Give me information about myocardial infaction so that I can understand very easily
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compose a complete, easy-to-understand guide on myocardial infarction.
Myocardial Infarction (Heart Attack) - A Complete Guide
What Is It? - The Simple Explanation
A myocardial infarction (MI), commonly called a "heart attack," is the death (necrosis) of heart muscle due to lack of blood supply. Think of it this way: your heart muscle needs oxygen to survive, just like you need air to breathe. When a blockage cuts off that blood supply, the muscle starts dying within 20-40 minutes of the obstruction.
- Robbins & Kumar Basic Pathology defines it as "necrosis of the heart muscle resulting from ischemia"
How Does It Happen? - The Mechanism
This diagram from Harrison's shows it beautifully:
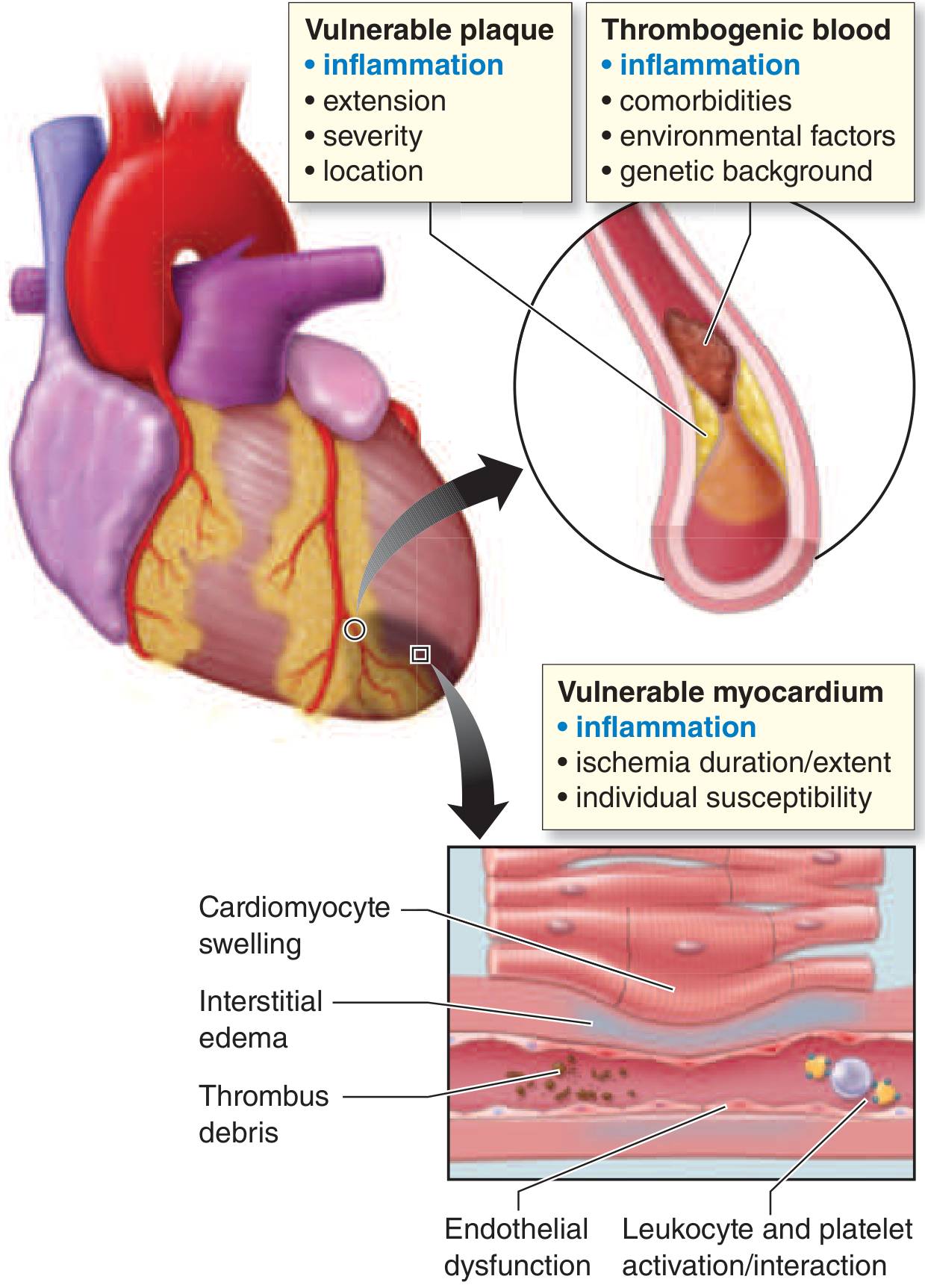
The process follows a clear sequence:
- Atherosclerosis builds up - A fatty plaque (atheroma) forms inside a coronary artery over years, narrowing it
- Plaque ruptures - The plaque's outer cap suddenly cracks due to mechanical stress or inflammation, exposing its inner contents to blood
- Clot forms instantly - Platelets rush to the rupture site and release thromboxane A2, ADP, and serotonin, triggering more clot formation. Tissue factor activates the coagulation cascade
- Artery blocks completely - Within minutes, the growing clot (thrombus) can fully occlude the coronary artery
- Muscle dies - Without oxygen, heart muscle cells die in a "wavefront" starting from the innermost layer (subendocardium) and spreading outward
Key fact: Angiography within 4 hours of an MI shows a clot in ~90% of cases. Without treatment, at least some clots dissolve spontaneously - but not fast enough to save the muscle. - Robbins & Kumar Basic Pathology
What Happens to the Heart Muscle?
