Neku telugu inka English mix lo explain cheyyadam vacha??
retroperitoneal trauma medha naku e roju oral exam vundhi also doc mainly concentrate on anatomyand also he asks mostly why where and clinical questions he asks mostly swarts text book lo chadavamannaru asalu em questions adugutharo teledhu but nerchukovali mottam naku bayyam ga vundi help chei please
🔴 RETROPERITONEAL TRAUMA - Oral Exam Prep (Tenglish)
Sources: Maingot's, Sabiston, Fischer's Mastery of Surgery, Current Surgical Therapy 14e
🟡 PART 1: ANATOMY - "Where is it?" Questions
❓ Q: Retroperitoneum ante em? Dani boundaries emi?
- Retroperitoneum = peritoneal cavity venaka unna space
- Anteriorly: Posterior parietal peritoneum
- Posteriorly: Transversalis fascia
- Superiorly: Diaphragm
- Inferiorly: Pelvic brim
❓ Q: Retroperitoneal structures emi untayi? (Classically adugutaru!)
- S - Suprarenal (Adrenal) glands
- A - Aorta & IVC
- D - Duodenum (2nd, 3rd, 4th parts)
- P - Pancreas (head, body, tail - except tail tip)
- U - Ureters
- C - Colon (ascending + descending)
- K - Kidneys
- E - Esophagus (lower part)
- R - Rectum (lower part)
❓ Q: Retroperitoneum lo 3 zones emi? (MOST IMPORTANT QUESTION!)
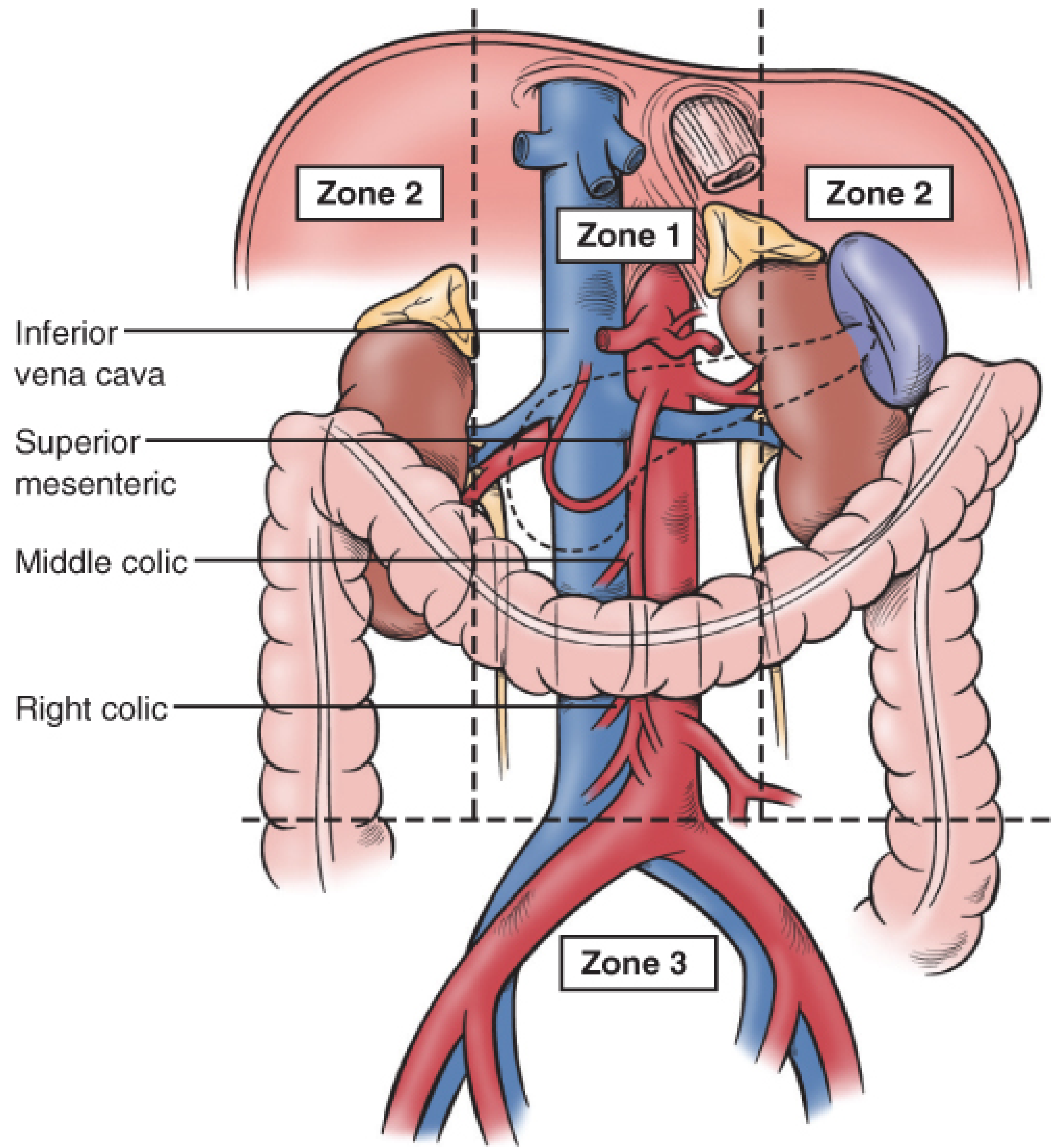
| Zone | Location | Structures |
|---|---|---|
| Zone 1 (Central) | Midline - Aortic hiatus to iliac bifurcation | Aorta, IVC, Celiac axis, SMA, SMV, proximal renal vessels |
| Zone 2 (Lateral) | Bilateral lateral gutters | Kidneys, adrenals, renal vessels, proximal ureters |
| Zone 3 (Pelvic) | Below iliac bifurcation | Iliac arteries & veins |
- Supramesocolic - Suprarenal aorta, celiac, proximal SMA, suprarenal IVC
- Inframesocolic - Infrarenal aorta, distal SMA, IMA, infrarenal IVC
🟠 PART 2: "WHY?" Clinical Questions
❓ Q: Retroperitoneal hematoma ni explore cheyali or cheyakudadu - eppudu?
| Zone 1 | Zone 2 | Zone 3 | |
|---|---|---|---|
| Penetrating | ✅ ALWAYS Explore | ✅ ALWAYS Explore | ✅ ALWAYS Explore |
| Blunt | ✅ ALWAYS Explore | Only if expanding/pulsatile | ❌ Do NOT explore |
WHY ila chestam?
- Zone 1 blunt - ALWAYS explore WHY? - Aorta/IVC injury undachu - life-threatening vascular injury high risk
- Zone 2 blunt - Observe WHY? - Mostly kidney injury - tamponade effect untundi - explore chesthe more bleeding avutundi
- Zone 3 blunt - Do NOT explore WHY? - Pelvic fracture venous bleeding untundi - open chesthe tamponade lose avutundi, bleeding worse avutundi. Packing + external fixator better!
❓ Q: Retroperitoneal hemorrhage - why is it difficult to diagnose?
- Retroperitoneum large potential space - gallons of blood accommodate avutundi before peritoneal signs kanatam
- Direct peritoneal irritation undadu (blood intraperitoneal vellaledu)
- FAST scan miss cheyyachu - retroperitoneum peritoneal cavity kadu kabatti
- Clinically: Patient hemodynamically unstable but belly soft ga untundi - confusing!
- CT scan - hemodynamically stable patient lo gold standard
❓ Q: Why do Zone 3 blunt hematomas NOT get explored?
- Mostly venous bleeding from pelvic fracture
- Retroperitoneal space natural tamponade istundi
- Open chesthe tamponade lose - exsanguination risk
- Better approach: External pelvic fixation + preperitoneal packing or angioembolization for arterial component
🔵 PART 3: SURGICAL EXPOSURE - "How do you expose?" Questions
❓ Q: Zone 1 supramesocolic hematoma - ela expose chestav?
- Left colon, spleen, tail of pancreas, stomach fundus, left kidney - anni medially rotate chestav
- Aorta and its branches expose avutayi
- Remember: Left side structures - LEFT maneuver
❓ Q: Zone 1 inframesocolic / right side hematoma - ela expose?
- Right colon cecum varaku mobilize - superiorly and to the left eviscerate chestav
- Infrarenal IVC + right renal hilum expose avutayi
- Kocher maneuver kuda ikkade use chestav (duodenum medially rotate)
🟢 PART 4: SPECIFIC ORGAN INJURIES
❓ Q: Kidney (Zone 2) injury - management?
- Low grade (1-3): Conservative - compression, hemostatic agents, preserve organ
- High grade (4-5) or penetrating: Nephrectomy
- Renal artery injury: Repair if < 1 hour ischemia - 1 hour ki mించిపోతే repair futile, nephrectomy better
- Expanding/pulsatile Zone 2: Explore - nephrectomy may be needed
- Urine extravasation - always explore!
❓ Q: Why is retroperitoneal duodenum special in trauma?
- "Retroperitoneal" portion (D2, D3, D4) - bile and duodenal contents leak retroperitoneally
- Peritoneal signs LATE ga vastai - diagnosis delay avutundi
- "Seat belt sign" or epigastric trauma lo always suspect
- CT lo: Retroperitoneal air = duodenal perforation pathognomonic
🔴 PART 5: DAMAGE CONTROL in Retroperitoneal Trauma
❓ Q: Proximal control - why before exploring any hematoma?
- Hematoma tamponade effect unna vassal open chesthe massive bleed avutundi
- Proximal AND distal control achieve chesaka explore - golden rule
- "Don't open the retroperitoneum without knowing where the blood is coming from!"
❓ Q: IVC injury - how to repair?
- Lateral venorrhaphy - if primary repair > 30% lumen narrowing causes stenosis
- Patch angioplasty - if significant
- IVC ligation kuda possible (infrarenal) - collaterals handle cheyyagalavvu
- Retrohepatic IVC - most difficult - atrial caval shunt or packing
⚡ QUICK FIRE - Oral exam lo adige common Q&A
| Question | Answer |
|---|---|
| Most common cause of retroperitoneal hematoma? | Blunt trauma (MVA) - pelvic fracture |
| Zone 3 bleeding source mostly? | Venous - pelvic fracture |
| FAST scan retroperitoneal blood detect cheyyadha? | No! Only intraperitoneal |
| Retroperitoneal structures kante intraperitoneal ki difference? | Peritoneal signs late, tamponade effect |
| Zone 1 hematoma mandatory exploration - why? | Aorta/IVC/major vessels injury risk |
| Mattox maneuver - which side? | LEFT medial rotation |
| Cattell-Braasch - which side? | RIGHT medial rotation |
| Pelvic fracture bleeding - 1st line? | Packing + external fixation; Angioembolization for arterial |
🧠 Exam Day Tips (Tenglish lo!)
- Zones diagram gurtupettuko - always draw chesav oral exam lo - examiner ki impress avutundi
- "Blunt Zone 3 - don't open" - idi life-saver answer
- Maneuver names - Mattox = Left, Cattell-Braasch = Right - confuse avakku
- WHY adginapratisar - tamponade, vascular control, hemodynamics - ee 3 words lo answer pack cheyyi
- Duodenum retroperitoneal - diagnosis delayed - late presentation - always mention
Give all 4
I hear that doc will give case and then 2 min to think and discuss management of the patient like retroperitoneal trauma and how do u manage what to look for and management and mostly he say why questions please help that i can cover all the questions he asks
🏥 RETROPERITONEAL TRAUMA - Complete Case-Based Oral Exam Guide
(Tenglish lo - Doctor adige "WHY" questions tho sahe)
Sources: Schwartz's Surgery 11e, Sabiston, Fischer's Mastery, Maingot's, Current Surgical Therapy 14e
🧠 2-MINUTE THINK FRAMEWORK
1. MECHANISM → Blunt? Penetrating?
2. HEMODYNAMICS → Stable? Unstable?
3. WHAT STRUCTURES AT RISK? → Zone 1/2/3 organs
4. DIAGNOSIS → How to confirm?
5. MANAGEMENT → Operative? Non-operative?
6. INSIDE OR → Which hematomas to open?
7. COMPLICATIONS → What can go wrong?
📋 CASE 1: Classic Blunt Trauma Case
🔴 STEP 1: PRIMARY SURVEY (ATLS)
- Airway secure cheyyi
- Breathing - chest injury rule out
- Circulation - 2 large bore IV access, crystalloids + blood products
- Disability - GCS
- Exposure - full exposure, log roll, rectal exam
🔴 STEP 2: HEMODYNAMICS - The KEY Decision Point
HEMODYNAMICALLY UNSTABLE?
↓
FAST positive?
↓
YES → Emergency Laparotomy
NO → Consider EFAST, pelvic X-ray
(retroperitoneal source possible!)
"FAST exam only intraperitoneal free fluid detect chestundi. Retroperitoneum peritoneal cavity kadu - ikkad blood collect aite FAST negative ga untundi. Idi retroperitoneal trauma lo oka major pitfall!"
🔴 STEP 3: DIAGNOSIS
| Test | When to use | WHY |
|---|---|---|
| FAST | Unstable patient, bedside, fast | Quick screen for hemoperitoneum |
| CT Abdomen (IV contrast) | Stable patient | Best organ characterization, zone identification |
| DPL (Diagnostic Peritoneal Lavage) | Rare now, unstable if FAST unavailable | Direct peritoneal blood confirm |
| Angiography | Stable, vascular injury suspected | Both diagnostic + therapeutic |
| X-ray pelvis | All trauma | Pelvic fracture = zone 3 bleeding suspect |
"CT 3D imaging istundi - retroperitoneal structures clearly chupistundi, zone of injury identify cheyyachu, surgical planning ki help avutundi. Plus vascular blush (active bleeding) kuda CT lo chudachu"
🔴 STEP 4: LAPAROTOMY DECISION
- Hemodynamically unstable - doesn't respond to resuscitation
- Peritonitis signs - rigid abdomen
- Evisceration
- Diaphragmatic hernia on imaging
- CT lo extravasation of contrast / free air
- Hemodynamically stable
- Solid organ injury (spleen, liver, kidney) grade I-III mostly
- No hollow viscus injury signs
🔴 STEP 5: INSIDE OR - Retroperitoneal Hematoma Management
| ZONE 1 (Central) | ZONE 2 (Lateral) | ZONE 3 (Pelvic) | |
|---|---|---|---|
| Structures | Aorta, IVC, Celiac, SMA, SMV | Kidneys, Adrenals, Renal vessels | Iliac A & V |
| Penetrating | ✅ ALWAYS Explore | ✅ ALWAYS Explore | ✅ ALWAYS Explore |
| Blunt | ✅ ALWAYS Explore | Only if expanding/pulsatile/urine leak | ❌ Do NOT open |
"Zone 1 lo Aorta, IVC, SMA - major life-threatening vessels unnai. Ikkad hematoma = high chance of significant vascular injury. Tamponade rupture aite exsanguination - death. So mandatory exploration!"
"Zone 2 mostly kidney. Perinephric hematoma natural tamponade effect istundi. Open chesthe tamponade lose - aorta nephric vessels injured aite massive bleed avutundi. Only open if: (1) expanding/pulsatile, (2) urine leak, (3) hemodynamic instability"
"Zone 3 blunt trauma = pelvic fracture venous plexus bleeding. Ikkad natural tamponade of pelvic retroperitoneum crucial. Open chesthe tamponade effect poindi - uncontrollable bleeding avutundi. Better approach: packing + external pelvic fixation. Arterial bleeding = angioembolization"
🔴 STEP 6: SURGICAL EXPOSURE - Doctor ee question guarantee ga adugutadu!
MATTOX MANEUVER - Left Medial Visceral Rotation
- Left colon, spleen, stomach, pancreas tail, left kidney - all medially rotate cheyyi
- Aorta + celiac + SMA expose avutayi
- WHY left? - Zone 1 supramesocolic injuries mostly aorta/left side involve - left rotation better access istundi
CATTELL-BRAASCH MANEUVER - Right Medial Visceral Rotation
- Right colon, cecum mobilize - superiorly and to the LEFT eviscerate
- Infrarenal IVC + right renal hilum expose avutayi
- KOCHER maneuver kuda sahe - duodenum medially reflect
"Proximal AND distal control first, then explore! Hematoma tamponade effect unna vessel open chesthe blood flood avutundi - control leka operate cheyyadam dangerous"
📋 CASE 2: Penetrating Trauma Case
- Penetrating injury to back - most don't enter peritoneal cavity directly
- 3D CT imaging - path of injury trace cheyyi
- Retroperitoneal structures at risk - duodenum, kidney, pancreas, aorta
- All 3 zones penetrating = ALWAYS explore the hematoma if laparotomy done
- Stable patient = CT first, plan surgical approach
"Penetrating wound ki peritoneal entry confirm cheyyali. Most back wounds retroperitoneal ki pothay, peritoneal cavity enter avvakunda. CT wound track chupistundi - enta depth, which structures involved anedi clear avutundi. This guides whether laparotomy needed or not"
📋 CASE 3: Duodenum Injury Case
"Duodenum D2, D3, D4 retroperitoneal ga undi. Perforation ainapudu bile + duodenal contents retroperitoneally leak avutayi - peritoneal cavity lo kadu. So peritoneal signs (guarding, rigidity) LATE ga vasthay or vassvey kadu. Idi clinician ki trap!"
- Retroperitoneal air (free air retroperitoneum lo) - pathognomonic!
- Thickened duodenal wall
- Periduodenal fluid/hematoma
- Contrast extravasation
- Duodenal hematoma (no perforation): Conservative - NGT decompression, TPN, repeat imaging at 5-7 days. 14 days persist ayite - operate
- Perforation confirmed: Emergency surgery - Kocher maneuver, wide mobilization, primary repair (single/double layer)
- Severe damage: Billroth II or Roux-en-Y reconstruction
- Pyloric exclusion - select cases lo (controversial - individualize cheyyi)
📋 CASE 4: Pancreatic Injury Case
"Pancreas kuda retroperitoneal - peritoneal signs kuddavu. CT sensitivity for ductal injury only 52-54%! Serum amylase useful only if taken >3 hours after injury. So high index of suspicion maintain cheyyali"
| Grade | Duct | Management |
|---|---|---|
| I-II | No duct injury | Conservative - drain, observe |
| III | Duct involved, distal | Distal pancreatectomy ± splenectomy |
| IV | Duct involved, proximal (head) | Drainage + damage control, Whipple select cases |
| V | Massive head disruption | Damage control, complex reconstruction |
"Pancreatic enzymes caustic ga untayi - leak ayite peripancreatic digestion, abscess, fistula, pseudocyst. Grade III+ = duct disruption = operative management mandatory"
📋 CASE 5: Kidney (Renal) Trauma Case
- Grade 1-2: Contusion/minor lac - Conservative
- Grade 3: Major lac without collecting system - Conservative (mostly)
- Grade 4: Lac + collecting system OR renal artery/vein segmental injury - Observe but careful
- Grade 5: Shattered kidney / vascular pedicle avulsion - Operate
- Life-threatening hemorrhage
- Renal pedicle avulsion
- Pulsatile/expanding retroperitoneal hematoma
- Penetrating injury + hemodynamic instability
"Stable - admit, bed rest, hemodynamic monitoring. Repeat CT cheyyi to confirm extravasation resolved. Persist ayite ureteral stent or nephrostomy. Uncontrolled = operate"
"Ikkad hematoma tamponade provide chestundi. Medially - renal vessels isolate chesaka hematoma open cheyyi. Otherwise uncontrolled bleeding - nephrectomy rate increases. Early control = chance to save the kidney"
⚡ DAMAGE CONTROL SURGERY - Doctor definitely adugutadu!
- Temperature < 32-34°C (hypothermia)
- pH < 7.2 (acidosis)
- Coagulopathy (INR elevated, ongoing bleeding)
- "Lethal Triad" - Hypothermia + Acidosis + Coagulopathy
- Stage 1: OR lo - control hemorrhage + contamination only (60-90 min max!)
