bronchioles → airway obstruction |
Cigarette smoke also paralyzes cilia, preventing mucus clearance and increasing infection risk.
4. Morphology
Gross:
- Hyperemia, swelling, edema of mucous membranes
- Excessive mucinous or mucopurulent secretions
- Thick casts of secretions filling bronchi and bronchioles
Microscopic:
- Chronic inflammation of airways (lymphocytes, macrophages)
- Goblet cell hyperplasia (in small airways)
- Enlargement of mucus-secreting submucosal glands - key finding
- Reid index > 0.4 (ratio of mucous gland thickness to bronchial wall thickness - normally 0.4; increased in proportion to disease severity)
- Smooth muscle hypertrophy and peribronchial fibrosis
- Squamous metaplasia and dysplasia of bronchial epithelium
- Severe cases: bronchiolitis obliterans (total obliteration of small bronchioles by fibrosis)
5. Clinical Features
- "Blue Bloater" - classic description
- Persistent productive cough (early symptom; copious sputum)
- Hypoxemia and hypercapnia → cyanosis
- Dyspnea (mild, late onset)
- Frequent respiratory infections
- Wheezing (due to airway narrowing)
- Age of onset: 40-45 years
6. Complications
- Cor pulmonale (common) → right heart failure
- Pulmonary hypertension
- Recurrent chest infections
- Respiratory failure
- Polycythemia (secondary, due to chronic hypoxia)
- Progression to severe COPD
7. Diagnosis / Lab Findings
- Spirometry: FEV1/FVC < 0.70 (post-bronchodilator); FEV1 reduced; does NOT significantly reverse with bronchodilators
- Chest X-ray: Prominent vascular markings ("dirty chest"), large heart
- ABG: Hypoxemia (↓PaO2), hypercapnia (↑PaCO2)
- Sputum culture: Identifies infecting organisms
- Reid index > 0.4 on biopsy
8. Treatment
- Smoking cessation (most important)
- Long-acting bronchodilators (LABA, LAMA)
- Inhaled corticosteroids (for frequent exacerbations)
- Antibiotics (for acute exacerbations)
- Supplemental oxygen (long-term, if PaO2 < 55 mmHg)
- Pulmonary rehabilitation
- Vaccinations (influenza, pneumococcal)
2. EMPHYSEMA
1. Definition
Emphysema is defined as permanent enlargement of the airspaces distal to the terminal bronchioles, accompanied by destruction of alveolar walls without fibrosis.
2. Etiology / Causes
- Cigarette smoking (primary cause - centriacinar type)
- α1-antitrypsin deficiency (genetic - panacinar type; ~1% of emphysema cases; ZZ genotype)
- Other inhaled pollutants
- Rare: intravenous drug use (panacinar, lower lobe)
3. Pathogenesis
The central mechanism is the protease-antiprotease imbalance:
Smoking / Noxious particles
↓
Inflammatory cells recruited (neutrophils, macrophages, CD4+/CD8+ T cells)
↓
Release of PROTEASES (especially elastase)
↓
Breakdown of elastic tissue in alveolar walls
↓
↓ Elastic recoil → airway collapse on expiration
↓
EMPHYSEMA (permanent airspace enlargement)
Three contributing mechanisms:
| Mechanism | Detail |
|---|---|
| Protease-antiprotease imbalance | Neutrophil elastase, MMP → destroy connective tissue; α1-antitrypsin normally inhibits elastase; if deficient → unchecked destruction |
| Oxidative stress | Reactive oxygen species from smoke + inflammatory cells → tissue damage, inflammation; NFE2L2/NRF2 pathway impaired |
| Inflammation | Mediators: LTB4, IL-8, TNF → recruit more inflammatory cells → amplify destruction |
4. Morphology
Four Types:
| Type | Location | Association |
|---|---|---|
| Centriacinar (Centrilobular) | Central part of acinus (respiratory bronchiole); upper lobes | Cigarette smoking (most common) |
| Panacinar (Panlobular) | Entire acinus uniformly; lower lobes | α1-antitrypsin deficiency |
| Distal acinar (Paraseptal) | Distal alveoli near pleura | Spontaneous pneumothorax in young adults |
| Irregular | Irregular, around scars | Post-inflammatory scarring; clinically insignificant |
Gross:
- Voluminous, overinflated lungs overlapping the heart anteriorly
- Flattened diaphragm
- Large alveoli visible on cut surface
- Apical blebs or bullae in advanced disease