Here is a microscopic view showing a normal coronary artery (left) versus one almost completely blocked by old thrombus (right):
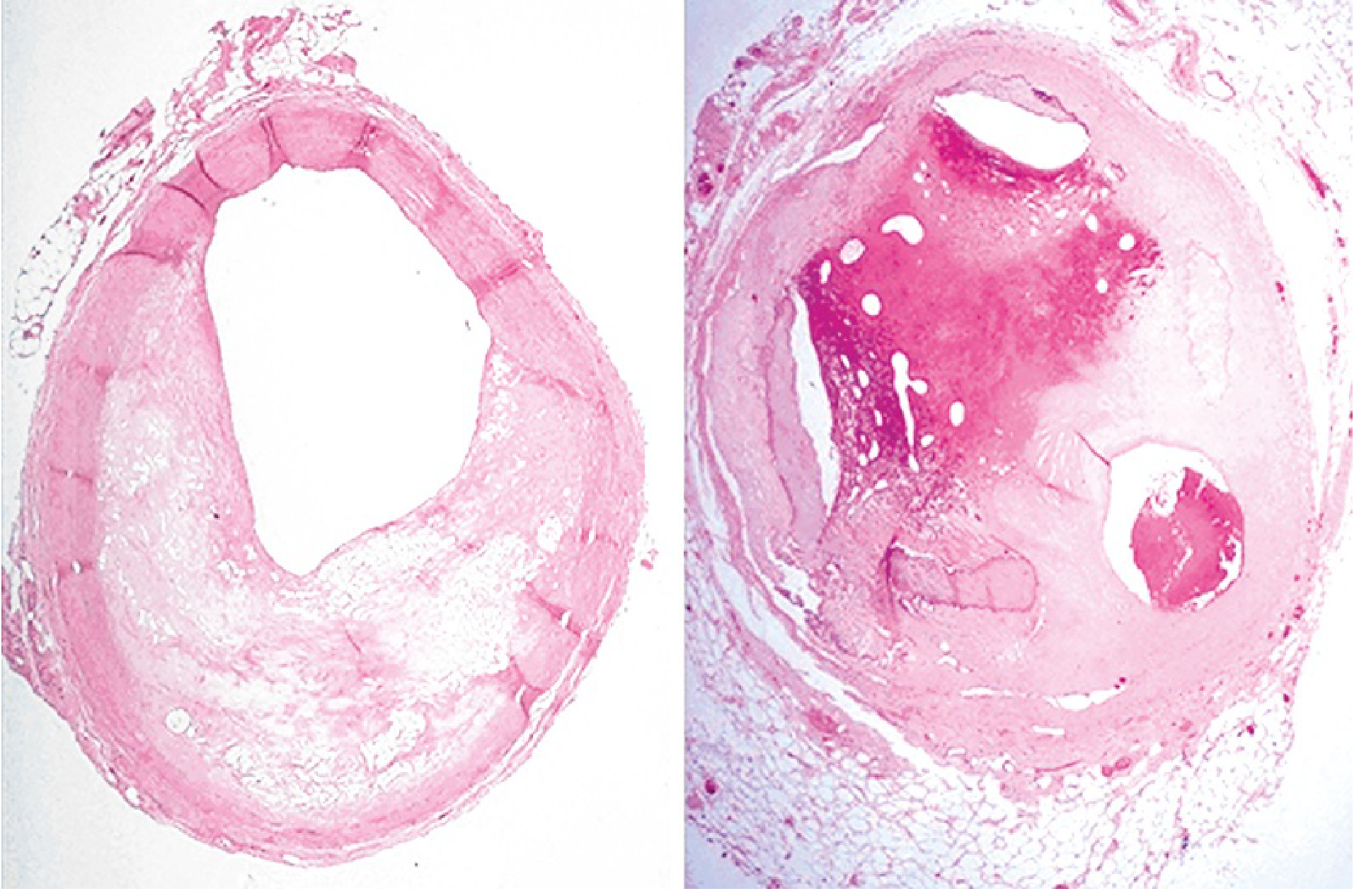
Within seconds of blockage, aerobic metabolism stops. ATP drops rapidly, lactic acid builds up, and the muscle cells lose their ability to contract. If blood flow is restored before 20-40 minutes, the damage can be reversed. After that, cells die irreversibly.