- Stage 2: ICU - resuscitation, warm, correct coags
- Stage 3: Planned reoperation - definitive repair 24-48 hrs later
"Lethal triad present aite - long surgery = more hypothermia, more acidosis, more coagulopathy - patient chastadu. Abbreviated surgery = stop bleeding + contamination only, ICU lo stabilize, then fix properly. Survival improves!"
🎯 MASTER ANSWER FORMAT for 2-MIN ORAL
"Sir, first I would assess this patient with ATLS primary survey. Based on hemodynamic status - [stable/unstable] - I would [CT/direct OR]. At laparotomy, the retroperitoneal hematoma is in Zone [X], which contains [structures]. For [blunt/penetrating] mechanism, I would [explore/observe] because [WHY]. The exposure would be done using [Mattox/Cattell-Braasch] maneuver after achieving proximal and distal vascular control. If the patient shows signs of lethal triad, damage control approach would be taken."
📌 QUICK FIRE - All "WHY" Questions
| WHY Question | Answer (1 liner) |
|---|---|
| WHY FAST miss retroperitoneal blood? | FAST only intraperitoneal - retro space separate |
| WHY Zone 1 ALWAYS explore blunt? | Aorta/IVC - life threatening vascular injury |
| WHY Zone 3 blunt NEVER explore? | Venous bleeding - tamponade effect - opening worsens it |
| WHY duodenal injury diagnosis delayed? | Retroperitoneal location - peritoneal signs absent/late |
| WHY proximal control before hematoma? | Tamponade release = massive bleed without control |
| WHY damage control? | Lethal triad - prolonged surgery kills |
| WHY amylase >3hrs for pancreas? | Early amylase may be normal before inflammation peaks |
| WHY Mattox = left rotation? | Aorta and supramesocolic vessels are left-sided |
| WHY not explore Zone 2 blunt? | Perinephric tamponade - exploration increases nephrectomy rate |
| WHY Kocher for duodenum? | D2/D3 mobilize cheyyadaniki - retroperitoneal fixation release |
- Case vinagane Mechanism + Hemodynamics note cheskoni
- 2 min lo Zone identify cheyyi
- Structured ga answer cheyyi
- "WHY" adgithe - tamponade / vascular control / anatomical location - oka 3 words explain cheyyachu
goodpm students. you wait for me at the library. pls use the time to study and talk with your partner. we will start immediately as soon as i arrive. each pair will have a total of 7 minutes. 2 cases, 4 questions each case. 2.5pts/question, total of 20 points. passing score is 12. during the exam, you can talk to your partner frst before answering. i will accept one answer only and it will be final. so you have to talk and think before giving me the answer. if the time is up and you did not finish the case, grade is automatically zero for the unanswered question. Ila cheppdu doc
📋 Exam Format - Quick Summary
⚠️ Key Rules - Gurtupettukko!
- Partner tho talk chesukోవచ్చు before answering - use this time wisely!
- One answer only - FINAL - once cheppite change cheyyaradhu
- Time up = zero for remaining questions - speed important!
- 7 min / 8 questions = roughly ~50 seconds per question - fast ga think cheyyali
⚡ Strategy for You
- Case 1: ~3 min (4 questions × ~45 sec)
- Case 2: ~3 min (4 questions × ~45 sec)
- Buffer: ~1 min for tough ones
- Adigi cheppataniki 10-15 sec - quick whisper, confirm answer, THEN speak
- Wrong antē partner correct chesukuntadu before final answer
- Oka person anatomy/zones cheppali, inkokaru management/WHY cheppali - divide responsibility!
Create a 1-page quick reference cheat sheet for exam (anatomy + zones + WHY answers)
mkdir -p /home/daytona/workspace/retroperitoneal-cheatsheet
~/retroperitoneal-cheatsheet/generate_cheatsheet.py
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.units import mm
from reportlab.platypus import (
SimpleDocTemplate, Table, TableStyle, Paragraph, Spacer, HRFlowable
)
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.enums import TA_CENTER, TA_LEFT
from reportlab.platypus import KeepTogether
OUTPUT = "/home/daytona/workspace/retroperitoneal-cheatsheet/Retroperitoneal_Trauma_CheatSheet.pdf"
doc = SimpleDocTemplate(
OUTPUT,
pagesize=A4,
leftMargin=10*mm, rightMargin=10*mm,
topMargin=8*mm, bottomMargin=8*mm
)
W, H = A4
# ── colour palette ──────────────────────────────────────────────────────────
RED = colors.HexColor("#C0392B")
ORANGE = colors.HexColor("#E67E22")
BLUE = colors.HexColor("#1A5276")
GREEN = colors.HexColor("#1E8449")
LTBLUE = colors.HexColor("#D6EAF8")
LTORANGE = colors.HexColor("#FDEBD0")
LTGREEN = colors.HexColor("#D5F5E3")
LTRED = colors.HexColor("#FADBD8")
LTYELLOW = colors.HexColor("#FEF9E7")
WHITE = colors.white
DARK = colors.HexColor("#1C2833")
GRAY = colors.HexColor("#F2F3F4")
MIDGRAY = colors.HexColor("#BDC3C7")
# ── styles ───────────────────────────────────────────────────────────────────
base = getSampleStyleSheet()
def S(name, parent="Normal", **kw):
return ParagraphStyle(name, parent=base[parent], **kw)
title_s = S("title_s", fontSize=13, textColor=WHITE, alignment=TA_CENTER,
fontName="Helvetica-Bold", spaceAfter=0, leading=16)
hdr_s = S("hdr_s", fontSize=7.5, textColor=WHITE, alignment=TA_CENTER,
fontName="Helvetica-Bold", leading=10)
subhdr_s = S("subhdr_s", fontSize=7, textColor=DARK, alignment=TA_CENTER,
fontName="Helvetica-Bold", leading=9)
body_s = S("body_s", fontSize=6.4, textColor=DARK, alignment=TA_LEFT,
fontName="Helvetica", leading=8.5)
bold_s = S("bold_s", fontSize=6.4, textColor=DARK, alignment=TA_LEFT,
fontName="Helvetica-Bold", leading=8.5)
red_s = S("red_s", fontSize=6.4, textColor=RED, alignment=TA_LEFT,
fontName="Helvetica-Bold", leading=8.5)
green_s = S("green_s", fontSize=6.4, textColor=GREEN, alignment=TA_LEFT,
fontName="Helvetica-Bold", leading=8.5)
center_s = S("center_s", fontSize=6.4, textColor=DARK, alignment=TA_CENTER,
fontName="Helvetica", leading=8.5)
cbold_s = S("cbold_s", fontSize=6.4, textColor=DARK, alignment=TA_CENTER,
fontName="Helvetica-Bold", leading=8.5)
cred_s = S("cred_s", fontSize=6.6, textColor=RED, alignment=TA_CENTER,
fontName="Helvetica-Bold", leading=9)
cgreen_s = S("cgreen_s", fontSize=6.6, textColor=GREEN, alignment=TA_CENTER,
fontName="Helvetica-Bold", leading=9)
corange_s = S("corange_s", fontSize=6.6, textColor=ORANGE, alignment=TA_CENTER,
fontName="Helvetica-Bold", leading=9)
tiny_s = S("tiny_s", fontSize=5.8, textColor=DARK, alignment=TA_LEFT,
fontName="Helvetica", leading=7.5)
tinybold_s= S("tinybold_s",fontSize=5.8, textColor=DARK, alignment=TA_LEFT,
fontName="Helvetica-Bold", leading=7.5)
def P(txt, style=body_s): return Paragraph(txt, style)
# ── helper: section header row ───────────────────────────────────────────────
def sec_hdr(text, bg=BLUE, cols=1, col_widths=None):
t = Table([[P(text, hdr_s)]], colWidths=col_widths or [175*mm])
t.setStyle(TableStyle([
("BACKGROUND", (0,0),(-1,-1), bg),
("TOPPADDING", (0,0),(-1,-1), 3),
("BOTTOMPADDING",(0,0),(-1,-1), 3),
("LEFTPADDING", (0,0),(-1,-1), 4),
("RIGHTPADDING", (0,0),(-1,-1), 4),
]))
return t
# ════════════════════════════════════════════════════════════════════════════
# BUILD CONTENT
# ════════════════════════════════════════════════════════════════════════════
story = []
# ── TITLE BAR ────────────────────────────────────────────────────────────────
title_tbl = Table(
[[P("🔴 RETROPERITONEAL TRAUMA — Oral Exam Quick Reference 🔴", title_s)]],
colWidths=[175*mm]
)
title_tbl.setStyle(TableStyle([
("BACKGROUND", (0,0),(-1,-1), RED),
("TOPPADDING", (0,0),(-1,-1), 5),
("BOTTOMPADDING",(0,0),(-1,-1), 5),
("ROUNDEDCORNERS", [3]),
]))
story.append(title_tbl)
story.append(Spacer(1, 2*mm))
# ════════════════════════════════════════════════════════════════════════════
# ROW 1: Anatomy mnemonic + 2-min Framework (side by side)
# ════════════════════════════════════════════════════════════════════════════
cw_left = 85*mm
cw_right = 87*mm
# LEFT: Retroperitoneal structures
anat_rows = [
[P("RETROPERITONEAL STRUCTURES — SAD PUCKER", hdr_s)],
[P("<b>S</b>uprarenal glands (Adrenals)", body_s)],
[P("<b>A</b>orta & IVC", body_s)],
[P("<b>D</b>uodenum (D2, D3, D4 only)", body_s)],
[P("<b>P</b>ancreas (except tail tip)", body_s)],
[P("<b>U</b>reters", body_s)],
[P("<b>C</b>olon — ascending & descending", body_s)],
[P("<b>K</b>idneys", body_s)],
[P("<b>E</b>sophagus (lower)", body_s)],
[P("<b>R</b>ectum (lower 2/3)", body_s)],
]
anat_t = Table(anat_rows, colWidths=[cw_left])
anat_t.setStyle(TableStyle([
("BACKGROUND", (0,0),(0,0), BLUE),
("BACKGROUND", (0,1),(-1,-1), LTBLUE),
("TOPPADDING", (0,0),(-1,-1), 2),
("BOTTOMPADDING",(0,0),(-1,-1), 2),
("LEFTPADDING", (0,0),(-1,-1), 4),
("RIGHTPADDING", (0,0),(-1,-1), 4),
("BOX", (0,0),(-1,-1), 0.5, BLUE),
("INNERGRID", (0,0),(-1,-1), 0.3, MIDGRAY),
]))
# RIGHT: 2-min Think Framework
fw_rows = [
[P("2-MINUTE ORAL FRAMEWORK ⏱", hdr_s)],
[P("1️⃣ MECHANISM → Blunt or Penetrating?", body_s)],
[P("2️⃣ HEMODYNAMICS → Stable or Unstable?", body_s)],
[P("3️⃣ ZONE → Which zone hematoma?", body_s)],
[P("4️⃣ STRUCTURES AT RISK → What inside that zone?", body_s)],
[P("5️⃣ DIAGNOSIS → CT (stable) / Direct OR (unstable)", body_s)],
[P("6️⃣ EXPLORE? → Zone + Mechanism decide", body_s)],
[P("7️⃣ EXPOSURE → Mattox / Cattell-Braasch / Kocher", body_s)],
[P("8️⃣ DAMAGE CONTROL? → Lethal Triad present?", body_s)],
[P("9️⃣ COMPLICATIONS → Fistula, abscess, ACS, sepsis", body_s)],
]
fw_t = Table(fw_rows, colWidths=[cw_right])
fw_t.setStyle(TableStyle([
("BACKGROUND", (0,0),(0,0), ORANGE),
("BACKGROUND", (0,1),(-1,-1), LTORANGE),
("TOPPADDING", (0,0),(-1,-1), 2),
("BOTTOMPADDING",(0,0),(-1,-1), 2),
("LEFTPADDING", (0,0),(-1,-1), 4),
("RIGHTPADDING", (0,0),(-1,-1), 4),
("BOX", (0,0),(-1,-1), 0.5, ORANGE),
("INNERGRID", (0,0),(-1,-1), 0.3, MIDGRAY),
]))
row1 = Table([[anat_t, fw_t]], colWidths=[cw_left+2*mm, cw_right+2*mm])
row1.setStyle(TableStyle([("VALIGN",(0,0),(-1,-1),"TOP"),
("LEFTPADDING",(0,0),(-1,-1),0),
("RIGHTPADDING",(0,0),(-1,-1),2*mm)]))
story.append(row1)
story.append(Spacer(1, 2*mm))
# ════════════════════════════════════════════════════════════════════════════
# ROW 2: ZONES TABLE (full width)
# ════════════════════════════════════════════════════════════════════════════
story.append(sec_hdr("ZONES OF RETROPERITONEUM + HEMATOMA MANAGEMENT", BLUE, col_widths=[175*mm]))
zone_data = [
# header
[P("ZONE", hdr_s), P("LOCATION", hdr_s), P("STRUCTURES", hdr_s),
P("BLUNT", hdr_s), P("PENETRATING", hdr_s), P("EXPOSURE", hdr_s)],
# zone 1
[P("ZONE 1\n(Central)", cbold_s),
P("Midline: aortic hiatus → iliac bifurcation", body_s),
P("Aorta, IVC, Celiac, SMA, SMV,\nproximal renal vessels", body_s),
P("✅ ALWAYS\nExplore", cred_s),
P("✅ ALWAYS\nExplore", cred_s),
P("Mattox (L)\nor Cattell-\nBraasch (R)", center_s)],
# zone 2
[P("ZONE 2\n(Lateral)", cbold_s),
P("Bilateral lateral gutters", body_s),
P("Kidneys, adrenals, renal A&V,\nproximal ureters", body_s),
P("Only if expanding /\npulsatile / urine leak", corange_s),
P("✅ ALWAYS\nExplore", cred_s),
P("Medial renal\nvascular\ncontrol first", center_s)],
# zone 3
[P("ZONE 3\n(Pelvic)", cbold_s),
P("Below iliac bifurcation → pelvis", body_s),
P("Iliac arteries & veins,\npelvic venous plexus", body_s),
P("❌ Do NOT\nOpen!", cgreen_s),
P("✅ ALWAYS\nExplore", cred_s),
P("Packing +\next. fixator;\nAngioembo.", center_s)],
]
cws = [18*mm, 32*mm, 42*mm, 26*mm, 26*mm, 28*mm]
zone_t = Table(zone_data, colWidths=cws, repeatRows=1)
zone_t.setStyle(TableStyle([
("BACKGROUND", (0,0),(-1,0), BLUE),
("BACKGROUND", (0,1),(-1,1), LTBLUE),
("BACKGROUND", (0,2),(-1,2), LTORANGE),
("BACKGROUND", (0,3),(-1,3), LTGREEN),
("BOX", (0,0),(-1,-1), 0.8, BLUE),
("INNERGRID", (0,0),(-1,-1), 0.3, MIDGRAY),
("VALIGN", (0,0),(-1,-1), "MIDDLE"),
("ALIGN", (0,0),(-1,0), "CENTER"),
("TOPPADDING", (0,0),(-1,-1), 2),
("BOTTOMPADDING",(0,0),(-1,-1), 2),
("LEFTPADDING", (0,0),(-1,-1), 3),
("RIGHTPADDING", (0,0),(-1,-1), 3),
]))
story.append(zone_t)
story.append(Spacer(1, 2*mm))
# ════════════════════════════════════════════════════════════════════════════
# ROW 3: Surgical Maneuvers + Damage Control (side by side)
# ════════════════════════════════════════════════════════════════════════════
cw3a = 88*mm
cw3b = 84*mm
# LEFT: Maneuvers
man_rows = [
[P("SURGICAL EXPOSURE MANEUVERS", hdr_s)],
[P("<b>MATTOX (Left medial rotation)</b>", body_s)],
[P("Mobilize: L colon + spleen + pancreas tail + stomach + L kidney → medially\n→ Exposes: Supramesocolic aorta, celiac, SMA, L renal hilum", tiny_s)],
[P("<b>CATTELL-BRAASCH (Right medial rotation)</b>", body_s)],
[P("Mobilize: R colon + cecum → superiorly & to LEFT\n→ Exposes: Infrarenal IVC, R renal hilum, iliac vessels", tiny_s)],
[P("<b>KOCHER Maneuver</b>", body_s)],
[P("Duodenum D2 mobilized medially\n→ Exposes: Pancreatic head, IVC, right renal structures", tiny_s)],
[P("⚠️ GOLDEN RULE: Proximal + Distal control FIRST, then explore!", red_s)],
]
man_t = Table(man_rows, colWidths=[cw3a])
man_t.setStyle(TableStyle([
("BACKGROUND", (0,0),(0,0), GREEN),
("BACKGROUND", (0,1),(-1,-1), LTGREEN),
("TOPPADDING", (0,0),(-1,-1), 2),
("BOTTOMPADDING",(0,0),(-1,-1), 2),
("LEFTPADDING", (0,0),(-1,-1), 4),
("RIGHTPADDING", (0,0),(-1,-1), 4),
("BOX", (0,0),(-1,-1), 0.5, GREEN),
("INNERGRID", (0,0),(-1,-1), 0.3, MIDGRAY),
]))
# RIGHT: Damage Control
dc_rows = [
[P("DAMAGE CONTROL SURGERY 💉", hdr_s)],
[P("<b>Indications (Lethal Triad):</b>", bold_s)],
[P("🌡️ Hypothermia < 32-34°C", body_s)],
[P("🧪 Acidosis pH < 7.2", body_s)],
[P("🩸 Coagulopathy (INR elevated, ongoing bleed)", body_s)],
[P("<b>3 Stages:</b>", bold_s)],
[P("Stage 1: OR — control bleed + contamination (60-90 min max)", body_s)],
[P("Stage 2: ICU — warm, correct coags, resuscitate", body_s)],
[P("Stage 3: Planned reoperation at 24-48 hrs", body_s)],
]
dc_t = Table(dc_rows, colWidths=[cw3b])
dc_t.setStyle(TableStyle([
("BACKGROUND", (0,0),(0,0), RED),
("BACKGROUND", (0,1),(-1,-1), LTRED),
("TOPPADDING", (0,0),(-1,-1), 2),
("BOTTOMPADDING",(0,0),(-1,-1), 2),
("LEFTPADDING", (0,0),(-1,-1), 4),
("RIGHTPADDING", (0,0),(-1,-1), 4),
("BOX", (0,0),(-1,-1), 0.5, RED),
("INNERGRID", (0,0),(-1,-1), 0.3, MIDGRAY),
]))
row3 = Table([[man_t, dc_t]], colWidths=[cw3a+2*mm, cw3b+2*mm])
row3.setStyle(TableStyle([("VALIGN",(0,0),(-1,-1),"TOP"),
("LEFTPADDING",(0,0),(-1,-1),0),
("RIGHTPADDING",(0,0),(-1,-1),2*mm)]))
story.append(row3)
story.append(Spacer(1, 2*mm))
# ════════════════════════════════════════════════════════════════════════════
# ROW 4: WHY Questions Table (full width)
# ════════════════════════════════════════════════════════════════════════════
story.append(sec_hdr('⚡ "WHY" QUICK ANSWERS — Most Likely Oral Questions', ORANGE, col_widths=[175*mm]))
why_data = [
[P("WHY Question", hdr_s), P("Answer", hdr_s)],
[P("WHY Zone 1 blunt — ALWAYS explore?", bold_s),
P("Aorta/IVC/SMA present — life-threatening vascular injury risk — tamponade rupture = death", body_s)],
[P("WHY Zone 2 blunt — observe?", bold_s),
P("Perinephric hematoma = natural tamponade — opening loses it → massive bleed, high nephrectomy rate", body_s)],
[P("WHY Zone 3 blunt — NEVER open?", bold_s),
P("Pelvic fracture venous bleeding — natural tamponade critical — opening → uncontrolled exsanguination", body_s)],
[P("WHY FAST misses retroperitoneal blood?", bold_s),
P("FAST detects only INTRAPERITONEAL free fluid — retroperitoneum is a separate space entirely", body_s)],
[P("WHY duodenal injury diagnosis is delayed?", bold_s),
P("D2/D3/D4 are retroperitoneal — perforation leaks retro, NOT into peritoneum → peritoneal signs absent/late", body_s)],
[P("WHY proximal control BEFORE exploring hematoma?", bold_s),