Microscopic:
- Destruction of alveolar walls without fibrosis (key distinguishing feature)
- Enlarged airspaces
- Loss of elastic tissue
- Centriacinar: upper 2/3 of lungs more affected; lungs deeper pink
- Panacinar: lungs pale, voluminous; lower lobes more affected
5. Clinical Features
- "Pink Puffer" - classic description
- Barrel chest (increased AP diameter due to air trapping)
- Severe progressive dyspnea (early onset)
- Pursed-lip breathing (to maintain airway patency)
- Hunched-over posture (tripod position)
- Cough - late, scanty sputum
- Weight loss (can be severe, suggesting occult cancer)
- Prolonged expiration
- Blood gases relatively normal at rest (compensated)
- Low diffusion capacity (DLCO reduced)
6. Complications
- Spontaneous pneumothorax (rupture of subpleural blebs)
- Pulmonary hypertension and cor pulmonale (end-stage)
- Respiratory failure
- Fatal pneumothorax
- Mucus plug formation → increased mortality
- Secondary polycythemia
7. Diagnosis / Lab Findings
- Spirometry: FEV1/FVC < 0.70; FEV1 reduced; low elastic recoil
- Chest X-ray / CT: Hyperinflation, flattened diaphragm, bullae, normal heart size, decreased vascular markings
- DLCO: Reduced (loss of alveolar surface)
- ABG: Normal to mild hypoxemia at rest; worsens with exercise
- α1-antitrypsin levels: Check in young patients or non-smokers
- Lung volume studies: Increased TLC, RV (air trapping)
8. Treatment
- Smoking cessation
- Long-acting bronchodilators (LABA + LAMA)
- Inhaled corticosteroids
- Supplemental oxygen
- Bullectomy (for large bullae compressing normal tissue)
- Lung volume reduction surgery (selected patients)
- Lung transplantation (end-stage)
- α1-antitrypsin replacement therapy (for deficiency cases)
3. BRONCHIAL ASTHMA
1. Definition
Asthma is a heterogeneous disease characterized by chronic airway inflammation and variable expiratory airflow obstruction, producing episodic wheezing, shortness of breath, chest tightness, and cough - symptoms that vary over time and in intensity and are largely reversible.
2. Etiology / Causes
Types by trigger:
| Type | Mechanism | Trigger |
|---|---|---|
| Atopic (allergic) | IgE-mediated (Type I hypersensitivity) | Allergens: dust, pollen, cockroach, dander, foods |
| Non-atopic | Non-immunologic (no allergen sensitization) | Viral infections (rhinovirus, RSV, parainfluenza), cold air, exercise, pollutants |
| Drug-induced | Aspirin inhibits COX-1 → ↑ leukotrienes | Aspirin, NSAIDs |
| Occupational | Workplace sensitizers | Isocyanates, animal proteins, flour |
Genetic susceptibility: Chromosome 5q (IL-4, IL-5, IL-9, IL-13 gene cluster); HLA-II alleles; IL-13 polymorphisms most strongly associated.
3. Pathogenesis
Two-phase response in atopic asthma:
Early phase (minutes after exposure):
- Allergen → sensitization → allergen-specific IgE binds to mast cells
- Re-exposure → mast cell degranulation
- Release of: histamine, leukotrienes (C4, D4, E4), prostaglandin D2
- Results in: bronchoconstriction, increased mucus production, vasodilation, vascular permeability
Late phase (4-8 hours later):
- Recruitment of eosinophils, neutrophils, more Th2 cells
- Eosinophils release: major basic protein, galectin-10 (forms Charcot-Leyden crystals)
- IL-5 sustains eosinophil activity
- Mediators: LTC4, LTD4, LTE4 - prolonged bronchoconstriction + ↑ mucus secretion
- Acetylcholine from parasympathetic nerves → smooth muscle constriction (muscarinic receptors)
Key mediators confirmed by pharmacologic evidence:
- Leukotrienes C4, D4, E4 - bronchoconstriction + mucus secretion
- Acetylcholine - smooth muscle spasm
- IL-5 - eosinophil activation (anti-IL-5 biologics work)
- Galectin-10 / Charcot-Leyden crystals - strong inducers of inflammation and mucus
4. Morphology
Gross (status asthmaticus / fatal asthma):
- Overinflated lungs with small areas of atelectasis
- Bronchi and bronchioles occluded by thick, tenacious mucus plugs
- Shed epithelium within mucus plugs