Why is the innermost layer (subendocardium) most vulnerable?
- It receives blood last, from the most distal branches
- It faces the highest internal pressures that squeeze blood vessels shut during contraction
- So any reduction in flow hits this zone hardest first - Guyton and Hall Textbook of Medical Physiology
Types of MI
| Type | Description |
|---|---|
| STEMI (ST-Elevation MI) | Full-thickness (transmural) blockage. The most severe type - ST segment rises on ECG. Requires emergency reperfusion. |
| NSTEMI (Non-ST-Elevation MI) | Partial blockage. ST segment does not elevate. Still serious but slightly less acute. |
| Subendocardial MI | Only the innermost layer is affected. Can occur even without total occlusion - e.g., during prolonged high demand (tachycardia, severe hypertension) on top of existing coronary narrowing. |
Risk Factors
- Age - Frequency rises sharply with age; ~45% of MIs happen before age 65
- Male sex - Men at higher risk, but gap narrows after menopause in women
- Atherosclerosis risk factors - High cholesterol, hypertension, diabetes, smoking, obesity
- Family history
- Prior heart disease
Note: ~10% of MIs occur before age 40. Women after menopause lose their estrogen-related protection and IHD becomes the #1 cause of death in older women. - Robbins & Kumar Basic Pathology
Symptoms - What Does It Feel Like?
Classic presentation:
- Chest pain - Heavy, crushing, pressure-like discomfort in the center of the chest, lasting more than 30 minutes
- Radiation - Pain spreads to the left arm, jaw, neck, or back
- Sweating (diaphoresis) - Often described as cold, clammy sweat
- Shortness of breath
- Nausea and vomiting
- Anxiety - Patients are often restless and unable to get comfortable
The combination of >30 minutes of substernal chest pain + profuse sweating strongly suggests STEMI. - Harrison's Principles of Internal Medicine
Important atypical presentations (especially in diabetics and the elderly):
- No chest pain at all ("silent MI")
- Sudden breathlessness
- Sudden loss of consciousness
- Profound weakness or fatigue
- Confusion
Physical signs doctors look for:
- Pallor, cold extremities (reduced cardiac output)
- Tachycardia (fast heart rate) in anterior MI (sympathetic activation)
- Bradycardia (slow heart rate) in inferior MI (vagal activation)
- 3rd and 4th heart sounds (sign of poor ventricular function)
- Possible pericardial friction rub
- Fever up to 38°C in the first week
Diagnosis - How It Is Confirmed
1. ECG (Electrocardiogram)
The most important and fastest tool - should be done within 10 minutes of hospital arrival.
- STEMI: ST elevation in the leads corresponding to the affected territory
- NSTEMI: ST depression, T-wave changes
- Old MI: Pathological Q waves (deep, wide Q waves in two contiguous leads)
2. Cardiac Biomarkers (Blood Tests)
The most important marker is Troponin (cTnI or cTnT):
- Leaks out of dying cells when the sarcolemmal membrane ruptures
- Rises within 3-6 hours of onset, peaks at 12-24 hours, stays elevated for days
- The higher the troponin rise, the larger the infarct
Initial troponin may be normal if the patient presents very early - serial measurements are needed. - Washington Manual of Medical Therapeutics
3. Imaging
- Chest X-ray - Looks for pulmonary edema and rules out aortic dissection
- Echocardiogram (ultrasound) - Shows wall motion abnormalities (areas of muscle not contracting) - useful when diagnosis is uncertain
- Coronary angiography - The gold standard - directly visualizes the blockage before angioplasty
Causes of Death After MI
The four main causes are (from Guyton & Hall):
- Decreased cardiac output (cardiogenic shock) - The damaged heart cannot pump enough blood. Importantly, the infarcted area can bulge outward during contraction ("systolic stretch"), making the pump even less efficient than the size of the infarct suggests
- Pulmonary edema - Blood dams up behind the failing left ventricle, flooding the lungs
- Ventricular fibrillation - The most common cause of death: ischemic muscle becomes electrically unstable. In 80-90% of cardiac deaths from ischemia, ventricular fibrillation is the final mechanism
- Cardiac rupture - The infarcted muscle softens and tears (typically days 3-7 after MI)
Treatment - The Golden Hour
"Time is muscle" - Every minute of delay means more heart muscle dies. Mortality benefit from reperfusion drops sharply with time.