P("Hematoma provides tamponade on injured vessel — opening without control → massive uncontrolled hemorrhage", body_s)],
[P("WHY damage control instead of full repair?", bold_s),
P("Lethal triad (hypothermia + acidosis + coagulopathy) — prolonged surgery worsens all three → death", body_s)],
[P("WHY pancreas ductal injury (≥Grade III) needs surgery?", bold_s),
P("Pancreatic enzymes are caustic — duct leak → peripancreatic digestion, fistula, abscess, pseudocyst", body_s)],
[P("WHY Mattox = LEFT rotation?", bold_s),
P("Supramesocolic aorta + celiac + SMA are left-sided — left rotation gives optimal exposure", body_s)],
[P("WHY not repair renal artery if ischemia > 1 hour?", bold_s),
P("Warm ischemia >1 hr → irreversible renal damage — repair futile, nephrectomy is better option", body_s)],
]
why_t = Table(why_data, colWidths=[68*mm, 105*mm])
why_style = [
("BACKGROUND", (0,0),(-1,0), ORANGE),
("BOX", (0,0),(-1,-1), 0.8, ORANGE),
("INNERGRID", (0,0),(-1,-1), 0.3, MIDGRAY),
("VALIGN", (0,0),(-1,-1), "MIDDLE"),
("TOPPADDING", (0,0),(-1,-1), 2),
("BOTTOMPADDING",(0,0),(-1,-1), 2),
("LEFTPADDING", (0,0),(-1,-1), 4),
("RIGHTPADDING", (0,0),(-1,-1), 4),
]
# Alternate row colors
for i in range(1, len(why_data)):
bg = LTYELLOW if i % 2 == 1 else WHITE
why_style.append(("BACKGROUND", (0,i),(-1,i), bg))
why_t.setStyle(TableStyle(why_style))
story.append(why_t)
story.append(Spacer(1, 2*mm))
# ════════════════════════════════════════════════════════════════════════════
# ROW 5: Organ-specific mini tables (Kidney + Duodenum + Pancreas)
# ════════════════════════════════════════════════════════════════════════════
cw5 = 57*mm
# KIDNEY
kidney_rows = [
[P("KIDNEY TRAUMA (AAST Grade)", hdr_s)],
[P("Gr 1-2: Contusion/minor lac → Conservative", body_s)],
[P("Gr 3: Major lac, no collecting sys → Conservative", body_s)],
[P("Gr 4: Lac + collecting sys / segmental vessel → Observe; stent if urine leak persists", body_s)],
[P("Gr 5: Shattered / pedicle avulsion → Surgery + nephrectomy", red_s)],
[P("Operate if: hemorrhage / pedicle avulsion / pulsatile hematoma / penetrating + unstable", tiny_s)],
]
kid_t = Table(kidney_rows, colWidths=[cw5])
kid_t.setStyle(TableStyle([
("BACKGROUND", (0,0),(0,0), BLUE),
("BACKGROUND", (0,1),(-1,-1), LTBLUE),
("TOPPADDING", (0,0),(-1,-1), 2),
("BOTTOMPADDING",(0,0),(-1,-1), 2),
("LEFTPADDING", (0,0),(-1,-1), 3),
("RIGHTPADDING", (0,0),(-1,-1), 3),
("BOX", (0,0),(-1,-1), 0.5, BLUE),
("INNERGRID", (0,0),(-1,-1), 0.3, MIDGRAY),
]))
# DUODENUM
duod_rows = [
[P("DUODENUM TRAUMA", hdr_s)],
[P("Hematoma (no perf): NGT + TPN, re-image at 5-7 days\nIf persist >14 days → operate to evacuate", body_s)],
[P("Perforation: Emergency surgery\n→ Wide Kocher + primary repair (1 or 2 layer)", body_s)],
[P("Large loss / near ampulla: Billroth II or Roux-en-Y", body_s)],
[P("CT signs: Retroperitoneal FREE AIR (pathognomonic!)\n+ wall thickening + periduodenal fluid", red_s)],
[P("Key: Peritoneal signs ABSENT (retro location) → always suspect!", tinybold_s)],
]
duo_t = Table(duod_rows, colWidths=[cw5])
duo_t.setStyle(TableStyle([
("BACKGROUND", (0,0),(0,0), ORANGE),
("BACKGROUND", (0,1),(-1,-1), LTORANGE),
("TOPPADDING", (0,0),(-1,-1), 2),
("BOTTOMPADDING",(0,0),(-1,-1), 2),
("LEFTPADDING", (0,0),(-1,-1), 3),
("RIGHTPADDING", (0,0),(-1,-1), 3),
("BOX", (0,0),(-1,-1), 0.5, ORANGE),
("INNERGRID", (0,0),(-1,-1), 0.3, MIDGRAY),
]))
# PANCREAS
panc_rows = [
[P("PANCREAS TRAUMA (AAST Grade)", hdr_s)],
[P("Gr I-II: No duct injury → Conservative + drain", body_s)],
[P("Gr III: Duct injury, DISTAL → Distal pancreatectomy ± splenectomy", body_s)],
[P("Gr IV: Duct injury, PROXIMAL (head) → Drainage; Whipple select cases", body_s)],
[P("Gr V: Massive head disruption → Damage control + complex recon", red_s)],
[P("Key: Serum amylase useful only if >3 hrs post-injury; CT sensitivity only 52-54%!", tinybold_s)],
]
pan_t = Table(panc_rows, colWidths=[cw5])
pan_t.setStyle(TableStyle([
("BACKGROUND", (0,0),(0,0), GREEN),
("BACKGROUND", (0,1),(-1,-1), LTGREEN),
("TOPPADDING", (0,0),(-1,-1), 2),
("BOTTOMPADDING",(0,0),(-1,-1), 2),
("LEFTPADDING", (0,0),(-1,-1), 3),
("RIGHTPADDING", (0,0),(-1,-1), 3),
("BOX", (0,0),(-1,-1), 0.5, GREEN),
("INNERGRID", (0,0),(-1,-1), 0.3, MIDGRAY),
]))
row5 = Table([[kid_t, duo_t, pan_t]], colWidths=[cw5+2*mm, cw5+2*mm, cw5+2*mm])
row5.setStyle(TableStyle([("VALIGN",(0,0),(-1,-1),"TOP"),
("LEFTPADDING",(0,0),(-1,-1),0),
("RIGHTPADDING",(0,0),(-1,-1),2*mm)]))
story.append(row5)
story.append(Spacer(1, 2*mm))
# ════════════════════════════════════════════════════════════════════════════
# FOOTER
# ════════════════════════════════════════════════════════════════════════════
footer_data = [[
P("Hemodynamically <b>UNSTABLE</b> → Emergency Laparotomy | "
"Hemodynamically <b>STABLE</b> → CT Abdomen (IV contrast) | "
"FAST = Intraperitoneal only (misses retro!) | "
"All Penetrating → Explore all zones | "
"Blunt Zone 3 → NEVER open", center_s)
]]
footer_t = Table(footer_data, colWidths=[175*mm])
footer_t.setStyle(TableStyle([
("BACKGROUND", (0,0),(-1,-1), DARK),
("TOPPADDING", (0,0),(-1,-1), 3),
("BOTTOMPADDING",(0,0),(-1,-1), 3),
("LEFTPADDING", (0,0),(-1,-1), 5),
("RIGHTPADDING", (0,0),(-1,-1), 5),
]))
# override text color white for footer
footer_t2 = Table([[P(
"<font color='white'>Hemodynamically <b>UNSTABLE</b> → Emergency Laparotomy | "
"Hemodynamically <b>STABLE</b> → CT Abdomen (IV contrast) | "
"FAST = Intraperitoneal only (misses retro!) | "
"All Penetrating → Explore all zones | "
"Blunt Zone 3 → NEVER open</font>", center_s)]], colWidths=[175*mm])
footer_t2.setStyle(TableStyle([
("BACKGROUND", (0,0),(-1,-1), DARK),
("TOPPADDING", (0,0),(-1,-1), 3),
("BOTTOMPADDING",(0,0),(-1,-1), 3),
]))
story.append(footer_t2)
# ── BUILD ────────────────────────────────────────────────────────────────────
doc.build(story)
print(f"PDF created: {OUTPUT}")
cd /home/daytona/workspace/retroperitoneal-cheatsheet && python generate_cheatsheet.py 2>&1
ls -lh /home/daytona/workspace/retroperitoneal-cheatsheet/
Retroperitoneal Trauma CheatSheet
PDF Document · PDF
Cheat sheet lo emi undi:
| Section | Content |
|---|---|
| 🔵 SAD PUCKER mnemonic | All retroperitoneal structures |
| 🟠 2-Minute Framework | 9-step oral answer template |
| 🔵 Zones Table | Zone 1/2/3 - structures + Blunt/Penetrating management |
| 🟢 Surgical Maneuvers | Mattox, Cattell-Braasch, Kocher - when + why |
| 🔴 Damage Control | Lethal triad + 3 stages |
| 🟡 WHY Answers | 10 most likely "why" questions + answers |
| 🔵🟠🟢 Organ mini-tables | Kidney / Duodenum / Pancreas grades + management |
| ⚫ Footer | Key decision rules in one line |
Generate practice Q&A scenarios with time limits (mock exam)
~/retroperitoneal-cheatsheet/generate_mockexam.py
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.units import mm
from reportlab.platypus import (
SimpleDocTemplate, Table, TableStyle, Paragraph, Spacer, PageBreak, HRFlowable
)
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_JUSTIFY
OUTPUT = "/home/daytona/workspace/retroperitoneal-cheatsheet/Retroperitoneal_Mock_Exam.pdf"
# ── colours ──────────────────────────────────────────────────────────────────
RED = colors.HexColor("#C0392B")
ORANGE = colors.HexColor("#E67E22")
BLUE = colors.HexColor("#1A5276")
GREEN = colors.HexColor("#1E8449")
PURPLE = colors.HexColor("#6C3483")
TEAL = colors.HexColor("#117A65")
LTBLUE = colors.HexColor("#D6EAF8")
LTORANGE = colors.HexColor("#FDEBD0")
LTGREEN = colors.HexColor("#D5F5E3")
LTRED = colors.HexColor("#FADBD8")
LTPURPLE = colors.HexColor("#E8DAEF")
LTYELLOW = colors.HexColor("#FEF9E7")
LTTEAL = colors.HexColor("#D1F2EB")
WHITE = colors.white
DARK = colors.HexColor("#1C2833")
MIDGRAY = colors.HexColor("#BDC3C7")
LIGHTGRAY= colors.HexColor("#F2F3F4")
# ── styles ───────────────────────────────────────────────────────────────────
base = getSampleStyleSheet()
def S(name, **kw):
return ParagraphStyle(name, parent=base["Normal"], **kw)
title_s = S("ts", fontSize=15, textColor=WHITE, alignment=TA_CENTER,
fontName="Helvetica-Bold", leading=18)
sub_s = S("ss", fontSize=9, textColor=WHITE, alignment=TA_CENTER,
fontName="Helvetica", leading=12)
hdr_s = S("hs", fontSize=8, textColor=WHITE, alignment=TA_CENTER,
fontName="Helvetica-Bold", leading=10)
case_s = S("cs", fontSize=11, textColor=WHITE, alignment=TA_LEFT,
fontName="Helvetica-Bold", leading=14)
scenario_s= S("sc", fontSize=9.5,textColor=DARK, alignment=TA_JUSTIFY,
fontName="Helvetica", leading=13, spaceAfter=2)
q_s = S("qs", fontSize=10, textColor=BLUE, alignment=TA_LEFT,
fontName="Helvetica-Bold", leading=13)
qnum_s = S("qn", fontSize=11, textColor=WHITE, alignment=TA_CENTER,
fontName="Helvetica-Bold", leading=14)
timer_s = S("tm", fontSize=9, textColor=ORANGE, alignment=TA_CENTER,
fontName="Helvetica-Bold", leading=11)
ans_hdr_s = S("ah", fontSize=8.5,textColor=WHITE, alignment=TA_LEFT,
fontName="Helvetica-Bold", leading=11)
ans_s = S("as", fontSize=8.5,textColor=DARK, alignment=TA_LEFT,
fontName="Helvetica", leading=11)
ans_bold_s= S("ab", fontSize=8.5,textColor=DARK, alignment=TA_LEFT,
fontName="Helvetica-Bold", leading=11)
why_s = S("ws", fontSize=8.5,textColor=GREEN, alignment=TA_LEFT,
fontName="Helvetica-Bold", leading=11)
red_s = S("rs", fontSize=8.5,textColor=RED, alignment=TA_LEFT,
fontName="Helvetica-Bold", leading=11)
pts_s = S("ps", fontSize=9, textColor=WHITE, alignment=TA_CENTER,
fontName="Helvetica-Bold", leading=11)
tip_s = S("tip", fontSize=7.5,textColor=TEAL, alignment=TA_LEFT,
fontName="Helvetica-Oblique", leading=10)
instr_s = S("is", fontSize=8.5,textColor=DARK, alignment=TA_LEFT,
fontName="Helvetica", leading=11)
center_s = S("ce", fontSize=8, textColor=DARK, alignment=TA_CENTER,
fontName="Helvetica", leading=10)
bold_center_s = S("bc", fontSize=8, textColor=DARK, alignment=TA_CENTER,
fontName="Helvetica-Bold", leading=10)
def P(txt, st=ans_s): return Paragraph(txt, st)
def HR(): return HRFlowable(width="100%", thickness=0.5, color=MIDGRAY, spaceAfter=3, spaceBefore=3)
# ════════════════════════════════════════════════════════════════════════════
# DATA: 3 EXAM SETS
# ════════════════════════════════════════════════════════════════════════════
# Each set: 2 cases × 4 questions
# Format: {set_title, set_color, cases: [{case_title, scenario, bg, questions: [{q, marks, time_s, answer, why_key}]}]}
EXAMS = [
# ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
# SET A
# ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
{
"title": "MOCK EXAM — SET A",
"color": BLUE,
"cases": [
{
"title": "CASE A-1 | Blunt Abdominal Trauma",
"bg": BLUE,
"scenario": (
"A 32-year-old male is brought to the ER after a high-speed motor vehicle collision. "
"He was the unrestrained driver. On arrival: BP 70/40 mmHg, HR 148 bpm, RR 24/min, GCS 14. "
"Abdomen is distended and tender diffusely. FAST exam shows free fluid in Morrison's pouch. "
"Chest X-ray is clear. Pelvis X-ray shows no fracture."
),
"questions": [
{
"q": "Q1. What is your immediate management priority for this patient?",
"marks": 2.5,
"time_s": 50,
"answer": (
"Immediate priority: ATLS primary survey — secure airway (intubate if needed), "
"ensure adequate breathing, establish 2 large-bore IV access, aggressive fluid "
"resuscitation with type-specific blood + crystalloids (1:1:1 — pRBC:FFP:platelets). "
"Patient is hemodynamically UNSTABLE (BP 70/40, HR 148) with FAST-positive free fluid "
"→ activate massive transfusion protocol → proceed to EMERGENCY LAPAROTOMY immediately. "
"No time for CT scan in unstable patient."
),
"why_key": "Unstable + FAST positive = straight to OR. CT wastes time → patient can die on table."
},
{
"q": "Q2. At laparotomy, you find a large central (Zone 1) retroperitoneal hematoma that is not pulsatile but is expanding. What do you do and WHY?",
"marks": 2.5,
"time_s": 55,
"answer": (
"Zone 1 hematoma — ALWAYS explore, regardless of blunt or penetrating mechanism, "
"regardless of whether it is pulsatile or not. "
"Step 1: Achieve PROXIMAL control first — clamp the aorta at the diaphragmatic hiatus if needed. "
"Step 2: Use LEFT MEDIAL VISCERAL ROTATION (Mattox maneuver) — mobilize left colon, spleen, "
"stomach, pancreatic tail, left kidney medially → expose supramesocolic aorta, celiac, SMA. "
"Step 3: Explore hematoma, identify bleeding vessel, repair or ligate."
),
"why_key": "Zone 1 = Aorta/IVC/major vessels. Even non-pulsatile hematoma hides lethal vascular injury. Tamponade can rupture any moment → MUST explore."
},
{
"q": "Q3. During exploration, the patient develops temperature 31°C, pH 7.15, and coagulopathy (INR 2.1). What strategy do you adopt?",
"marks": 2.5,
"time_s": 50,
"answer": (
"This is the LETHAL TRIAD — hypothermia (31°C) + acidosis (pH 7.15) + coagulopathy (INR 2.1). "
"Switch to DAMAGE CONTROL SURGERY:\n"
"Stage 1 (OR, 60-90 min MAX): Control hemorrhage with packing/clamps, control "
"GI contamination with stapling — NO definitive repair.\n"
"Stage 2 (ICU): Rewarm patient, correct coagulopathy (FFP/platelets/cryo), "
"correct acidosis, resuscitate.\n"
"Stage 3 (Planned reoperation 24-48 hrs): Definitive repair once physiologically stable."
),
"why_key": "Continuing surgery in lethal triad worsens all 3 parameters → irreversible coagulopathy → death. Abbreviate to save life first."
},
{
"q": "Q4. Post-op Day 3, patient develops abdominal distension, rising bladder pressure (28 mmHg), oliguria, and worsening oxygenation. What is the diagnosis and management?",
"marks": 2.5,
"time_s": 50,
"answer": (
"Diagnosis: ABDOMINAL COMPARTMENT SYNDROME (ACS) — defined as intra-abdominal "
"pressure >20 mmHg with new organ dysfunction.\n"
"Features here: Bladder pressure 28 mmHg + oliguria (renal) + poor oxygenation (pulmonary) "
"+ distension (bowel).\n"
"Management: EMERGENCY DECOMPRESSIVE LAPAROTOMY — open abdomen, do NOT close.\n"
"Leave open with temporary abdominal closure (vacuum-assisted closure / Bogota bag).\n"
"Definitive fascial closure after organ function normalizes (usually 3-5 days)."
),
"why_key": "Raised intra-abdominal pressure compresses IVC (reduced preload), diaphragm (ventilation failure), renal vessels (oliguria). Decompression is the only treatment."
},
]
},
{
"title": "CASE A-2 | Penetrating Abdominal Trauma — Stab Wound",
"bg": TEAL,
"scenario": (
"A 22-year-old male presents with a stab wound to the right flank. "
"BP 110/70, HR 104, RR 18. Abdomen mildly tender in right flank. "
"No peritoneal signs. FAST exam shows no free fluid. "
"CT abdomen with IV contrast shows a track entering the retroperitoneum, "
"Grade 3 right renal laceration with a contained retroperitoneal hematoma "
"and no active contrast extravasation. No pneumoperitoneum."
),
"questions": [
{
"q": "Q1. FAST is negative and the patient is stable. Does a negative FAST rule out retroperitoneal injury? Explain.",
"marks": 2.5,
"time_s": 45,
"answer": (
"NO — negative FAST does NOT rule out retroperitoneal injury.\n"
"FAST detects only INTRAPERITONEAL free fluid (Morrison's pouch, splenorenal recess, "
"pelvis, pericardium). The retroperitoneum is a SEPARATE space — blood collecting "
"there does NOT appear on FAST.\n"
"In this case: retroperitoneal hematoma from renal laceration → FAST negative → "
"but significant injury present.\n"
"CT with IV contrast is the gold standard for retroperitoneal injury assessment "
"in hemodynamically stable patients."
),
"why_key": "FAST = intraperitoneal only. Retro is a separate compartment. Never use FAST alone to exclude retroperitoneal trauma."