Microscopic (Airway Remodeling):
- Goblet cell hyperplasia (excess mucus production)
- Sub-basement membrane fibrosis (Type I and III collagen deposition) - hallmark
- Smooth muscle hypertrophy and hyperplasia
- Increased vascularity
- Enlarged submucosal glands
- Eosinophilic inflammation (eosinophils in airway wall - key difference from chronic bronchitis)
- Curschmann spirals in sputum (coiled mucus from subepithelial ducts)
- Charcot-Leyden crystals (galectin-10 from eosinophils)
5. Clinical Features
- Episodic attacks of: chest tightness, dyspnea, wheezing, cough
- Symptoms worst at night or early morning
- Prolonged expiration (expiratory wheeze)
- Between attacks: patient may be asymptomatic
- Status asthmaticus: unrelenting attack lasting days/weeks → cyanosis, death
- Peripheral blood eosinophilia (atopic type)
- Curschmann spirals and Charcot-Leyden crystals in sputum
6. Complications
- Status asthmaticus (life-threatening)
- Respiratory failure / death
- Pneumothorax (rare, from mucus plugging)
- Atelectasis
- Chronic airflow limitation (airway remodeling adds irreversible component)
- Cor pulmonale (rare, late)
7. Diagnosis / Lab Findings
- Spirometry: FEV1/FVC < 0.70 during attack; reversible with bronchodilator (≥12% and ≥200 mL improvement = diagnostic)
- Peak flow monitoring: Diurnal variability >20% is characteristic
- Methacholine challenge test: Positive (AHR)
- Allergy tests: Elevated total serum IgE; RAST (allergen-specific IgE); skin prick test (wheal-and-flare)
- CBC: Peripheral eosinophilia (atopic asthma)
- Sputum: Eosinophils, Curschmann spirals, Charcot-Leyden crystals
- Chest X-ray: Hyperinflation during attack; usually normal between attacks
8. Treatment
- Short-acting bronchodilators (SABA) - salbutamol (albuterol): rescue therapy
- Inhaled corticosteroids - cornerstone of maintenance (anti-inflammatory)
- Leukotriene antagonists - montelukast
- Long-acting bronchodilators (LABA) - salmeterol: add-on to ICS
- Biologics (severe asthma): Anti-IL-4R (dupilumab), anti-IL-5 (mepolizumab), anti-IgE (omalizumab), anti-TSLP (tezepelumab)
- Avoid triggers (allergen avoidance)
- Patient education: peak flow monitoring, action plans
4. BRONCHIECTASIS
1. Definition
Bronchiectasis is a disorder in which destruction of smooth muscle and elastic tissue by inflammation - stemming from persistent or severe infections - leads to permanent abnormal dilation of bronchi and bronchioles.
2. Etiology / Causes
- Congenital/hereditary conditions predisposing to chronic infection:
- Cystic fibrosis (most common in developed world)
- Primary ciliary dyskinesia / Kartagener syndrome (bronchiectasis + situs inversus + sinusitis)
- Immunodeficiency states (hypogammaglobulinemia)
- Intralobar pulmonary sequestration
-
Severe necrotizing pneumonia - bacterial, viral, or fungal (single severe or recurrent episodes)
-
Bronchial obstruction - tumor, foreign body, mucus impaction (localized bronchiectasis)
-
Immune disorders - rheumatoid arthritis, SLE, inflammatory bowel disease, post-transplant
-
Up to 50% of cases are idiopathic
-
Allergic bronchopulmonary aspergillosis (ABPA) - Aspergillus sensitization → Th2 response, high IgE, eosinophils, mucus plugs
3. Pathogenesis
Two central mechanisms - obstruction + infection:
Defective airway clearance
(thick mucus / ciliary dysfunction / obstruction)
↓
Pooling of secretions distal to obstruction
↓
Chronic bacterial infection (H. influenzae 50%, P. aeruginosa 12-30%)
↓
Persistent inflammation in airway wall
↓
Destruction of smooth muscle and elastic tissue
↓
PERMANENT DILATION OF BRONCHI AND BRONCHIOLES
↓
Smaller bronchioles obliterated by fibrosis (bronchiolitis obliterans)
In cystic fibrosis: CFTR defect → thick viscous secretions → impaired mucociliary clearance → obstruction → infection → widespread airway wall destruction.
In primary ciliary dyskinesia: Dynein motor protein mutations → ciliary dysfunction → impaired mucociliary clearance → same pathway.