Immediate Goals
- Restore blood flow (reperfusion) as fast as possible
- Relieve pain
- Prevent complications (arrhythmias, shock, pulmonary edema)
Step-by-Step Management
Pre-hospital / On arrival:
- Aspirin 162-325 mg (chewed, not swallowed whole) - immediately blocks platelet aggregation
- 12-lead ECG within 10 minutes of arrival
- Oxygen if O2 saturation < 90%
- IV access, cardiac monitoring, defibrillator ready
Reperfusion therapy (the cornerstone):
| Method | Details |
|---|---|
| Primary PCI (Percutaneous Coronary Intervention) | Preferred if available within 90 min of first medical contact. A catheter is threaded to the blocked artery; a balloon opens it and a stent keeps it open. |
| Thrombolytics (clot-busting drugs) | Used if PCI cannot be done within time limits. Drugs like alteplase or tenecteplase dissolve the clot. Patient is then transferred to a PCI center. |
Medications used (from Washington Manual):
| Drug | Role |
|---|---|
| Aspirin | Antiplatelet - blocks thromboxane A2 |
| P2Y12 inhibitors (Ticagrelor, Prasugrel, Clopidogrel) | Stronger antiplatelet - blocks ADP pathway |
| Heparin (UFH) or low-molecular-weight heparin | Anticoagulant - prevents clot extension |
| Beta-blockers (metoprolol) | Reduce heart rate and oxygen demand, prevent arrhythmias |
| ACE inhibitors / ARBs | Reduce remodeling and heart failure risk |
| Statins (high-intensity) | Stabilize plaques, lower LDL |
| Nitroglycerin | Relieves ischemic pain (avoid if hypotensive) |
| Morphine | Pain relief (use cautiously - may reduce platelet drug absorption) |
Complications
| Complication | When | Mechanism |
|---|---|---|
| Arrhythmias | Within hours | Electrical instability of ischemic muscle |
| Heart failure / Cardiogenic shock | Hours-days | Large area of muscle lost |
| Ventricular septal rupture | Days 3-7 | Softened septum perforates |
| Papillary muscle rupture | Days 3-7 | Mitral regurgitation |
| Free wall rupture | Days 3-7 | Cardiac tamponade - often fatal |
| Pericarditis (Dressler's syndrome) | Weeks-months | Autoimmune reaction |
| Left ventricular aneurysm | Weeks | Thin, scarred wall bulges out |
Recovery and Long-Term Care
The heart heals in three stages:
- Acute (hours to 7 days) - Necrosis, neutrophil infiltration
- Healing (7-28 days) - Macrophages clear debris, granulation tissue forms
- Healed (after 29 days) - Scar tissue replaces dead muscle (permanent, non-contractile)
Long-term medications typically continued: dual antiplatelet therapy (for at least 1 year after stent), statin, beta-blocker, ACE inhibitor, and lifestyle modification (diet, exercise, smoking cessation).
Quick Summary
Blocked coronary artery
↓
No oxygen to heart muscle
↓
Cells die after 20-40 min (starting from inner layer)
↓
Symptoms: chest pain, sweating, breathlessness
↓
Diagnosis: ECG + Troponin
↓
Treatment: Open the artery ASAP (PCI or thrombolytics)
+ Aspirin + anticoagulant + beta-blocker + statin
Sources: Robbins & Kumar Basic Pathology | Guyton and Hall Textbook of Medical Physiology | Harrison's Principles of Internal Medicine 22E | Washington Manual of Medical Therapeutics | Fuster and Hurst's The Heart, 15th Edition
This is a shared conversation. Sign in to Orris to start your own chat.