},
{
"q": "Q2. CT shows a right Zone 2 retroperitoneal hematoma from a Grade 3 renal laceration — no active bleeding. Penetrating mechanism. What is your management?",
"marks": 2.5,
"time_s": 55,
"answer": (
"Penetrating Zone 2 hematoma → ALWAYS explore (unlike blunt Zone 2 which can be observed).\n"
"At laparotomy:\n"
"Step 1: MEDIAL RENAL VASCULAR CONTROL first — isolate renal artery and vein medially "
"BEFORE opening the perinephric hematoma. This prevents uncontrolled hemorrhage.\n"
"Step 2: Open hematoma carefully, assess injury.\n"
"Grade 3: Major laceration, no collecting system → attempt renorrhaphy (repair) to "
"preserve the kidney. Use manual compression + hemostatic agents + suture.\n"
"If expanding/pulsatile or uncontrolled: nephrectomy.\n"
"Confirm contralateral kidney function before nephrectomy (one-shot IVP intraop)."
),
"why_key": "All penetrating Zone 2 hematomas = explore. Medial vascular control first = prevents catastrophic bleed when hematoma is opened."
},
{
"q": "Q3. Why do you achieve medial renal vascular control BEFORE opening the perinephric hematoma?",
"marks": 2.5,
"time_s": 40,
"answer": (
"The perinephric hematoma acts as a natural TAMPONADE on the injured renal parenchyma "
"and vessels. If you open the hematoma without prior vascular control:\n"
"→ Tamponade effect is lost instantly\n"
"→ Massive, uncontrolled hemorrhage from renal hilum/parenchyma\n"
"→ Surgeon forced into emergency nephrectomy\n"
"By isolating the renal artery (and vein) medially FIRST:\n"
"→ Can occlude vessels if uncontrolled bleeding occurs\n"
"→ Allows safe renorrhaphy\n"
"→ Significantly reduces nephrectomy rate"
),
"why_key": "Control before opening = save the kidney. No control before opening = lose the kidney."
},
{
"q": "Q4. Post-op Day 2: patient develops flank pain, fever 38.8°C, and urine output drops. CT shows urinoma (urine collection). What is the next step?",
"marks": 2.5,
"time_s": 45,
"answer": (
"Urinoma = urine extravasation from collecting system injury not recognized/repaired.\n"
"Management — stepwise:\n"
"1. Percutaneous drainage of urinoma (IR-guided) to decompress collection.\n"
"2. Retrograde ureteral stenting (cystoscopy) to divert urine and allow collecting "
"system to heal — PREFERRED first-line.\n"
"3. If stenting fails or injury is large: nephrostomy tube placement (percutaneous).\n"
"4. Operative repair only if above measures fail or injury is major.\n"
"Monitor with follow-up CT urogram at 48-72 hrs."
),
"why_key": "Urinoma = missed collecting system injury. Minimally invasive first — drain + stent. Avoid reoperation if possible."
},
]
},
]
},
# ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
# SET B
# ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
{
"title": "MOCK EXAM — SET B",
"color": GREEN,
"cases": [
{
"title": "CASE B-1 | Blunt Trauma — Pelvic Fracture",
"bg": GREEN,
"scenario": (
"A 45-year-old female is brought in after being struck by a bus. "
"BP 85/50 mmHg, HR 138 bpm. Pelvis is unstable on compression. "
"Pelvic X-ray: open-book pelvic fracture (symphysis pubis diastasis). "
"FAST exam: no free intraperitoneal fluid. "
"Despite 2L crystalloid resuscitation, BP remains 80/50."
),
"questions": [
{
"q": "Q1. FAST is negative but the patient is hemodynamically unstable. Where is the bleeding coming from and why can FAST not detect it?",
"marks": 2.5,
"time_s": 50,
"answer": (
"Source of bleeding: Zone 3 retroperitoneum — pelvic fracture disrupts the pelvic "
"venous plexus (and sometimes iliac arteries), causing massive RETROPERITONEAL hemorrhage.\n"
"Why FAST is negative:\n"
"Blood is collecting in the RETROPERITONEUM (Zone 3 pelvic space), NOT the peritoneal cavity. "
"FAST only detects intraperitoneal fluid. Retroperitoneum is a separate compartment — blood "
"there is invisible on FAST.\n"
"Key teaching: Pelvic fracture + hemodynamic instability + negative FAST = Zone 3 "
"retroperitoneal hemorrhage until proven otherwise."
),
"why_key": "Open-book fracture tears pelvic venous plexus. Blood stays retroperitoneal. FAST = intraperitoneal only → missed entirely."
},
{
"q": "Q2. How do you manage this Zone 3 retroperitoneal hematoma? Would you open it at laparotomy? WHY or WHY NOT?",
"marks": 2.5,
"time_s": 55,
"answer": (
"Zone 3, BLUNT mechanism → Do NOT open the hematoma at laparotomy.\n"
"WHY NOT:\n"
"• Pelvic fracture bleeding is predominantly VENOUS (pelvic venous plexus).\n"
"• The retroperitoneal space acts as a natural tamponade — holds pressure on venous bleed.\n"
"• Opening it releases the tamponade → uncontrolled exsanguination → death.\n\n"
"Correct management:\n"
"1. Apply pelvic binder / sheet immediately (temporary)\n"
"2. External pelvic fixation (orthopaedics) — reduces pelvic volume, restores tamponade\n"
"3. Preperitoneal pelvic packing (PPP) — pack anterior preperitoneal space\n"
"4. If arterial bleeding suspected (no response to packing): Angiography + selective embolization\n"
"5. REBOA (Resuscitative Endovascular Balloon Occlusion of Aorta) — in extremis"
),
"why_key": "Venous bleeding + retroperitoneal tamponade = do NOT open. Opening = death. Restore tamponade by compressing pelvis mechanically."
},
{
"q": "Q3. After pelvic packing and external fixation, BP stabilizes at 105/70. CT scan now shows no active arterial blush. What is the next step in management?",
"marks": 2.5,
"time_s": 45,
"answer": (
"Patient is now hemodynamically STABLE after packing + external fixation.\n"
"No active arterial blush on CT → angioembolization not immediately needed.\n\n"
"Next steps:\n"
"1. Admit to ICU — continuous hemodynamic monitoring.\n"
"2. Continue massive transfusion protocol (1:1:1 ratio) until coagulopathy corrected.\n"
"3. Serial abdominal exams — watch for signs of re-bleeding.\n"
"4. Packs removed at 24-48 hrs planned reoperation (damage control stage 3).\n"
"5. Orthopaedics: plan definitive pelvic fixation once physiologically stable.\n"
"6. If re-bleeding occurs → angiography + embolization."
),
"why_key": "Stable after packing = ICU management. Remove packs at 24-48 hrs. Angioembo reserved for arterial blush or re-bleeding."
},
{
"q": "Q4. During pelvic packing, you inadvertently enter the peritoneal cavity. What complications must you now watch for and why?",
"marks": 2.5,
"time_s": 45,
"answer": (
"By entering the peritoneum, you have disrupted the retroperitoneal barrier.\n\n"
"Complications to watch for:\n"
"1. LOSS OF TAMPONADE — peritoneum opened = retroperitoneal pressure equalizes "
"with peritoneal cavity → pelvic hematoma decompresses → re-bleeding risk.\n"
"2. FECAL CONTAMINATION — if bowel injury missed, now has free access to peritoneum.\n"
"3. ABDOMINAL COMPARTMENT SYNDROME — blood + packs + bowel edema → raised IAP.\n"
"4. INFECTION/SEPSIS — pelvic hematoma now communicates with peritoneal cavity.\n\n"
"Management: Formal exploration, pack properly, close peritoneum if possible, "
"monitor bladder pressure for ACS."
),
"why_key": "Retroperitoneal tamponade works only if peritoneum is INTACT. Breach it = lose tamponade = re-bleed + contamination risk."
},
]
},
{
"title": "CASE B-2 | Blunt Trauma — Seat Belt Injury",
"bg": ORANGE,
"scenario": (
"A 28-year-old male, restrained driver, presents after head-on collision. "
"Seat-belt sign across upper abdomen. BP 118/76, HR 92, RR 16. "
"Mild epigastric tenderness. FAST negative. "
"Serum amylase at 2 hrs post-injury: 140 U/L (normal). "
"CT abdomen: hypodense line across the neck of pancreas with surrounding edema. No free fluid."
),
"questions": [
{
"q": "Q1. What specific injury are you most concerned about and why is this mechanism (seat belt) classically associated with it?",
"marks": 2.5,
"time_s": 45,
"answer": (
"Most concerned about: PANCREATIC TRANSECTION at the neck — Grade III/IV pancreatic injury "
"with probable main pancreatic duct disruption.\n\n"
"Why seat belt mechanism:\n"
"The pancreatic NECK overlies the vertebral column (L1-L2). In a seat belt injury, "
"the anterior abdominal wall is forcibly compressed against the lap belt → "
"pancreas is crushed between the seat belt/steering wheel AND the rigid vertebral column. "
"The neck is the narrowest, most fixed part → maximum shear force here → transection.\n"
"Classic: 'Handlebar injury' in children, 'Seat belt injury' in adults."
),
"why_key": "Pancreatic neck = directly over vertebral column. Compression = crushing between two hard surfaces = transection. Retroperitoneal location = silent injury."
},
{
"q": "Q2. Serum amylase at 2 hrs is NORMAL. Does this rule out pancreatic injury? What is the most useful investigation now?",
"marks": 2.5,
"time_s": 45,
"answer": (
"NO — normal early amylase does NOT rule out pancreatic injury.\n"
"Amylase rises AFTER inflammation develops — serum amylase is only reliable if "
"measured MORE THAN 3 HOURS after injury. Early levels (within 2-3 hrs) can be "
"completely normal even with significant pancreatic injury.\n\n"
"Sensitivity of amylase for pancreatic trauma: poor specificity.\n\n"
"Best investigations now:\n"
"1. CONTRAST-ENHANCED CT ABDOMEN (already done) — sensitivity 47-79% for parenchymal "
"injury, 52-54% for ductal injury. CT shows pancreatic neck hypodensity here → high suspicion.\n"
"2. MRCP (Magnetic Resonance Cholangiopancreatography) — best non-invasive test for "
"DUCTAL integrity.\n"
"3. ERCP — both diagnostic AND therapeutic (can stent duct)."
),
"why_key": "Amylase < 3 hrs = unreliable. CT = first line but misses duct 50% of time. MRCP/ERCP = gold standard for ductal assessment."
},
{
"q": "Q3. CT confirms Grade III pancreatic injury — transection at neck with likely main duct disruption. What is the operative management?",
"marks": 2.5,
"time_s": 55,
"answer": (
"Grade III = main pancreatic duct disruption, DISTAL to the superior mesenteric vein.\n\n"
"Operative management:\n"
"DISTAL PANCREATECTOMY ± splenectomy.\n\n"
"Steps:\n"
"1. Enter lesser sac via gastrocolic ligament division.\n"
"2. Mobilize hepatic flexure.\n"
"3. Kocher maneuver — mobilize pancreatic head.\n"
"4. Assess injury — confirm duct involvement, location relative to SMV.\n"
"5. Transect pancreas to LEFT of injury, oversew proximal stump.\n"
"6. Distal pancreatectomy (remove body + tail).\n"
"7. Splenectomy if splenic vessels involved (spleen-preserving possible in stable patients).\n"
"8. Place closed-suction drain near pancreatic stump.\n\n"
"WHY resect: Pancreatic enzymes are caustic — duct leak = peripancreatic digestion, "
"fistula, pseudocyst, abscess."
),
"why_key": "Grade III = duct disrupted, distal → distal pancreatectomy. Leaving duct leak = enzyme digestion of surrounding tissue = fistula/sepsis/death."
},
{
"q": "Q4. Post-op Day 5: drain output increases to 200 mL/day, amylase in drain fluid: 3× serum amylase. What is this complication and how do you manage it?",
"marks": 2.5,
"time_s": 45,
"answer": (
"Diagnosis: PANCREATIC FISTULA (Post-operative pancreatic fistula — POPF).\n"
"Defined as: drain amylase > 3× upper limit of normal serum amylase on/after post-op day 3.\n\n"
"Grading (ISGPF):\n"
"• Grade A (biochemical leak): No clinical impact → keep drain, observe\n"
"• Grade B: Clinical impact, drain needed >3 wks or IR drainage → NPO + TPN + octreotide\n"
"• Grade C: Organ failure / reoperation needed → aggressive management\n\n"
"Management:\n"
"1. Keep drain IN — do NOT remove (drain controls the fistula)\n"
"2. NPO + Total Parenteral Nutrition (TPN)\n"
"3. Octreotide (somatostatin analogue) — reduces pancreatic secretion\n"
"4. ERCP + ductal stenting if partial duct disruption\n"
"5. Most Grade A/B fistulas close spontaneously in 4-6 weeks"
),
"why_key": "Drain amylase > 3× serum = POPF. Remove drain = uncontrolled fistula → abscess → sepsis. Keep drain in = controlled fistula → heals."
},
]
},
]
},
# ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
# SET C
# ━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
{
"title": "MOCK EXAM — SET C",
"color": PURPLE,
"cases": [
{
"title": "CASE C-1 | Gunshot Wound — Multiple Zones",
"bg": PURPLE,
"scenario": (
"A 35-year-old male presents with a single gunshot wound to the abdomen (left of umbilicus). "
"BP 90/60, HR 125. Abdomen rigid, peritoneal signs present. "
"He is taken directly to the OR. At laparotomy: small bowel perforations (×2), "
"and a large ZONE 1 pulsatile retroperitoneal hematoma is discovered."
),
"questions": [
{
"q": "Q1. You find a Zone 1 pulsatile retroperitoneal hematoma during laparotomy. What is your approach and why is it ALWAYS mandatory to explore Zone 1?",
"marks": 2.5,
"time_s": 55,
"answer": (
"Zone 1, PENETRATING mechanism → MANDATORY exploration regardless of pulsatile or not.\n\n"
"Approach:\n"
"1. Achieve PROXIMAL AORTIC CONTROL first — compress aorta at diaphragmatic hiatus manually "
"or clamp, before opening hematoma.\n"
"2. LEFT MEDIAL VISCERAL ROTATION (Mattox maneuver) for supramesocolic Zone 1:\n"
" — Mobilize: L colon, spleen, stomach, pancreatic tail, L kidney → retract medially\n"
" — Exposes: entire abdominal aorta, celiac, SMA, L renal hilum.\n"
"3. For infrarenal Zone 1 (right side): Cattell-Braasch maneuver.\n"
"4. Identify injured vessel → repair primarily if possible, or damage control shunt.\n\n"
"WHY always explore Zone 1:\n"
"Zone 1 contains the aorta, IVC, celiac, SMA, SMV, proximal renal vessels — all "
"potentially life-threatening if injured. Tamponade can fail at any moment. "
"Missed vascular injury = death."
),
"why_key": "Zone 1 = major vessels. Pulsatile or not = always explore. Proximal control first = controlled exploration."
},
{
"q": "Q2. The Zone 1 hematoma is from an infrarenal aortic injury. You find a 1.5 cm lateral laceration. How do you repair it and what if primary repair causes >50% narrowing?",
"marks": 2.5,
"time_s": 50,
"answer": (
"Primary repair (lateral arteriorrhaphy):\n"
"• Use 3-0 or 4-0 prolene suture, running or interrupted\n"
"• Lateral repair of aortic laceration — close the hole without narrowing lumen\n\n"
"If primary repair causes >30-50% narrowing of lumen:\n"
"• PATCH ANGIOPLASTY — use a patch of autologous vein (saphenous) or prosthetic "
"(Dacron/PTFE) to widen the repair.\n"
"• In a contaminated field (bowel injury present here): prefer autologous vein patch "
"or bovine pericardium — prosthetic graft has higher infection risk.\n\n"
"If segment is destroyed: interposition graft (Dacron tube graft) — but HIGH infection "
"risk with bowel contamination → damage control, extra-anatomic bypass later.\n\n"
"Damage control option: temporary intraluminal shunt → definitive repair at Stage 3."
),
"why_key": "Simple laceration = primary repair. Narrowing >30-50% = patch. Contaminated field = avoid prosthetic. Shunt = damage control."
},
{
"q": "Q3. After aortic repair, you notice the right iliac artery has a Zone 3 penetrating injury with active bleeding. How does your management differ from a blunt Zone 3 hematoma?",
"marks": 2.5,
"time_s": 50,
"answer": (
"PENETRATING Zone 3 hematoma → ALWAYS explore and repair (unlike blunt Zone 3).\n\n"
"Key difference from blunt Zone 3:\n"
"• Blunt Zone 3 = venous fracture bleeding → do NOT open (loses tamponade)\n"
"• Penetrating Zone 3 = arterial injury (iliac artery here) → MUST repair to prevent "
"limb ischemia and ongoing hemorrhage\n\n"
"Management of iliac artery injury:\n"
"1. Proximal and distal control of iliac artery\n"
"2. Primary repair if simple laceration (lateral arteriorrhaphy)\n"
"3. Interposition graft if segment destroyed\n"
"4. Damage control: temporary intraluminal shunt → definitive repair at Stage 3\n"
" (preferred if patient in lethal triad)\n"
"5. Ligation is possible for external iliac in extremis (with planned bypass)\n"
"NEVER ligate common iliac artery without bypass."
),
"why_key": "Penetrating = arterial injury = must repair. Blunt = venous = do not open. Penetrating always = explore all zones."
},
{
"q": "Q4. Post-op: Right lower limb is cold, pale, pulseless with paresthesia. What is this and what do you do next?",
"marks": 2.5,
"time_s": 45,
"answer": (
"Diagnosis: ACUTE LIMB ISCHEMIA — 6 P's: Pain, Pallor, Pulselessness, Paresthesia, "
"Paralysis, Poikilothermia (cold).\n"
"Here: Cold + pale + pulseless + paresthesia = critical ischemia → surgical emergency.\n\n"
"Likely cause: Iliac artery repair thrombosis / stenosis / missed injury / "
"temporary shunt occlusion.\n\n"
"Immediate management:\n"
"1. Anticoagulate immediately — IV heparin bolus (if no contraindication)\n"
"2. Urgent duplex ultrasound / CT angiography to localize occlusion\n"
"3. Return to OR IMMEDIATELY — explore iliac repair, Fogarty thrombectomy\n"
"4. If repair stenosed: revise repair / patch\n"
"5. Fasciotomy of compartments if ischemia >4-6 hrs (prevent compartment syndrome)\n"
"Time is critical — >6 hours warm ischemia → irreversible muscle necrosis."
),
"why_key": "6 P's = acute ischemia. Heparin + urgent return to OR + Fogarty. >6 hrs = irreversible damage. Fasciotomy if prolonged ischemia."
},
]
},
{
"title": "CASE C-2 | Blunt Trauma — Duodenal Injury",
"bg": TEAL,
"scenario": (
"A 40-year-old male, unrestrained driver, presents with epigastric pain after "
"steering wheel impact. BP 122/80, HR 88, RR 14. Abdomen mildly tender epigastric region. "
"No guarding or rigidity. FAST negative. "
"CT abdomen: thickened duodenal wall (D2/D3), retroperitoneal air, periduodenal fluid. "
"No free intraperitoneal air."
),
"questions": [
{
"q": "Q1. CT shows retroperitoneal air near the duodenum but NO intraperitoneal free air. The patient has no peritoneal signs. Explain this clinical picture — why are peritoneal signs absent?",
"marks": 2.5,
"time_s": 45,
"answer": (
"This is the CLASSIC presentation of retroperitoneal duodenal perforation.\n\n"
"Why peritoneal signs are absent:\n"
"Duodenum D2, D3, D4 are RETROPERITONEAL — they lie behind the posterior parietal peritoneum. "
"When a perforation occurs in these segments, duodenal contents (bile, fluid, air) leak "
"into the RETROPERITONEAL space, NOT into the peritoneal cavity.\n\n"
"Since the peritoneum is NOT contaminated:\n"
"• No peritoneal irritation → no guarding, no rigidity\n"
"• No intraperitoneal free air\n"
"• FAST negative (no intraperitoneal fluid)\n\n"
"Retroperitoneal air on CT (air tracking along retroperitoneal fat planes) = "
"PATHOGNOMONIC of retroperitoneal perforation (duodenum most common).\n\n"
"Teaching point: Absence of peritoneal signs does NOT exclude retroperitoneal visceral injury."