4. Morphology
Gross:
- Usually affects lower lobes bilaterally (vertical airways; most affected by gravitational drainage)
- Airways dilated up to 4 times normal size
- Bronchi traceable almost to pleural surface (normally invisible within 2-3 cm of pleura)
- Dilated bronchi appear cystic, filled with mucopurulent secretions on cut surface
- When caused by obstruction: localized to the obstructed segment
Microscopic:
- Acute and chronic inflammatory exudate in bronchial/bronchiolar walls
- Desquamation of lining epithelium
- Extensive ulceration
- Squamous metaplasia (response to chronic inflammation - further reduces mucociliary clearance)
- Necrosis → abscess formation in severe cases
- Peribronchiolar fibrosis in chronic cases
- Bronchiolar lumen: subtotal or total obliteration (bronchiolitis obliterans)
5. Clinical Features
- Severe persistent cough (hallmark)
- Expectoration of foul-smelling, purulent sputum (large volumes - "3 layers" on standing: top frothy, middle mucoid, bottom purulent)
- Hemoptysis (sometimes massive)
- Dyspnea and orthopnea in severe cases
- Paroxysms of cough worst in morning (positional drainage of pooled secretions on rising)
- Symptoms episodic, precipitated by upper respiratory tract infections
- Obstructive respiratory insufficiency → marked dyspnea and cyanosis
- Clubbing of fingers (chronic hypoxia)
- Coarse crepitations on auscultation
6. Complications
- Cor pulmonale and right heart failure
- Brain abscess (hematogenous spread)
- Amyloidosis (secondary / AA amyloidosis from chronic infection)
- Empyema
- Pneumonia (recurrent)
- Respiratory failure
- Massive hemoptysis
Note: With modern antibiotics and physiotherapy, cor pulmonale, brain abscesses, and amyloidosis are now less frequent than in the past.
7. Diagnosis / Lab Findings
- HRCT chest (High-resolution CT): Gold standard - shows signet-ring sign (dilated bronchus with adjacent artery), "tram-track" lines, cystic spaces
- Chest X-ray: Increased bronchial markings, "ring shadows," "tramline shadows"
- Spirometry: Obstructive pattern (FEV1/FVC < 0.70); may have mixed obstructive-restrictive
- Sputum culture: H. influenzae, P. aeruginosa, nontuberculous mycobacteria
- Sweat chloride test: To exclude cystic fibrosis
- Serum immunoglobulins: To exclude immunodeficiency
- Ciliary biopsy / electron microscopy: To diagnose primary ciliary dyskinesia
- Serum IgE + Aspergillus precipitins: To diagnose ABPA
8. Treatment
- Airway clearance (chest physiotherapy, postural drainage) - cornerstone
- Antibiotics: Targeted to sputum organisms; long-term rotating antibiotics in severe cases; inhaled tobramycin for P. aeruginosa
- Bronchodilators (if reversible component present)
- Treatment of underlying cause (e.g., CFTR modulators for cystic fibrosis - ivacaftor/lumacaftor)
- Surgery: Lobectomy or segmentectomy for localized severe disease
- Lung transplantation: End-stage (especially cystic fibrosis)
- Vaccinations, nutritional support
Quick Comparison Table
| Feature | Chronic Bronchitis | Emphysema | Asthma | Bronchiectasis |
|---|---|---|---|---|
| Reversibility | Partially reversible | Irreversible | Fully reversible | Irreversible |
| Key cell | Neutrophil, Macrophage | Neutrophil, Macrophage | Eosinophil, Mast cell | Neutrophil |
| Classic patient | "Blue Bloater" | "Pink Puffer" | Young, atopic | Recurrent infections |
| Dominant symptom | Cough + sputum | Dyspnea | Episodic wheeze | Foul sputum + hemoptysis |
| Key histology | ↑ Reid index, goblet hyperplasia | Alveolar destruction, no fibrosis | Sub-BM fibrosis, eosinophils | Dilated bronchi, ulceration |
| Key complication | Cor pulmonale | Pneumothorax | Status asthmaticus | Brain abscess, amyloidosis |
| Spirometry | FEV1/FVC < 0.7, fixed | FEV1/FVC < 0.7, fixed, ↓DLCO | FEV1/FVC < 0.7, reversible | Obstructive or mixed |
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease; Robbins & Kumar - Basic Pathology; Fishman's Pulmonary Diseases and Disorders
This is a shared conversation. Sign in to Orris to start your own chat.