),
"why_key": "D2/D3/D4 = retroperitoneal. Leak → retro space, not peritoneum. No peritoneal contact = no peritoneal signs. CT retro air = pathognomonic."
},
{
"q": "Q2. CT confirms duodenal perforation (D2). Patient is hemodynamically stable. What is your operative management?",
"marks": 2.5,
"time_s": 55,
"answer": (
"Any evidence of perforation on imaging → EMERGENCY LAPAROTOMY.\n\n"
"Operative steps:\n"
"1. WIDE KOCHER MANEUVER — mobilize duodenum D2 (and D3) medially: incise lateral "
"peritoneum along duodenum → reflect duodenum + pancreatic head medially → full exposure.\n"
"2. Assess injury: size, location, proximity to ampulla of Vater, tissue viability.\n"
"3. Debride devitalized tissue.\n"
"4. Primary repair (most cases — up to 98% amenable):\n"
" • Single or double-layer closure with absorbable suture\n"
" • Transverse closure (to avoid narrowing) for longitudinal lacerations\n"
"5. Reinforce with omentum patch over repair.\n"
"6. Nasogastric/nasojejunal tube decompression.\n"
"7. Drain placement — allows controlled fistula if leak occurs.\n\n"
"If ampulla involved or large tissue loss:\n"
"• Billroth II or Roux-en-Y reconstruction"
),
"why_key": "Kocher = expose D2/D3. Primary repair in most cases. Omentum = reinforces suture line. Drain = controlled fistula protection."
},
{
"q": "Q3. Intraoperatively, you find a large duodenal hematoma WITHOUT perforation. The patient is stable. How do you manage this?",
"marks": 2.5,
"time_s": 45,
"answer": (
"Duodenal intramural hematoma WITHOUT perforation → usually managed CONSERVATIVELY.\n\n"
"Conservative management:\n"
"1. Nasogastric tube (NGT) decompression — decompress stomach, rest duodenum\n"
"2. NPO (nil per oral) — rest the bowel\n"
"3. Total Parenteral Nutrition (TPN) — maintain nutrition\n"
"4. Repeat contrast study (upper GI fluoroscopy or CT) at 5-7 days — check if "
"obstruction resolving.\n\n"
"If obstruction persists beyond 14 days:\n"
"→ Operative exploration — evacuate hematoma, inspect duodenal wall for hidden "
"perforation or stricture.\n\n"
"Important: If hematoma found INCIDENTALLY at laparotomy → do NOT intentionally "
"open it (risk of converting hematoma to perforation). Only open if full-thickness "
"injury suspected.\n\n"
"WHY conservative: Most hematomas reabsorb spontaneously. Surgery risks perforation."
),
"why_key": "No perforation = conservative. NGT + TPN + repeat imaging. >14 days no resolution = operate. Never open hematoma unless suspecting full-thickness injury."
},
{
"q": "Q4. Post-op Day 7 after duodenal repair: patient develops bile-stained drain output (500 mL/day). What is this complication and how do you manage it?",
"marks": 2.5,
"time_s": 45,
"answer": (
"Diagnosis: DUODENAL FISTULA (anastomotic leak / suture line failure).\n"
"Bile-stained fluid >200 mL/day from drain = duodenal fistula.\n\n"
"Management — stepwise:\n"
"1. KEEP DRAIN IN — do NOT remove. This converts it to a CONTROLLED external fistula.\n"
"2. NPO + Total Parenteral Nutrition (TPN) — complete bowel rest, maintain nutrition.\n"
"3. Skin protection — duodenal juice is caustic (bile + enzymes) → protect skin with "
"barrier cream, stomal appliance.\n"
"4. Octreotide — reduces secretion, may help fistula close.\n"
"5. CT scan — rule out undrained collection (if uncontrolled fistula = abscess risk).\n"
"6. Most controlled fistulas close spontaneously in 4-8 weeks.\n\n"
"If fistula does NOT close:\n"
"• ERCP + biliary stenting (if bile duct involvement)\n"
"• Reoperation (Roux-en-Y duodenojejunostomy) for persistent fistula."
),
"why_key": "Controlled fistula = keep drain = heals. Uncontrolled = abscess = sepsis. NPO + TPN + protect skin. Remove drain = death spiral."
},
]
},
]
},
] # end EXAMS
# ════════════════════════════════════════════════════════════════════════════
# BUILD PDF
# ════════════════════════════════════════════════════════════════════════════
doc = SimpleDocTemplate(
OUTPUT, pagesize=A4,
leftMargin=15*mm, rightMargin=15*mm,
topMargin=12*mm, bottomMargin=12*mm
)
story = []
CW = 180*mm # content width
# ── COVER PAGE ───────────────────────────────────────────────────────────────
cover = Table([[P("RETROPERITONEAL TRAUMA\nMOCK ORAL EXAMINATION", title_s)]], colWidths=[CW])
cover.setStyle(TableStyle([
("BACKGROUND",(0,0),(-1,-1), RED),
("TOPPADDING",(0,0),(-1,-1), 12),
("BOTTOMPADDING",(0,0),(-1,-1), 12),
("ROUNDEDCORNERS",[5]),
]))
story.append(cover)
story.append(Spacer(1, 4*mm))
info_data = [
[P("<b>Format:</b> 2 Cases × 4 Questions per exam set", instr_s),
P("<b>Time:</b> 7 minutes total", instr_s)],
[P("<b>Marks:</b> 2.5 pts per question → 20 pts total", instr_s),
P("<b>Pass:</b> 12 / 20 (5 correct questions)", instr_s)],
[P("<b>Sets included:</b> SET A, SET B, SET C (6 cases, 24 questions)", instr_s),
P("<b>Tip:</b> Talk with partner before answering!", instr_s)],
]
info_t = Table(info_data, colWidths=[90*mm, 90*mm])
info_t.setStyle(TableStyle([
("BACKGROUND",(0,0),(-1,-1), LTYELLOW),
("BOX",(0,0),(-1,-1), 1, ORANGE),
("INNERGRID",(0,0),(-1,-1), 0.3, MIDGRAY),
("TOPPADDING",(0,0),(-1,-1), 4),
("BOTTOMPADDING",(0,0),(-1,-1), 4),
("LEFTPADDING",(0,0),(-1,-1), 6),
("RIGHTPADDING",(0,0),(-1,-1), 6),
]))
story.append(info_t)
story.append(Spacer(1, 4*mm))
# time strategy box
strat_data = [[
P("⏱ TIME STRATEGY", hdr_s),
P("~50 sec / question", center_s),
P("Partner: whisper answer (10 sec) → confirm → speak", center_s),
P("Never skip — guess earns more than zero!", center_s),
]]
strat_t = Table(strat_data, colWidths=[32*mm, 32*mm, 72*mm, 44*mm])
strat_t.setStyle(TableStyle([
("BACKGROUND",(0,0),(0,0), ORANGE),
("BACKGROUND",(1,0),(-1,0), LTORANGE),
("BOX",(0,0),(-1,-1), 0.8, ORANGE),
("INNERGRID",(0,0),(-1,-1), 0.3, MIDGRAY),
("VALIGN",(0,0),(-1,-1),"MIDDLE"),
("TOPPADDING",(0,0),(-1,-1), 4),
("BOTTOMPADDING",(0,0),(-1,-1), 4),
("LEFTPADDING",(0,0),(-1,-1), 5),
]))
story.append(strat_t)
story.append(Spacer(1, 3*mm))
story.append(HR())
story.append(P("INSTRUCTIONS: Read each case carefully. Discuss with your partner. State your answer clearly. Remember — one answer, final. Time yourself with the timer shown for each question.", instr_s))
story.append(HR())
# ── EXAM SETS ────────────────────────────────────────────────────────────────
for ei, exam in enumerate(EXAMS):
story.append(PageBreak())
# SET TITLE BAR
set_t = Table([[P(exam["title"], title_s)]], colWidths=[CW])
set_t.setStyle(TableStyle([
("BACKGROUND",(0,0),(-1,-1), exam["color"]),
("TOPPADDING",(0,0),(-1,-1), 8),
("BOTTOMPADDING",(0,0),(-1,-1), 8),
]))
story.append(set_t)
story.append(Spacer(1, 3*mm))
for ci, case in enumerate(exam["cases"]):
# CASE HEADER
case_t = Table([[P(case["title"], case_s)]], colWidths=[CW])
case_t.setStyle(TableStyle([
("BACKGROUND",(0,0),(-1,-1), case["bg"]),
("TOPPADDING",(0,0),(-1,-1), 5),
("BOTTOMPADDING",(0,0),(-1,-1), 5),
("LEFTPADDING",(0,0),(-1,-1), 6),
]))
story.append(case_t)
story.append(Spacer(1, 1.5*mm))
# SCENARIO BOX
scen_t = Table([[P(case["scenario"], scenario_s)]], colWidths=[CW])
scen_t.setStyle(TableStyle([
("BACKGROUND",(0,0),(-1,-1), LIGHTGRAY),
("BOX",(0,0),(-1,-1), 0.8, case["bg"]),
("TOPPADDING",(0,0),(-1,-1), 5),
("BOTTOMPADDING",(0,0),(-1,-1), 5),
("LEFTPADDING",(0,0),(-1,-1), 7),
("RIGHTPADDING",(0,0),(-1,-1), 7),
]))
story.append(scen_t)
story.append(Spacer(1, 2*mm))
# QUESTIONS
for qi, qdata in enumerate(case["questions"]):
qnum = qi + 1
marks_label = f"2.5 pts"
timer_label = f"⏱ {qdata['time_s']} sec"
# Question header row
qhdr_data = [[
P(f"Q{qnum}", qnum_s),
P(qdata["q"], q_s),
P(marks_label, pts_s),
P(timer_label, timer_s),
]]
qhdr_t = Table(qhdr_data, colWidths=[10*mm, 132*mm, 18*mm, 20*mm])
qhdr_t.setStyle(TableStyle([
("BACKGROUND",(0,0),(0,0), case["bg"]),
("BACKGROUND",(1,0),(1,0), LTBLUE),
("BACKGROUND",(2,0),(2,0), GREEN),
("BACKGROUND",(3,0),(3,0), LTORANGE),
("BOX",(0,0),(-1,-1), 0.8, case["bg"]),
("INNERGRID",(0,0),(-1,-1), 0.3, MIDGRAY),
("VALIGN",(0,0),(-1,-1),"MIDDLE"),
("TOPPADDING",(0,0),(-1,-1), 4),
("BOTTOMPADDING",(0,0),(-1,-1), 4),
("LEFTPADDING",(0,0),(-1,-1), 4),
("RIGHTPADDING",(0,0),(-1,-1), 4),
("ALIGN",(2,0),(3,0),"CENTER"),
]))
story.append(qhdr_t)
# ANSWER BOX
ans_lines = qdata["answer"].split("\n")
ans_content = []
for line in ans_lines:
line = line.strip()
if line:
if line.startswith("Step") or line.startswith("•") or line.startswith("1.") or line.startswith("2.") or line.startswith("3.") or line.startswith("4.") or line.startswith("5.") or line.startswith("Stage") or line.startswith("Grade"):
ans_content.append(P(f" {line}", ans_s))
elif "WHY" in line and ":" in line:
ans_content.append(P(line, why_s))
elif line.endswith(":") or (len(line) < 60 and line.isupper()):
ans_content.append(P(line, ans_bold_s))
else:
ans_content.append(P(line, ans_s))
why_note = P(f"KEY INSIGHT: {qdata['why_key']}", why_s)
all_ans = ans_content + [Spacer(1,2), HR(), why_note]
ans_t = Table([[all_ans]], colWidths=[CW])
ans_t.setStyle(TableStyle([
("BACKGROUND",(0,0),(-1,-1), WHITE),
("BOX",(0,0),(-1,-1), 0.5, MIDGRAY),
("TOPPADDING",(0,0),(-1,-1), 4),
("BOTTOMPADDING",(0,0),(-1,-1), 4),
("LEFTPADDING",(0,0),(-1,-1), 7),
("RIGHTPADDING",(0,0),(-1,-1), 7),
("VALIGN",(0,0),(-1,-1),"TOP"),
]))
story.append(ans_t)
story.append(Spacer(1, 3*mm))
if ci == 0:
# divider between cases
story.append(HR())
story.append(Spacer(1, 2*mm))
# Score table at end of each set
score_t = Table([
[P("CASE", hdr_s), P("Q1", hdr_s), P("Q2", hdr_s), P("Q3", hdr_s), P("Q4", hdr_s), P("SUBTOTAL", hdr_s)],
[P(f"Case {exam['title'][-5:-3]}1", bold_center_s),
P("__ / 2.5", center_s), P("__ / 2.5", center_s), P("__ / 2.5", center_s), P("__ / 2.5", center_s), P("__ / 10", bold_center_s)],
[P(f"Case {exam['title'][-5:-3]}2", bold_center_s),
P("__ / 2.5", center_s), P("__ / 2.5", center_s), P("__ / 2.5", center_s), P("__ / 2.5", center_s), P("__ / 10", bold_center_s)],
[P("TOTAL", hdr_s), P("", center_s), P("", center_s), P("", center_s), P("", center_s), P("__ / 20", pts_s)],
], colWidths=[30*mm, 25*mm, 25*mm, 25*mm, 25*mm, 30*mm])
score_t.setStyle(TableStyle([
("BACKGROUND",(0,0),(-1,0), exam["color"]),
("BACKGROUND",(0,3),(-1,3), exam["color"]),
("BACKGROUND",(0,1),(-1,2), LTYELLOW),
("BOX",(0,0),(-1,-1), 1, exam["color"]),
("INNERGRID",(0,0),(-1,-1), 0.4, MIDGRAY),
("TOPPADDING",(0,0),(-1,-1), 3),
("BOTTOMPADDING",(0,0),(-1,-1), 3),
("SPAN",(1,3),(4,3)),
("VALIGN",(0,0),(-1,-1),"MIDDLE"),
("ALIGN",(0,0),(-1,-1),"CENTER"),
]))
story.append(Spacer(1, 4*mm))
story.append(score_t)
doc.build(story)
print(f"Mock exam PDF created: {OUTPUT}")
cd /home/daytona/workspace/retroperitoneal-cheatsheet && python generate_mockexam.py 2>&1
ls -lh /home/daytona/workspace/retroperitoneal-cheatsheet/
Retroperitoneal Mock Exam
PDF Document · PDF
Mock Exam lo emi undi:
| Set | Case 1 | Case 2 |
|---|---|---|
| 🔵 SET A | Blunt trauma — unstable, Zone 1 hematoma, ACS | Penetrating stab wound — renal injury, urinoma |
| 🟢 SET B | Pelvic fracture — open-book, Zone 3 bleeding | Seat belt — pancreatic transection, POPF |
| 🟣 SET C | GSW — aortic injury, iliac, acute ischemia | Blunt — duodenal perforation, fistula |
- ⏱ Timer shown (45-55 sec each)
- 2.5 pts label
- Full model answer
- KEY INSIGHT — "WHY" highlight in green
- Partner ki case cheppu — 2 min think time
- Timer start cheyyi
- Answer cheppi compare cheyyo model answer tho
- Score card fill cheyyi
How identify which zone or all zones or at what zone and what organs might involve in particular zone and immediate treatment or management give in tabular format and what type of injury
🗺️ HOW TO IDENTIFY THE ZONE + ORGANS + INJURY TYPE + MANAGEMENT
📍 STEP 1 — HOW TO IDENTIFY WHICH ZONE?
"Doctor case istinapratisar — zone ela identify cheyyadam?"
| CLUE | THINK ZONE | WHY |
|---|---|---|
| Central abdomen injury / epigastric / periumbilical | Zone 1 | Midline = aorta/IVC territory |
| Flank injury (right or left) | Zone 2 | Lateral = kidney territory |
| Pelvic fracture on X-ray | Zone 3 | Pelvis = iliac vessels |
| Stab wound to back | Could be any zone | Track direction matters — CT needed |
| Steering wheel / seat belt epigastric | Zone 1 or Zone 2 | Central compression |
| High-speed deceleration | Zone 1 (aorta shear) | Aortic hiatus tearing |
| GSW traversing midline | Zone 1 ± Zone 2 | Track crosses midline |
| Open-book pelvic fracture | Zone 3 | Pelvic ring disruption = pelvic veins |
| Flank bruising / Grey Turner sign | Zone 2 | Retroperitoneal blood tracks to flank |
| Seat belt sign + amylase elevated | Zone 1/2 (pancreas) | Pancreatic neck = over spine |
| Hematuria | Zone 2 (kidney/ureter) | Genitourinary = lateral retro |
🟥 ZONE 1 — Central Retroperitoneum
Location: Midline — Aortic hiatus → Iliac bifurcation
| Sub-zone | Landmarks | Structures |
|---|---|---|
| Supramesocolic | Above transverse mesocolon | Suprarenal Aorta, Celiac axis, Proximal SMA, Suprarenal IVC, Proximal SMV, Proximal renal arteries |
| Inframesocolic | Below transverse mesocolon | Infrarenal Aorta, Distal SMA, IMA, Infrarenal IVC, Distal SMV |
Organs at Risk in Zone 1:
| Organ / Structure | Type of Injury | How to Identify (Clinical + Imaging) |
|---|---|---|
| Abdominal Aorta | Laceration, transection, pseudoaneurysm | Pulsatile hematoma, BP uncontrollable, CT: contrast jet |
| Inferior Vena Cava (IVC) | Laceration, avulsion | Non-pulsatile expanding hematoma, rising venous pressure |
| Celiac axis | Avulsion, laceration | Epigastric blunt trauma, CT: celiac branch injury |
| SMA / SMV | Laceration, thrombosis | Bowel ischemia signs, elevated lactate, CT: no bowel enhancement |
| Pancreas (body/neck) | Contusion, transection, duct injury | Seat belt sign, elevated amylase >3h, CT: pancreatic hypodense line |
| Duodenum (D2-D4) | Hematoma, perforation | No peritoneal signs!, CT: retroperitoneal air, periduodenal fluid |
Zone 1 — Injury Type + Management:
| Injury Type | Mechanism | Immediate Management |
|---|---|---|
| Blunt | MVA deceleration, steering wheel | ✅ ALWAYS EXPLORE — proximal aortic control first |
| Penetrating | GSW, stab | ✅ ALWAYS EXPLORE — all penetrating Zone 1 |
| Exposure | — | Mattox maneuver (supramesocolic left side) / Cattell-Braasch (infrarenal right) |
| Aortic laceration | Primary repair (Prolene) or patch | Proximal clamp at diaphragm → lateral arteriorrhaphy |
| IVC laceration | Lateral venorrhaphy | If >30% narrowing → patch; infrarenal IVC can be ligated |
| Pancreatic duct injury (Gr III) | Distal pancreatectomy ± splenectomy | Kocher + gastrocolic ligament division |
| Duodenal perforation | Emergency laparotomy + Kocher + primary repair | NPO if hematoma only |
🟧 ZONE 2 — Lateral Retroperitoneum (Bilateral)
Location: Both lateral gutters (left and right sides)
Organs at Risk in Zone 2:
| Organ / Structure | Type of Injury | How to Identify |
|---|---|---|
| Kidneys | Contusion, laceration (Gr 1-5), shattered | Hematuria (gross or microscopic + hypotension), CT urogram, flank pain |
| Adrenal glands | Contusion, hemorrhage | CT: adrenal hematoma, usually incidental |
| Renal artery | Thrombosis, avulsion, pseudoaneurysm | Absent renal enhancement on CT ("non-perfused kidney"), late hypertension |
| Renal vein | Laceration | Zone 2 expanding hematoma, hematuria |
| Proximal ureters | Avulsion, laceration | Hematuria (may be absent!), CT urogram shows extravasation, urinoma |
Zone 2 — Injury Type + Management:
| Injury Type | Mechanism | Immediate Management |
|---|---|---|
| Blunt | MVA flank impact, fall | Observe IF stable + non-expanding + no urine leak. Open if pulsatile/expanding |
| Penetrating | GSW, stab flank | ✅ ALWAYS EXPLORE — all penetrating |
| Key step if operating | — | Medial renal vascular control FIRST before opening hematoma |
| Renal Gr 1-3 | Conservative | Bed rest, monitoring, repeat CT |
| Renal Gr 4 | CT-guided observation / stent urine leak | Nephrostomy/stent if collecting system injury |
| Renal Gr 5 (shattered/pedicle avulsion) | Surgery | Nephrectomy — confirm contralateral kidney first! |
| Renal artery thrombosis | Repair if <1 hr ischemia | >1 hr = nephrectomy (irreversible damage) |
| Ureteral injury | Stent (stable) / ligate + nephrostomy (unstable) | Formal repair delayed until stable |
🟩 ZONE 3 — Pelvic Retroperitoneum
Location: Below iliac bifurcation → Pelvic cavity
Organs at Risk in Zone 3:
| Organ / Structure | Type of Injury | How to Identify |
|---|---|---|
| Common / External / Internal Iliac arteries | Laceration, avulsion | Penetrating: pulsatile hematoma. Blunt: rare arterial, CT angio shows blush |
| Iliac veins / Pelvic venous plexus | Laceration, avulsion | Pelvic fracture + hemodynamic instability + FAST negative |
| Bladder | Rupture (intra or extraperitoneal) | Gross hematuria, inability to void, CT cystogram: extravasation |
| Urethra | Disruption | Blood at meatus, perineal hematoma, inability to catheterize |
| Rectum (lower) | Perforation | Rectal exam: blood, penetrating wound trajectory |
| Sacral vessels | Hemorrhage | Sacral fracture pattern on X-ray/CT |
Zone 3 — Injury Type + Management:
| Injury Type | Mechanism | Immediate Management |
|---|---|---|
| Blunt (MOST IMPORTANT!) | Pelvic fracture (MVA) | ❌ DO NOT OPEN hematoma — tamponade must be preserved |
| Blunt — immediate | — | Pelvic binder → External pelvic fixation → Preperitoneal packing |
| Blunt — arterial blush on CT | — | Angiography + selective embolization |
| Blunt — in extremis | — | REBOA (Zone 3 balloon) or internal iliac ligation |
| Penetrating | GSW, stab pelvis | ✅ ALWAYS EXPLORE — identify specific vessel/bowel/ureter injury |
| Iliac artery injury (penetrating) | Primary repair or interposition graft | Damage control shunt if lethal triad |
| Bladder rupture — intraperitoneal | Surgical repair (2-layer) | Foley catheter + suprapubic drain |
| Bladder rupture — extraperitoneal | Foley catheter drainage alone (mostly) | Surgery only if neck involved |
| Urethral disruption | DO NOT force catheter → Suprapubic cystostomy | Delayed urethroplasty |
📊 MASTER SUMMARY TABLE — All Zones at a Glance
| Feature | ZONE 1 | ZONE 2 | ZONE 3 |
|---|---|---|---|
| Location | Central midline | Bilateral lateral | Pelvis |
| Key vessels | Aorta, IVC, SMA, SMV, Celiac | Renal A/V | Iliac A/V |
| Key organs | Duodenum, Pancreas | Kidneys, Adrenals, Ureters | Bladder, Urethra, Rectum |
| Identify by | Central injury, pulsatile hematoma, epigastric trauma | Hematuria, flank injury, Zone 2 hematoma on CT | Pelvic fracture X-ray, FAST–ve unstable, blood at meatus |
| Blunt — explore? | ✅ YES always | Only if expanding/pulsatile/urine leak | ❌ NO — never open |
| Penetrating — explore? | ✅ YES always | ✅ YES always | ✅ YES always |
| Surgical exposure | Mattox (L) / Cattell-Braasch (R) | Medial renal vascular control | Direct exploration / packing |
| #1 danger | Aorta/IVC exsanguination | Nephrectomy if tamponade lost | Tamponade lost → massive bleed |
| Special non-op option | No | Angioembolization (Gr 4-5 stable) | Angioembolization (arterial blush) |
| WHY not open Zone 3 blunt? | N/A | N/A | Venous bleeding — pelvic tamponade = life |
⚡ CLINICAL CLUE → ZONE IDENTIFICATION (Exam Speed Table)
| What doctor says in the case | Your zone answer |
|---|---|
| "Pulsatile midline hematoma" | Zone 1 |
| "Central non-pulsatile expanding hematoma" | Zone 1 |
| "Hematuria + flank hematoma" | Zone 2 |
| "Pelvic fracture + hemodynamic instability" | Zone 3 |
| "Retroperitoneal air near duodenum" | Zone 1 (duodenal injury) |
| "Seat belt sign + amylase elevated" | Zone 1 (pancreatic injury) |
| "Grey Turner sign" (flank bruising) | Zone 2 (retroperitoneal blood) |
| "Blood at urethral meatus" | Zone 3 (urethral injury) |
| "Non-perfused kidney on CT" | Zone 2 (renal pedicle injury) |
| "Open-book pelvic fracture + FAST –ve" | Zone 3 |
| "GSW traversing midline" | Zone 1 ± Zone 2 |
| "Stab to back" | Any zone — CT to determine |
- Clue identify (location + mechanism + findings)
- Zone cheppu
- Organs at risk list cheyyi
- Blunt vs Penetrating — explore or not
- Exposure maneuver cheppu
- WHY explain cheyyi 💪🔥
Management and diagnosis a kind of injury or hematoma lo ela cheyyali and doc why emdhuku adhi ichav ani vati pharmacokinetics and metabolism anni adugutharu tell in tabular format
💊 RETROPERITONEAL TRAUMA — COMPLETE MANAGEMENT + DRUGS + PHARMACOKINETICS
Tabular Format — Oral Exam Ready
🩺 PART 1: INJURY / HEMATOMA TYPE → HOW TO DIAGNOSE
| Injury / Hematoma Type | How to Identify Clinically | Imaging Findings | What Zone? |
|---|---|---|---|
| Aortic injury | Uncontrollable hypotension, pulsatile midline hematoma | CT: contrast jet/extravasation, aortic wall disruption | Zone 1 |
| IVC laceration | Non-pulsatile expanding hematoma, raised CVP, cyanosis lower limbs | CT: retroperitoneal hematoma, right side, IVC wall defect | Zone 1 |
| Renal laceration | Gross hematuria, flank pain, Grey Turner sign | CT urogram: Grade 1-5 lac, contrast extravasation, urinoma | Zone 2 |
| Renal artery thrombosis | Hematuria MAY BE ABSENT, flank pain | CT: non-perfused kidney (no enhancement), "white kidney" sign | Zone 2 |
| Pancreatic transection | Seat belt sign, epigastric pain, NO peritoneal signs early | CT: hypodense line across neck, peripancreatic fluid. Amylase >3h | Zone 1 |
| Duodenal perforation | No peritoneal signs (classic!), epigastric pain post-RTA | CT: retroperitoneal FREE AIR, periduodenal fluid, wall thickening | Zone 1 |
| Duodenal hematoma | Epigastric pain, vomiting (obstruction), no free air | CT: intramural hyperdense mass, "coil spring" sign on UGI | Zone 1 |
| Pelvic hematoma | Pelvic fracture X-ray, FAST negative, hemodynamic instability | CT: pelvic hematoma, arterial blush if arterial source | Zone 3 |
| Ureteral injury | Hematuria (may be absent!), flank pain, urinoma delayed | CT urogram: extravasation, urinoma, delayed pyelogram absent | Zone 2 |
| Pancreatic fistula (post-op) | Drain fluid amylase >3× serum amylase on/after POD 3 | CT: peripancreatic fluid collection, drain output elevated | Zone 1 (post-op) |
🔴 PART 2: HEMATOMA MANAGEMENT — EXPLORE OR NOT?
| Hematoma | Mechanism | Explore? | Why? | What to Do |
|---|---|---|---|---|
| Zone 1 | Blunt | ✅ YES | Aorta/IVC/SMA — life-threatening vascular injury | Proximal control → Mattox or Cattell-Braasch → repair |
| Zone 1 | Penetrating | ✅ YES | Any penetrating = direct vessel injury | Explore immediately after proximal control |
| Zone 2 | Blunt | ⚠️ ONLY IF expanding / pulsatile / urine leak | Perinephric tamponade — opening loses it → nephrectomy rate increases | Medial renal vascular control → renorrhaphy or nephrectomy |
| Zone 2 | Penetrating | ✅ YES | Arterial injury likely — direct damage to renal pedicle | Medial control first → repair/nephrectomy |
| Zone 3 | Blunt | ❌ NEVER | Pelvic venous plexus bleeding — retroperitoneal tamponade = life | Pelvic binder → external fixation → preperitoneal packing → angioembolization |
| Zone 3 | Penetrating | ✅ YES | Iliac artery/vein injury — must control | Proximal/distal iliac control → primary repair / shunt |
💉 PART 3: DRUGS GIVEN IN RETROPERITONEAL TRAUMA MANAGEMENT
🅰️ DRUG 1: TRANEXAMIC ACID (TXA)
| Feature | Detail |
|---|---|
| Drug class | Antifibrinolytic agent |
| Indication | Trauma-induced coagulopathy (TIC) with significant hemorrhage; SBP <110 or HR >110 |
| Dose | 1g IV over 10 min (loading), then 1g IV over 8 hours |
| Time window | MUST give within 3 hours of injury — after 3 hrs it may cause HARM |
| Mechanism of Action | TXA is a synthetic lysine analogue. It competitively inhibits plasminogen activation by blocking lysine-binding sites on plasminogen → prevents conversion of plasminogen → plasmin → plasmin cannot cleave fibrin clot → antifibrinolysis → clot is preserved |
| WHY give it? | In trauma: hypoperfusion → endothelium releases tPA (tissue plasminogen activator) → activated Protein C consumes PAI-1 → excess tPA → hyperfibrinolysis → existing clots dissolve → uncontrolled bleeding. TXA blocks this pathway |
| Pharmacokinetics | Oral bioavailability: ~30-50%. IV used in trauma. Vd: 9-12 L. Protein binding: 3% (low) |
| Metabolism | Minimally metabolized in liver. Excreted UNCHANGED in urine (>95%) — renal excretion |
| Half-life | ~2 hours |
| Elimination | Renal — dose reduce in renal failure |
| WHY NOT after 3 hours? | Late TXA → pro-thrombotic (CRASH-2 data) → increased mortality. Early hyperfibrinolysis phase has passed by 3 hrs |
| Study | CRASH-2 Trial — 20,000 patients, significantly reduced death from hemorrhage when given <3 hrs |
🅱️ DRUG 2: FRESH FROZEN PLASMA (FFP)
| Feature | Detail |
|---|---|
| What it is | Contains ALL clotting factors (I, II, V, VII, VIII, IX, X, XI, XIII) + Protein C, S |
| Indication | Trauma-induced coagulopathy — replace clotting factors; given with pRBC in MTP |
| Dose / Ratio | 1:1:1 ratio — 1 unit pRBC : 1 unit FFP : 1 unit platelets (Massive Transfusion Protocol) |
| Mechanism | Replaces consumed/diluted clotting factors → restores coagulation cascade → fibrin clot formation |
| WHY 1:1:1? | Military data showed fresh whole blood reduces mortality. Civilian equivalent = 1:1:1 component therapy to "reconstitute whole blood" |
| WHY NOT just crystalloids? | Crystalloids cause: (1) Hemodilution → dilution coagulopathy, (2) Hypothermia, (3) Acidosis → worsens lethal triad → MORE bleeding |
| Storage | Frozen at -18°C; thaw before use |
| Pharmacokinetics | Not a drug — biological product. Clotting factors have variable half-lives (Factor VII shortest: ~4-6 hrs) |
| WHY calcium with MTP? | pRBC + FFP contain citrate as anticoagulant preservative. Citrate chelates (binds) calcium → hypocalcemia → calcium needed for coagulation cascade (Factor IV) → give CaCl₂ |
🅲 DRUG 3: CALCIUM CHLORIDE (CaCl₂)
| Feature | Detail |
|---|---|
| Indication | Massive transfusion → citrate-induced hypocalcemia; cardiac dysfunction in shock |
| Dose | 1g IV (10 mL of 10% CaCl₂) for each 4 units of blood products; monitor ionized Ca²⁺ |
| Target | Ionized calcium ≥ 0.9 mmol/L |
| Mechanism | Ca²⁺ is Factor IV in coagulation cascade — essential for tenase and prothrombinase complexes. Also needed for cardiac contractility (excitation-contraction coupling) and vascular smooth muscle tone |
| WHY CaCl₂ preferred over Calcium Gluconate? | CaCl₂ provides calcium directly (272 mg elemental Ca/10mL). Calcium gluconate requires liver metabolism to release free calcium — injured/hypoperfused liver in trauma may not metabolize it efficiently → CaCl₂ more reliable |
| Pharmacokinetics | IV → immediate ionization. Distributed throughout ECF. No hepatic metabolism. Renally excreted |
| Half-life | Not applicable (elemental ion) |
| Caution | Extravasation causes tissue necrosis — give through central line ideally |
🅳 DRUG 4: OCTREOTIDE (Somatostatin Analogue)
| Feature | Detail |
|---|---|
| Indication | Pancreatic fistula (post-op); reduce pancreatic secretion after pancreatic trauma/surgery |
| Dose | 100-200 mcg SC/IV TID or continuous infusion 25-50 mcg/hr |
| Mechanism | Octreotide is a synthetic analogue of somatostatin (longer acting). Binds somatostatin receptors (SSTR 1-5) on pancreatic acinar and ductal cells → inhibits secretin + CCK stimulated pancreatic exocrine secretion → reduces pancreatic enzyme and bicarbonate output → less fluid through injured duct → fistula output reduces → healing |
| WHY give it? | Pancreatic fistula = duct leak → enzymes flowing = autodigestion of surrounding tissue. Less secretion = less flow through leak = fistula closes faster |
| Pharmacokinetics | SC bioavailability: ~100%. Vd: 14 L. Protein binding: 65% (albumin, lipoproteins) |
| Metabolism | ~32% excreted unchanged in urine. Rest metabolized in liver by oxidation |
| Half-life | 1.5-2 hours (vs natural somatostatin half-life: 1-3 minutes) — octreotide much longer acting |
| Elimination | Renal + hepatic |
| WHY not natural somatostatin? | Natural somatostatin half-life = 1-3 minutes — impractical clinically. Octreotide half-life = ~2 hours — can give TID |
🅴 DRUG 5: HEPARIN (Unfractionated)
| Feature | Detail |
|---|---|
| Indication | Acute limb ischemia after vascular repair; vascular repair anticoagulation |
| Dose | 80-100 units/kg IV bolus before vascular clamp application; systemic anticoagulation 5000 units bolus + infusion |
| Mechanism | Heparin binds Antithrombin III (AT-III) → conformational change in AT-III → AT-III now rapidly inhibits Thrombin (IIa) and Factor Xa (1000× faster) → prevents fibrin clot formation → anticoagulation |
| WHY give in vascular repair? | Clamp application causes stasis distal to clamp → thrombus forms → ischemia worsens. Heparin prevents thrombus formation during clamp time → better outcome for distal tissue |
| Pharmacokinetics | IV only (poor oral absorption — large charged molecule). Vd: low (stays in vascular space) |
| Metabolism | Metabolized by heparinase in liver + reticuloendothelial system. Also cleared by kidneys at high doses |
| Half-life | Dose-dependent: 25 units/kg → ~30 min; 400 units/kg → ~150 min |
| Monitoring | aPTT (target 60-100 sec, 1.5-2.5× normal) |
| Reversal | Protamine sulphate — 1mg neutralizes 100 units heparin (positively charged protein binds negatively charged heparin → inactive complex) |
| WHY protamine works? | Heparin = negatively charged. Protamine = positively charged → ionic binding → neutralization |
🅵 DRUG 6: NOREPINEPHRINE / VASOPRESSIN (Vasopressors)
| Feature | NE (Norepinephrine) | Vasopressin |
|---|---|---|
| Indication | Distributive/vasodilatory shock after hemorrhage control; refractory hypotension | Refractory shock; adjunct to NE |
| Dose | 0.1-2 mcg/kg/min IV infusion | 0.03-0.04 units/min IV (fixed low dose) |
| Mechanism | Agonist at α1 adrenoceptors (vascular smooth muscle) → vasoconstriction → ↑SVR → ↑BP. Also β1 activity → ↑HR, ↑contractility | Binds V1 receptors (vascular) → vasoconstriction. V2 receptors (renal collecting duct) → water reabsorption → ↑blood volume |
| WHY give in trauma? | After massive hemorrhage → catecholamine depletion → vasodilation. NE restores SVR → maintains perfusion pressure | NE-refractory shock → vasopressin levels depleted in prolonged shock → exogenous vasopressin restores vascular tone |
| Pharmacokinetics | IV only. Vd: low. Does NOT cross BBB | IV only. Vd: 0.14 L/kg |
| Metabolism | MAO + COMT enzymes → metabolites excreted in urine | Enzymatic degradation by vasopressinase (liver, kidney, plasma) |
| Half-life | ~2 minutes (very short — must give as infusion) | 10-35 minutes |
| WHY short half-life? | Rapid inactivation by MAO and COMT at nerve terminals and liver → allows precise titration | Peptide — rapidly cleaved |
| Caution | Can cause peripheral ischemia if extravasates | Fixed dose only — higher doses cause coronary ischemia |
🅶 DRUG 7: ANTIBIOTICS (Broad Spectrum — Piperacillin-Tazobactam / Cefazolin)
| Feature | Detail |
|---|---|
| Indication | Penetrating trauma with bowel contamination; prophylaxis for laparotomy |
| Drug | Cefazolin (prophylaxis, clean cases); Pip-Tazo (contaminated: bowel injury, retroperitoneal abscess) |
| Mechanism — Cefazolin | Beta-lactam → binds Penicillin Binding Proteins (PBPs) → inhibits transpeptidation → prevents bacterial cell wall (peptidoglycan) cross-linking → cell lysis |
| Mechanism — Pip-Tazo | Piperacillin = extended-spectrum beta-lactam (PBP inhibitor). Tazobactam = beta-lactamase inhibitor (protects piperacillin from enzymatic degradation by resistant bacteria) |
| Pharmacokinetics — Pip-Tazo | IV. Low protein binding (~30%). Vd: 0.24 L/kg. Minimal hepatic metabolism |
| Metabolism | Piperacillin: small hepatic metabolism. Tazobactam: minimally metabolized |
| Elimination | Predominantly renal — dose adjust in renal failure |
| Half-life | Piperacillin: ~1 hour; Tazobactam: ~1 hour |
| WHY broad spectrum here? | Bowel injury = mixed gram-positive + gram-negative + anaerobic organisms. Pip-Tazo covers all three spectrums |
📊 PART 4: MASTER DRUG TABLE — QUICK ORAL REFERENCE
| Drug | Class | Mechanism (1 line) | WHY Used in Trauma | Half-life | Metabolism | Elimination |
|---|---|---|---|---|---|---|
| Tranexamic Acid | Antifibrinolytic | Blocks plasminogen → plasmin conversion → preserves fibrin clot | Trauma hyperfibrinolysis → clot dissolves → bleeding | 2 hrs | Minimal hepatic | Renal (95% unchanged) |
| FFP | Blood product | Replaces all clotting factors | Dilutional coagulopathy in MTP | Factor-specific | N/A | N/A |
| Calcium Chloride | Electrolyte | Factor IV in coagulation + cardiac contractility | Citrate chelates Ca in MTP → hypocalcemia | Elemental ion | None | Renal |
| Octreotide | Somatostatin analogue | SSTR binding → inhibits pancreatic exocrine secretion | Pancreatic fistula → reduce duct flow → fistula closes | 1.5-2 hrs | 32% renal unchanged, rest hepatic | Renal + hepatic |
| Heparin | Anticoagulant | Activates AT-III → inhibits Thrombin + Xa | Vascular clamp → stasis → thrombus → ischemia prevention | Dose-dependent 30-150 min | Heparinase (liver + RES) | Renal (high dose) |
| Norepinephrine | Vasopressor | α1 agonist → vasoconstriction → ↑SVR | Post-hemorrhage vasodilation, catecholamine depletion | ~2 min | MAO + COMT | Urinary metabolites |
| Vasopressin | Vasopressor | V1 receptor → vascular constriction | NE-refractory shock, vasopressin depletion in prolonged shock | 10-35 min | Vasopressinase (liver, kidney) | Renal |
| Cefazolin | Beta-lactam antibiotic | Inhibits PBP → blocks cell wall synthesis | Surgical prophylaxis — laparotomy | ~1.8 hrs | Minimal | Renal (unchanged) |
| Pip-Tazo | Beta-lactam + BLI | Pip inhibits PBP; Tazo protects from beta-lactamase | Contaminated trauma with bowel injury | ~1 hr | Minimal hepatic | Renal |
| Protamine | Heparin reversal | Ionic binding to heparin → inactive complex | Reverse heparin after vascular repair | ~7 min | Unknown | Unknown |
⚡ "WHY DID YOU GIVE THAT?" — Oral Quick Answers
| Doctor asks | Your answer |
|---|---|
| "Why TXA within 3 hours?" | After 3 hrs hyperfibrinolysis phase over — late TXA is pro-thrombotic and increases mortality (CRASH-2 data) |
| "Why 1:1:1 ratio in MTP?" | Reconstitutes whole blood — prevents dilutional coagulopathy — military data shows improved survival |
| "Why CaCl₂ not calcium gluconate in trauma?" | CaCl₂ = direct elemental calcium. Gluconate needs functioning liver to release free calcium — trauma liver may be hypoperfused/damaged |
| "Why heparin before vascular clamp?" | Clamp → stasis distal → thrombus → limb ischemia. Heparin activates AT-III → inhibits thrombin + Xa → prevents clamp-related thrombosis |
| "Why octreotide for pancreatic fistula?" | SSTR binding → inhibits CCK + secretin → reduces pancreatic exocrine output → less flow through duct leak → fistula closes spontaneously |
| "Why NOT crystalloids in trauma resuscitation?" | Hemodilution → dilutional coagulopathy + hypothermia + acidosis = worsens lethal triad. "Popping the clot" → more bleeding |
| "Why protamine reverses heparin?" | Protamine positively charged, heparin negatively charged → ionic neutralization → inactive complex |
| "Why permissive hypotension target SBP 90?" | Higher pressure pops clot → more bleeding. Lower pressure → inadequate organ perfusion. 90 mmHg = balance. NOT in TBI patients! |
| "Why vasopressin added to NE?" | Prolonged shock depletes endogenous vasopressin (relative vasopressin deficiency). Exogenous vasopressin restores V1-mediated vasoconstriction — NE-sparing effect |
- Mechanism → Target receptor/enzyme/pathway cheppu
- PK → Half-life + protein binding
- Metabolism → Liver? Renal? Unchanged?
- WHY this drug → Context specific reason
A grade hematoma ani adigithe adhi ela cheppali
🏆 AAST GRADE HEMATOMA / INJURY — ELA CHEPPALI?
(Oral exam lo doctor "Grade cheppu" antu adginapratisar — ee format lo answer cheyyi!)
🧠 ANSWER FRAMEWORK — Grade adginapratisar
"Sir, this is an AAST Grade [X] injury. It is characterized by [description]. Based on this grade and the [blunt/penetrating] mechanism, management is [conservative/operative] because [WHY]."
🔵 ORGAN 1: KIDNEY — AAST Grading (Most Commonly Asked!)
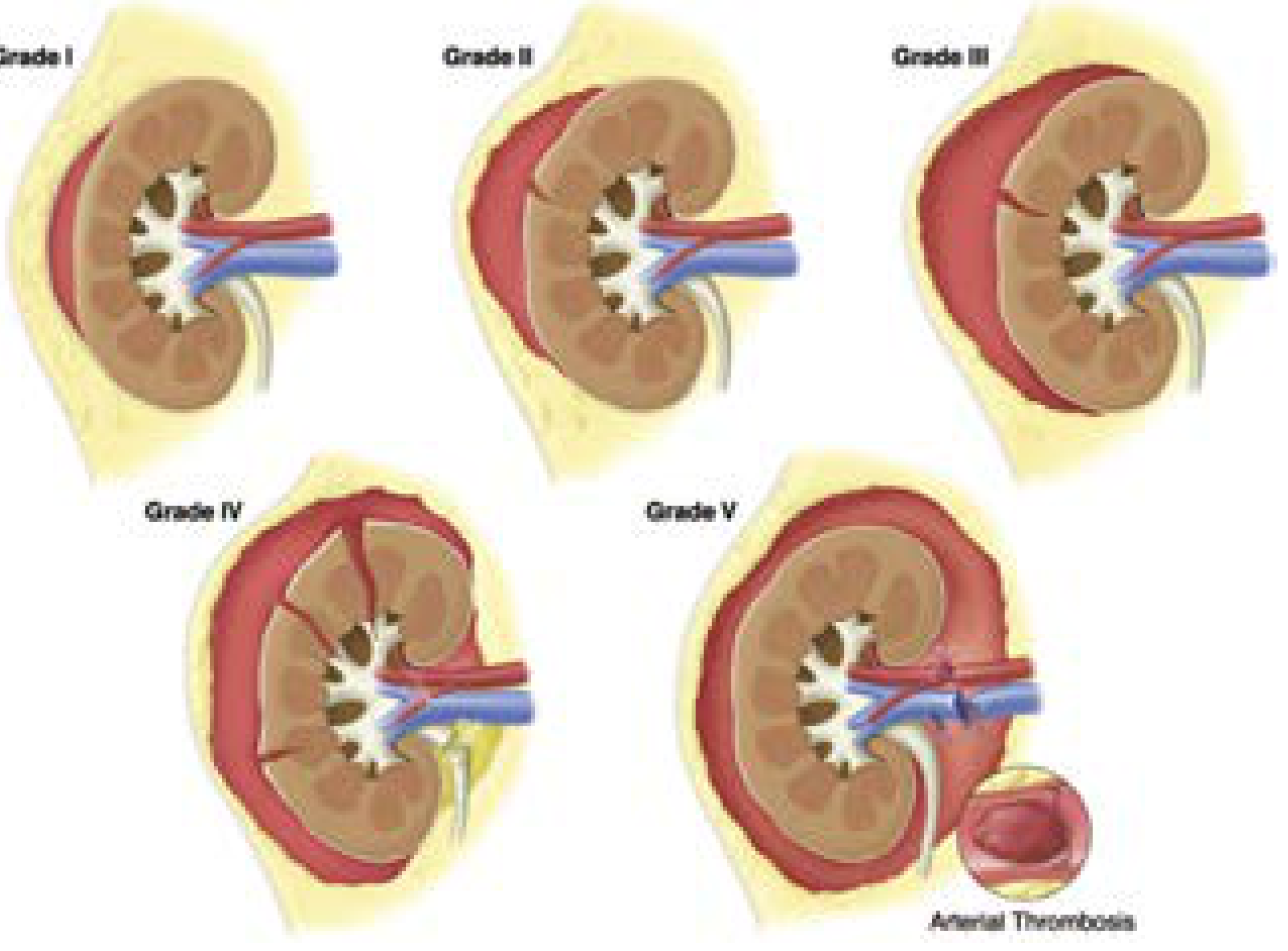
| Grade | Type | What it Means (CT lo emi kanapiStundi) | Hematoma Type | Management | WHY |
|---|---|---|---|---|---|
| I | Contusion / Hematoma | Subcapsular hematoma, no laceration. Micro/gross hematuria. Studies normal | Subcapsular, non-expanding, <10% surface | ✅ Conservative — bed rest, monitoring | Tamponade intact, no parenchymal tear, no collecting system injury |
| II | Hematoma + Laceration | Perirenal hematoma confined to Gerota's fascia. Lac <1 cm depth, NO urine leak | Perirenal, confined to Gerota fascia | ✅ Conservative | Gerota fascia = natural boundary. Tamponade contained. No duct injury |
| III | Laceration | Lac >1 cm depth, NO collecting system rupture, no urine leak | Expanding perinephric possible | ✅ Conservative (mostly) or angioembolization if vascular blush | Parenchyma injured but collecting system intact — no leak — tamponade possible |
| IV | Laceration + Vascular | Lac through cortex + medulla + collecting system → URINE LEAK. OR segmental renal A/V injury. OR active bleeding beyond Gerota | Perinephric expanding, beyond Gerota fascia | ⚠️ Conservative IF stable + closely monitor + stent urine leak. Angioembolization if blush. Operate if unstable | Collecting system breached = urinoma risk. Vascular injury = potential bleed. Gerota lost = tamponade lost |
| V | Shattered / Avulsion | Completely shattered kidney OR renal hilar avulsion (devascularized kidney) | Massive retroperitoneal hematoma | 🔴 Surgery — Nephrectomy | No salvageable parenchyma. Hilar avulsion = no perfusion = organ dead. Repair futile |
- Hemodynamic instability not responding to resuscitation
- Renal pedicle avulsion
- Pulsatile/expanding Zone 2 hematoma
- Penetrating trauma + retroperitoneal hematoma
🟤 ORGAN 2: LIVER — AAST Grading (OIS Scale)
| Grade | Type | Injury Description | Hematoma Character | Management | WHY |
|---|---|---|---|---|---|
| I | Hematoma + Laceration | Subcapsular hematoma <10% surface area. Capsular tear <1 cm depth | Subcapsular, non-expanding | ✅ Conservative — bed rest, serial CBC | Small, contained. Liver tamponade by capsule. Spontaneous hemostasis |
| II | Hematoma + Laceration | Subcapsular 10-50% surface. Intraparenchymal <10 cm. Lac 1-3 cm depth, <10 cm length | Subcapsular or intraparenchymal | ✅ Conservative — ICU monitoring | Capsule intact or minor breach. No major vessel involvement |
| III | Hematoma + Laceration | Subcapsular >50% surface or expanding. Ruptured subcapsular. Intraparenchymal >10 cm or expanding. Lac >3 cm depth | Expanding / ruptured subcapsular | ⚠️ Mostly conservative + angioembolization if blush. Operate if unstable | Expansion = active bleeding. Ruptured = loss of tamponade. Angioembo can control arterial source |
| IV | Laceration | Parenchymal disruption 25-75% hepatic lobe OR 1-3 Couinaud segments in one lobe | Major — crossing lobar planes | 🔴 Usually operative — packing, hepatorrhaphy, resection if needed | Major parenchyma destroyed. Significant vascular disruption. High bleed risk |
| V | Laceration + Vascular | >75% lobe disruption OR >3 Couinaud segments. Juxtahepatic / retrohepatic IVC injury | Massive | 🔴 Damage Control — pack + Pringle maneuver. Atrial caval shunt for retrohepatic IVC | Retrohepatic IVC = most lethal. Cannot repair under bleeding — pack first, stabilize, then repair |
| VI | Vascular | Hepatic avulsion | Exsanguinating | 🔴 Usually lethal — pack, damage control, ICU | Complete devascularization = not compatible with life in most cases |
- Pringle maneuver = portal triad (hepatic artery + portal vein) compression at hepatoduodenal ligament → controls inflow bleeding
- Atrial caval shunt = for retrohepatic IVC injury → bypass IVC bleeding
🟣 ORGAN 3: SPLEEN — AAST Grading
| Grade | Laceration | Hematoma | Management | WHY |
|---|---|---|---|---|
| I | <1 cm depth | Subcapsular <10% surface area | ✅ Conservative >95% success | Minor injury, capsule intact, natural tamponade |
| II | 1-3 cm, NOT involving trabecular vessel | Subcapsular 10-50% or intraparenchymal <5 cm | ✅ Conservative >90% success | No major vessels, contained hematoma |
| III | >3 cm OR involving trabecular vessel | Subcapsular >50% or RUPTURED subcapsular or intraparenchymal ≥5 cm | ⚠️ Conservative + consider angioembolization if CT blush | Large hematoma = risk of rupture. Trabecular vessel = more significant bleed |
| IV | Segmental or hilar vessel involvement | — | ⚠️ Angioembolization strongly considered. Operate if unstable | Hilar vessel injury = major hemorrhage potential |
| V | Shattered spleen or hilar vessel disruption with devascularization | — | 🔴 Splenectomy | No salvageable tissue. Devascularized = no viable organ. Cannot repair |
Post-splenectomy → OPSI (Overwhelming Post-Splenectomy Infection) — encapsulated organisms (Streptococcus pneumoniae, H. influenzae, Neisseria meningitidis) → vaccinate post-op!
🟡 ORGAN 4: PANCREAS — AAST Grading
| Grade | Injury | Duct Involved? | Management | WHY |
|---|---|---|---|---|
| I | Minor contusion/lac, no duct injury | ❌ No | Conservative — NPO, TPN, drain | No enzyme leak. Observation sufficient |
| II | Major contusion/lac, no duct injury | ❌ No | Conservative — NPO, TPN, closed-suction drain | No duct disruption = no ongoing enzyme leak |
| III | Distal transection OR parenchymal injury WITH duct injury | ✅ YES — distal | Distal pancreatectomy ± splenectomy | Duct disruption = caustic enzyme leak = fistula/abscess/pseudocyst. Remove distal segment |
| IV | Proximal transection / ampullary injury involving duct | ✅ YES — proximal (head) | Drainage procedure; Whipple in select cases | Head involvement = ampulla at risk. Complex repair |
| V | Massive disruption of pancreatic head | ✅ YES — massive | Damage control + complex reconstruction later | Pancreatic head = IVC, portal vein, bile duct close by — massive destruction |
Duct involved ≥ Grade III = OPERATE (distal = resect; proximal = complex) No duct = conservative
⚡ QUICK "GRADE ANSWER" TEMPLATE — 2-MINUTE FORMAT
"Sir, this is a Grade II renal injury — laceration less than 1 cm depth with perirenal hematoma confined within Gerota's fascia, no urinary extravasation. Since the mechanism is blunt and the patient is hemodynamically stable, this is managed conservatively with bed rest, IV fluids, serial hemoglobin monitoring, and repeat CT at 48-72 hours. No surgical intervention needed at this stage. We observe closely for any expanding hematoma, gross hematuria, or hemodynamic instability — any of which would prompt re-evaluation for intervention."
📊 MASTER GRADE SUMMARY — All Organs at a Glance
| Grade | Kidney | Liver | Spleen | Pancreas |
|---|---|---|---|---|
| I | Subcapsular hematoma, no lac | Subcapsular <10%, lac <1 cm | Subcapsular <10%, lac <1 cm | Contusion, no duct |
| II | Perirenal hematoma in Gerota, lac <1 cm | Subcapsular 10-50%, lac 1-3 cm | Subcapsular 10-50%, lac 1-3 cm, no trabecular | Major contusion, no duct |
| III | Lac >1 cm, NO collecting system | Subcapsular >50% / expanding / lac >3 cm | Lac >3 cm / trabecular vessel / ruptured subcapsular | Distal duct disruption |
| IV | Collecting system + urine leak OR segmental vessel | 25-75% lobe / 1-3 Couinaud segments | Hilar vessel involvement | Proximal duct / ampulla |
| V | Shattered / hilar avulsion | >75% lobe / retrohepatic IVC | Shattered / hilar devascularization | Massive head disruption |
| VI | N/A | Hepatic avulsion | N/A | N/A |
| Op? | Gr V = nephrectomy | Gr IV-V = pack+resect | Gr V = splenectomy | Gr III+ = resect/drain |
- Hematoma (subcapsular / perirenal / intraparenchymal) → Size + expanding? → Grade I-III
- Laceration depth → <1 cm = II, >1 cm = III, collecting system = IV, shattered = V
- Duct/vessel involvement → Yes = higher grade = operate
- Management key = Hemodynamic stability + grade combination decides! 💪🔥
How to manage a ptx with pelvic fracture and all inka neku telsinavi accutate ans oral exam lo cheppevi la vundali
🦴 PELVIC FRACTURE — COMPLETE ORAL EXAM GUIDE
(Accurate ga, step-by-step, tabular format — Tenglish lo)
🧠 ORAL EXAM LO ELA CHEPPALI — EXACT TEMPLATE
"Sir, this patient has a pelvic ring fracture with hemodynamic instability and a FAST-negative examination, which tells me the source of bleeding is the Zone 3 retroperitoneum — pelvic venous plexus and/or iliac vessel injury. My management follows a systematic multidisciplinary approach."
📍 STEP 1 — PELVIC FRACTURE CLASSIFICATION (Doctor definitely adugutadu!)
🅰️ TILE Classification (Stability based):
| Type | Stability | Pattern | Bleeding Risk | Management |
|---|---|---|---|---|
| A (A1, A2) | Stable | Avulsions, minimally displaced | Low | Non-operative |
| B (B1-B3) | Rotationally unstable, vertically STABLE | B1 = Open book; B2 = Lateral compression ipsilateral; B3 = Bucket handle | Moderate-High | Pelvic binder / ext fixation |
| C (C1-C3) | Rotationally AND vertically UNSTABLE | Complete SI joint disruption | HIGHEST — 67% present in shock | Surgery + angioembolization |
🅱️ Young & Burgess Classification (Mechanism based — most used!):
| Type | Mechanism | X-ray Finding | Bleeding Risk | WHY high risk? |
|---|---|---|---|---|
| LC I | Side impact — sacral fracture on impact side | Transverse sacral fracture | Low-moderate | Pelvis closes → reduces volume → less bleeding |
| LC II | Side impact — crescent fracture | Iliac wing fracture + SI disruption | Moderate | Some instability |
| LC III | LC I/II + contralateral open book | Ipsilateral LC + contralateral diastasis | HIGH — 60% retroperitoneal hematoma | Combined forces |
| APC I | Anterior compression — minor opening | Symphysis diastasis <2.5 cm | Low | Anterior only, posterior intact |
| APC II | Anterior compression — moderate | Symphysis >2.5 cm + anterior SI ligament torn | HIGH | Pelvic volume increases → more blood can accumulate |
| APC III | Anterior compression — complete | Complete SI joint disruption | HIGHEST — 67% shock | Complete pelvic ring disruption → massive volume increase → venous plexus + iliac vessels |
| VS | Vertical shear | Vertical hemipelvis displacement | HIGH — 63% hypovolemic shock | Hemipelvis completely unstable → tears all vessels |
"APC and VS injuries disrupt posterior SI ligaments — iki pelvic ring complete ga opens → pelvic volume dramatically increases → natural tamponade LOST → massive retroperitoneal hemorrhage possible"
📊 STEP 2 — ASSOCIATED INJURIES TABLE (Doc always adugutadu "what else?")
| Associated Injury | Incidence | How to Identify | Management |
|---|---|---|---|
| Urethral injury | 6-15% (males > females) | Blood at urethral meatus, inability to void, perineal hematoma, high-riding prostate on PR exam | DO NOT insert catheter! → Retrograde Urethrogram (RUG) first → Suprapubic cystostomy if injury confirmed |
| Bladder rupture — Extraperitoneal (EPBR) | ~60% of bladder injuries | Gross hematuria, inability to void, CT cystogram — extravasation around pelvis | Foley catheter drainage alone (3-4 weeks) — most heal spontaneously |
| Bladder rupture — Intraperitoneal (IPBR) | ~30% of bladder injuries | Hematuria + peritoneal signs, CT: intraperitoneal contrast leak | SURGICAL REPAIR — 2-layer closure. Foley + suprapubic drain |
| Rectal/bowel injury | ~14% | Blood on PR exam, rectal tenderness, CT — rectal perforation | Diverting colostomy + distal washout |
| Lumbosacral nerve injury | Common with VS/C type | Foot drop, perineal numbness, bladder/bowel dysfunction | Neurology consult; some recover with fracture fixation |
| Thoracic injuries | 63% | Chest X-ray, EFAST | Address simultaneously |
| Head injury | 40% (especially LC) | GCS, CT brain | TBI changes permissive hypotension strategy! |
| Aortic injury | APC injuries — 8× increased risk! | CT angio chest-abdomen | Endovascular stent graft |
🔴 STEP 3 — HEMORRHAGE MANAGEMENT ALGORITHM
The GOLDEN DECISION TREE:
PELVIC FRACTURE PATIENT
↓
HEMODYNAMICALLY STABLE?
/ \
YES NO
↓ ↓
CT scan (whole body) Apply PELVIC BINDER immediately
Identify source ↓
Plan fixation FAST positive?
/ \
YES NO
↓ ↓
Emergency Source = RETROPERITONEUM
Laparotomy (Zone 3 bleeding)
(intraperitoneal ↓
bleeding) RESUSCITATE (MTP 1:1:1)
↓
RESPOND to resuscitation?
/ \
YES NO
↓ ↓
CT angio PREPERITONEAL PACKING
(identify blush) + EXTERNAL FIXATION
↓ ↓
Arterial blush? Stabilized?
/ \ / \
YES NO YES NO
↓ ↓ ↓ ↓
Angio- Observe CT angio REBOA /
embolization + ICU + embolize Internal
iliac ligation
💊 STEP 4 — MANAGEMENT TABLE (All Interventions + WHY)
| Intervention | When | How | WHY |
|---|---|---|---|
| Pelvic Binder / Sheet | Immediately in ER — APC/VS type | Apply at greater trochanters level — closes pelvic ring | Reduces pelvic volume → restores retroperitoneal tamponade → compresses venous bleeding |
| Massive Transfusion Protocol (1:1:1) | All hemodynamically unstable | pRBC : FFP : Platelets 1:1:1 ratio | Reconstitutes whole blood, corrects TIC (Trauma-Induced Coagulopathy) |
| Tranexamic Acid | Within 3 hours of injury | 1g IV over 10 min → 1g over 8 hrs | Antifibrinolytic → preserves clot → reduces hemorrhage mortality (CRASH-2) |
| External Pelvic Fixation | Hemodynamically unstable, APC/VS | Anterior frame or C-clamp (posterior) | Reduces pelvic volume mechanically → tamponade restored → reduces venous bleeding |
| Preperitoneal Pelvic Packing (PPP) | Unstable not responding to binder/fixation | Pfannenstiel incision → pack preperitoneal space around pelvis | Directly compresses pelvic retroperitoneal bleeding — does NOT open Zone 3 hematoma |
| Angiography + Embolization | CT shows arterial blush OR fails to stabilize after packing | IR suite — selective coil/plug embolization of internal iliac branches | Arterial source (superior gluteal, pudendal arteries) — venous packing won't work for arterial — only embolization controls it |
| REBOA (Resuscitative Endovascular Balloon Occlusion of Aorta) | In extremis — massive ongoing hemorrhage | Zone 3 balloon at aortic bifurcation level | Temporizing — occludes aorta inflow → reduces pelvic bleeding → time to definitive control |
| Internal Iliac Ligation | Last resort — angioembolization failed/unavailable | Open surgical ligation of internal iliac artery | Reduces pulsatile flow to pelvis — collaterals maintain viability |
| Suprapubic Cystostomy | Urethral injury suspected | Percutaneous or open suprapubic tube | Bladder drainage WITHOUT going through damaged urethra |
| Retrograde Urethrogram (RUG) | Blood at meatus before any catheter | Inject contrast via meatus → X-ray | Confirms urethral integrity BEFORE placing Foley — placing Foley blindly converts partial to complete tear! |
⚠️ STEP 5 — CRITICAL "WHY" QUESTIONS TABLE
| Doctor's WHY question | Accurate answer |
|---|---|
| WHY pelvic binder at greater trochanter — not iliac crest? | Greater trochanter level closes POSTERIOR pelvic ring (SI joints) — iliac crest binder doesn't close the posterior ring → ineffective tamponade |
| WHY NOT open Zone 3 hematoma in blunt trauma? | Pelvic venous plexus bleeding — retroperitoneal space = natural tamponade. Opening releases it → uncontrolled exsanguination. Mortality approaches 100% if opened in blunt trauma |
| WHY PPP before angioembolization in some centers? | 80-85% of pelvic bleeding is VENOUS — packing controls venous. Angioembolization only controls arterial (15-20%). Packing faster to perform in unstable patient. Angioembo after stabilization |
| WHY REBOA Zone 3 (not Zone 1)? | Zone 3 balloon at aortic bifurcation — selectively reduces pelvic inflow without affecting visceral or renal vessels above. Zone 1 would occlude everything above |
| WHY do RUG before Foley in suspected urethral injury? | Partial urethral tear + blind Foley = converts partial → complete disruption. RUG first → if injury = suprapubic cystostomy instead |
| WHY EPBR managed conservatively (Foley only)? | Extraperitoneal bladder = urine stays in retroperitoneum → no peritoneal contamination → Foley diversion allows spontaneous healing. Surgery would disrupt pelvic hematoma tamponade |
| WHY IPBR needs surgery? | Intraperitoneal rupture → urine in peritoneum → chemical peritonitis → sepsis if not repaired urgently |
| WHY APC injuries bleed most? | APC opens the pelvic ring anteriorly AND tears posterior SI ligaments → massive volume increase → natural tamponade completely lost → venous plexus + arterial branches all torn |
| WHY mortality 38% in hypotensive pelvic fracture vs 3% in stable? | Hemodynamic instability = massive ongoing hemorrhage from venous plexus + arterial disruption. Large pelvic retroperitoneal space accommodates huge volumes before clinical deterioration noticed |
| WHY calcium in MTP? | Blood products contain citrate → chelates calcium → hypocalcemia → Factor IV deficiency → coagulation fails → more bleeding. CaCl₂ preferred over gluconate in trauma (needs no liver metabolism) |
🗣️ SAMPLE ORAL EXAM ANSWER — Full Marks Version
"Sir, this is an APC-type (open-book) pelvic ring fracture — likely Tile B1 or APC II/III — with hemodynamic instability and a FAST-negative examination.My immediate steps:First, ATLS primary survey — secure airway, establish 2 large-bore IVs, activate massive transfusion protocol at 1:1:1 ratio, give Tranexamic Acid 1g IV within 3 hours.Second, apply pelvic binder at the level of greater trochanters immediately — this closes the open pelvic ring, reduces volume, restores retroperitoneal tamponade.Since the FAST is negative, source of bleeding is Zone 3 retroperitoneum. I would NOT open this hematoma — opening a blunt Zone 3 hematoma releases the tamponade and causes uncontrolled exsanguination.If patient does not respond to resuscitation — I would proceed to preperitoneal packing plus external pelvic fixation, which directly compresses pelvic venous bleeding.Once patient stabilizes enough for imaging — CT abdomen and pelvis with IV contrast to identify arterial blush. If arterial blush present — angiography and selective embolization of internal iliac branches.Associated injuries to rule out: urethral injury — blood at meatus? Do retrograde urethrogram BEFORE placing catheter. Bladder rupture — CT cystogram. Rectal injury — PR exam. Nerve injury — neurological examination.Definitive pelvic fixation planned once physiologically stable — orthopaedics team for ORIF."
- Classification → Tile + Young-Burgess → APC/VS = worst bleeding
- FAST negative ≠ no bleeding → Zone 3 retroperitoneal
- Binder → PPP → Angio → step-up approach
- NEVER open Zone 3 blunt → death
- RUG before Foley → protect urethra
- Associated injuries list always mention 💪🔥
What will we order like tests in patients with blunt trauma
🧪 BLUNT TRAUMA — COMPLETE INVESTIGATIONS GUIDE
(Oral exam lo "what tests do you order?" adginapratisar — ee answer cheppu!)
🗣️ ORAL EXAM ANSWER OPENER
"Sir, my investigation approach depends on the patient's HEMODYNAMIC STATUS — stable vs unstable. I follow ATLS principles and order investigations in parallel with resuscitation, not instead of it."
⚡ THE MASTER DECISION FRAMEWORK
BLUNT TRAUMA PATIENT ARRIVES
↓
HEMODYNAMICALLY
STABLE?
/ \
YES NO
↓ ↓
Full workup BEDSIDE ONLY
(labs + CT) (FAST + CXR + Pelvis XR)
↓
Stabilizes? → CT
Doesn't? → OR directly
📋 INVESTIGATIONS TABLE — Complete + WHY for Each
🔴 BEDSIDE / IMMEDIATE (Done in Trauma Bay — All patients)
| Test | What It Shows | WHY Order It | Result + Interpretation |
|---|---|---|---|
| eFAST (Extended FAST) | Intraperitoneal free fluid, hemothorax, pneumothorax, pericardial effusion | Fastest bedside tool — no radiation, takes 2-3 min, done DURING resuscitation | Positive free fluid → emergency laparotomy if unstable. Negative → does NOT rule out retroperitoneal injury! |
| Chest X-ray (CXR) | Pneumothorax, hemothorax, rib fractures, diaphragm injury, mediastinal widening | Chest = #1 source of hidden bleeding after abdomen. Rib fractures over liver/spleen = suspect solid organ injury | Mediastinal widening → aortic injury → CT angio urgently |
| Pelvic X-ray (AP) | Pelvic ring fractures, symphysis diastasis | Pelvic fracture = Zone 3 retroperitoneal bleed source — FAST negative but patient unstable | Open-book fracture → apply binder IMMEDIATELY |
| 12-lead ECG | Cardiac contusion, arrhythmia, ST changes | Blunt chest trauma → myocardial contusion → arrhythmia risk in OR | ST changes / new RBBB → cardiac monitor, echo |
| Pulse oximetry + SpO₂ | Oxygen saturation continuously | Ongoing monitoring of respiratory status | <94% → supplemental O₂, consider intubation |
🟠 BLOOD TESTS (Send simultaneously — all blunt trauma)
| Test | What It Measures | WHY Order It | Critical Values + Meaning |
|---|---|---|---|
| Full Blood Count (FBC/CBC) | Hb, Hct, WBC, Platelets | Hb = blood loss estimate. Platelets = coagulopathy risk | Hb <8 g/dL → transfuse. Platelets <50,000 → give platelets in MTP |
| Blood Group + Cross-match | ABO/Rh type, compatible blood | Needed BEFORE transfusion. Takes 45-60 min | Emergency = O-negative blood (universal donor) until cross-match ready |
| Coagulation Profile (PT, aPTT, INR) | Clotting factor function | Trauma-induced coagulopathy (TIC) assessment — lethal triad component | INR >1.5 = coagulopathy → give FFP. aPTT >60 = factor deficiency |
| Fibrinogen | Fibrinogen level | First coagulation factor to deplete in massive hemorrhage | <1.5 g/L → give cryoprecipitate |
| Serum Lactate | Tissue hypoperfusion / anaerobic metabolism | Best marker of SHOCK severity and adequacy of resuscitation | >4 mmol/L = severe shock. Serial lactate — normalize with resuscitation |
| Base Excess (ABG) | Metabolic acidosis | pH + BE = lethal triad. Guides damage control decision | BE < -6 = significant acidosis. BE < -10 = consider damage control |
| Arterial Blood Gas (ABG) | pH, PaO₂, PaCO₂, HCO₃, Base Excess | Complete metabolic + respiratory picture — lethal triad diagnosis | pH <7.2 = damage control indication |
| Serum Electrolytes (Na, K, Ca, Mg) | Electrolyte status | Massive transfusion → hypocalcemia (citrate chelation), hypokalemia | Ionized Ca²⁺ <0.9 → give CaCl₂ immediately |
| Serum Amylase + Lipase | Pancreatic injury | Blunt epigastric trauma + seat belt sign → pancreatic injury | Amylase elevated >3 hrs post injury = significant. Early values can be NORMAL — don't rely on early result! |
| Liver Function Tests (LFTs) | AST, ALT, ALP, bilirubin | Hepatic injury screening. AST >200 = abdominal injury in pediatric trauma | Markedly elevated → CT abdomen |
| Urea + Creatinine (BMP) | Renal function baseline | Baseline before contrast CT. Oliguria post-trauma = renal injury or hypoperfusion | Elevated Cr → careful with contrast. Monitor urine output hourly |
| Urine dipstick / Urinalysis | Hematuria (microscopic or gross) | Renal / urological injury screening | Gross hematuria → CT urogram mandatory. Microscopic + hypotension → CT urogram |
| β-hCG (all women of childbearing age) | Pregnancy | Pregnant patient → radiation decisions, Rh management | Positive → obstetric consult, minimize radiation, Rh immunoglobulin if Rh-ve |
| Blood Alcohol Level | Intoxication | Blunt trauma often alcohol-related — affects clinical assessment | Elevated → GCS unreliable, CT brain important |
| Thromboelastography (TEG) / ROTEM | Real-time clot formation + fibrinolysis | Better than PT/aPTT for guiding MTP. Detects hyperfibrinolysis → guides TXA use | Hyperfibrinolysis pattern → Tranexamic Acid urgently |
🟡 IMAGING (Based on hemodynamic stability)
| Imaging Test | When to Order | What It Shows | WHY + Key Points |
|---|---|---|---|
| CT Abdomen + Pelvis with IV contrast | Hemodynamically STABLE patient | Solid organ injuries (grade), retroperitoneal hematoma zone, active arterial blush, free air, bowel injury | GOLD STANDARD for stable blunt trauma. 3D imaging — identifies zone, grade, vascular injury. WHY NOT in unstable? — CT delays definitive surgery → patient can die in scanner |
| CT Thorax with IV contrast | Suspected chest aortic injury (widened mediastinum on CXR) | Aortic injury, lung contusion, diaphragm tear | Mediastinal widening + blunt trauma = aortic injury until proven otherwise |
| CT Brain (non-contrast) | Any altered GCS, head injury, suspected TBI | Intracranial hemorrhage, skull fractures, cerebral edema | TBI changes management — no permissive hypotension in TBI (needs SBP >110 mmHg) |
| CT Urogram (contrast + delayed phase) | Gross hematuria OR microscopic hematuria + hypotension, deceleration injury | Renal lacerations (grade), urinary extravasation, urinoma, ureteral injury | Delayed phase (10-15 min) shows collecting system — essential for Grade IV renal injury |
| CT Angiography (CTA) | Arterial blush on regular CT, vascular injury suspected, pelvic fracture | Active arterial extravasation, pseudoaneurysm, vessel thrombosis | Identifies angioembolization target. Also therapeutic — can embolize in same session |
| Whole Body CT (Head to Pelvis) | Polytrauma, high-energy mechanism, deranged physiology | All injuries simultaneously — "pan-scan" | Most efficient in major trauma — misses fewer injuries than selective CT |
| Plain X-ray Cervical Spine | Neck pain, mechanism suggesting C-spine injury, altered GCS | Vertebral fractures, alignment | 3-view C-spine. Better replaced by CT C-spine in major trauma |
| EFAST (bedside ultrasound) | ALL unstable patients — immediately | Intraperitoneal fluid, pneumothorax, hemothorax, pericardial effusion | 4 windows: Hepatorenal (Morrison's), Splenorenal, Suprapubic, Pericardial + bilateral lung |
🟢 SPECIAL TESTS (Specific situations)
| Situation | Test | WHY |
|---|---|---|
| Seat belt sign + epigastric pain | Amylase (>3h), CT abdomen, MRCP/ERCP if CT unclear | Pancreatic injury — CT only 52-54% sensitive for duct. MRCP better for duct integrity |
| Pelvic fracture | CT pelvis, Retrograde Urethrogram (RUG) before Foley | Bladder/urethral injury in 6-15%. RUG before Foley = critical rule |
| Suspected aortic injury | CT Angiography Chest | High-energy deceleration = aortic shear at ligamentum arteriosum |
| Diaphragm injury suspected | CT chest/abdomen (both phases), diagnostic laparoscopy | Blunt diaphragm tears missed on plain X-ray — CT best |
| Suspected bowel/mesenteric injury | CT abdomen (look for free air, mesenteric stranding, bowel wall thickening) | No specific blood test. CT findings: free air = perforation, sentinel clot = mesenteric injury |
| TBI suspected | CT brain non-contrast | Intracranial hemorrhage — must rule out before permissive hypotension used |
📊 INVESTIGATIONS BASED ON HEMODYNAMIC STATUS — QUICK TABLE
| STABLE Patient | UNSTABLE Patient | |
|---|---|---|
| Primary | FAST + CXR + Pelvis XR simultaneously | FAST at bedside — takes 2-3 min |
| Blood tests | Full panel (all above) | Group + crossmatch + ABG + lactate STAT |
| Imaging | CT Whole Body (pan-scan) — gold standard | NO CT — go directly to OR |
| Special | CT urogram if hematuria, MRCP if pancreas suspected | Intraop assessment |
| Time | Can take 30-60 min for full workup | Every second counts — FAST → OR |
| Goal | Identify ALL injuries, grade them, plan management | Control bleeding FIRST — diagnose later |
⚡ ORAL EXAM "WHY" ANSWERS FOR INVESTIGATIONS
| Question | Answer |
|---|---|
| WHY CT not in unstable patient? | CT delays definitive hemorrhage control → patient can die in scanner. Unstable = straight to OR. "Treat the patient, not the scan" |
| WHY early amylase unreliable? | Pancreatic inflammation takes >3 hours to elevate amylase. Early = false negative. Always re-check at 3+ hours |
| WHY delayed CT urogram phase? | Contrast takes 10-15 min to reach collecting system. Without delay, urine extravasation (Grade IV renal) invisible |
| WHY eFAST not enough alone? | FAST = intraperitoneal only. Retroperitoneal, diaphragm, bowel, pancreatic injuries all missed. FAST negative ≠ no injury |
| WHY TEG/ROTEM better than PT/aPTT? | PT/aPTT measures only plasma coagulation — not platelets or fibrinolysis. TEG measures WHOLE BLOOD clot formation in real time — detects hyperfibrinolysis → guides TXA and cryoprecipitate use |
| WHY β-hCG in all women? | Pregnancy changes: (1) Minimize radiation, (2) Rh-ve mother needs anti-D if trauma, (3) Placental abruption risk, (4) Fetal monitoring needed |
| WHY serum lactate? | Lactate = marker of anaerobic metabolism = tissue hypoperfusion = shock. Serial lactate clearance = best resuscitation endpoint. Persistent high lactate = ongoing occult bleeding |
| WHY ionized calcium monitored in MTP? | pRBC + FFP contain citrate → chelates ionized calcium → hypocalcemia → coagulation fails (Ca²⁺ = Factor IV) + cardiac dysfunction → CaCl₂ must be given per 4 units blood products |
🗣️ COMPLETE ORAL ANSWER FORMAT
"Sir, in a blunt trauma patient, my investigations are guided by hemodynamic stability.Immediately, in ALL patients: eFAST exam to detect intraperitoneal blood, CXR for chest injuries, pelvic X-ray for pelvic fracture, and 12-lead ECG. Blood tests sent simultaneously: CBC, group and crossmatch, coagulation profile, ABG with lactate, serum electrolytes including ionized calcium, LFTs, amylase (after 3 hours post-injury), urea and creatinine, urinalysis for hematuria, and β-hCG in all women of childbearing age.If hemodynamically STABLE: CT whole body with IV contrast — gold standard. Includes CT brain, chest, abdomen-pelvis. If hematuria present: add delayed phase CT urogram. If pancreatic injury suspected: MRCP or serial amylase.If hemodynamically UNSTABLE: FAST only at bedside — if positive → emergency laparotomy immediately. No CT. The key principle is — treat the patient, not the scan."