Copd with xray
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Finding Sources
Excellent - I have everything I need. Here is a complete, well-illustrated answer on COPD chest X-ray findings.
COPD - Chest X-Ray Findings
Why CXR Matters in COPD
Chest radiography is not required to diagnose COPD (spirometry is the gold standard), but it is frequently obtained to investigate dyspnea, hemoptysis, or to exclude complicating conditions like pneumonia, heart failure, lung cancer, or pneumothorax. It is not particularly sensitive or specific for COPD diagnosis, but certain findings are characteristic.
Classic CXR Findings
1. Hyperinflation (Most Important Finding)
| Feature | Description |
|---|---|
| Flattened diaphragms | Bilateral diaphragmatic flattening - the most reliable sign. Best seen on the lateral view. |
| Increased lung volumes | Lungs appear unusually large; > 6 anterior ribs visible above the diaphragm on PA view |
| Barrel chest appearance | Increased AP diameter; AP:lateral ratio approaches 1:1 |
| Prominent retrosternal clear space | Clearly seen on lateral view - air trapping pushes the heart posteriorly |
| Low, flat diaphragms | On lateral view, diaphragm may appear nearly horizontal |
2. Lung Lucency
- Diffuse hyperlucency - reduced vascular markings throughout lungs
- Upper lobe predominance in centriacinar (centrilobular) emphysema (typical of smoking)
- Lower lobe predominance in panacinar emphysema (associated with alpha-1 antitrypsin deficiency)
- Bullae - focal radiolucent areas with thin walls; may be very large ("vanishing lung")
3. Vascular Changes
- Peripheral vascular pruning - vessels become attenuated and sparse at the periphery
- Prominent central pulmonary arteries - may indicate pulmonary hypertension (cor pulmonale)
4. Cardiac Changes
- Small, narrow, vertical heart - due to hyperinflated lungs pushing the heart into a more vertical position on frontal view
- In advanced disease with cor pulmonale: right ventricular enlargement
5. Airway Changes (often subtle on plain film)
- Bronchial wall thickening ("tram-tracks") - more obvious on CT
- Dirty chest appearance - increased bronhovascular markings in chronic bronchitis phenotype
Actual CXR from Murray & Nadel's Respiratory Medicine
Figure 64.3 - Centriacinar emphysema (54-year-old female smoker):
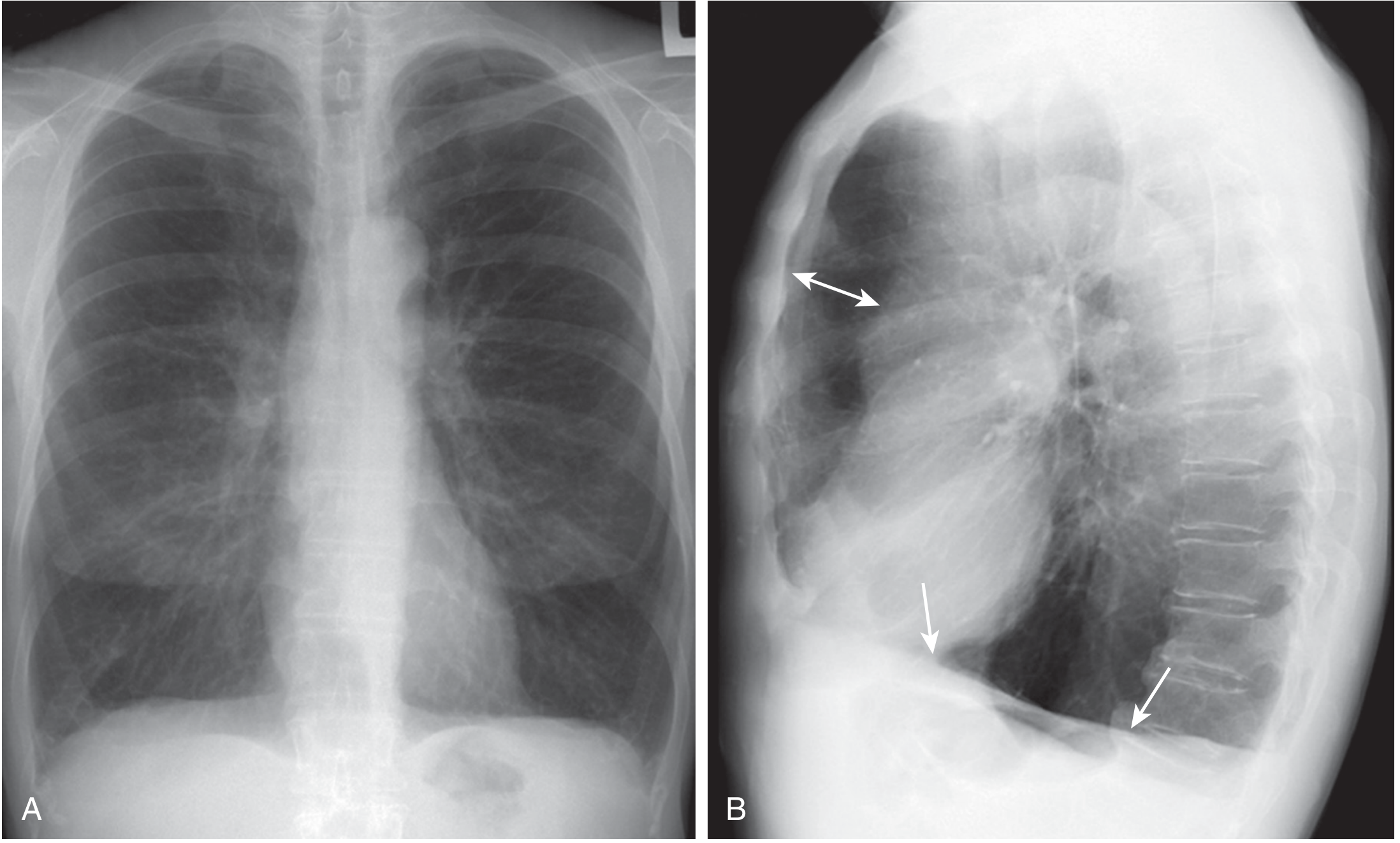
What to see in this image:
- (A) PA (frontal) view: Very large lung volumes; hyperlucency predominant in upper lobes; small-appearing, narrow heart
- (B) Lateral view: Arrows point to flattened diaphragms; double arrow shows a prominent retrosternal clear space - this is pathognomonic of severe hyperinflation
CT Chest in COPD - Two Phenotypes
CT is more sensitive than plain film and allows quantification of emphysema:
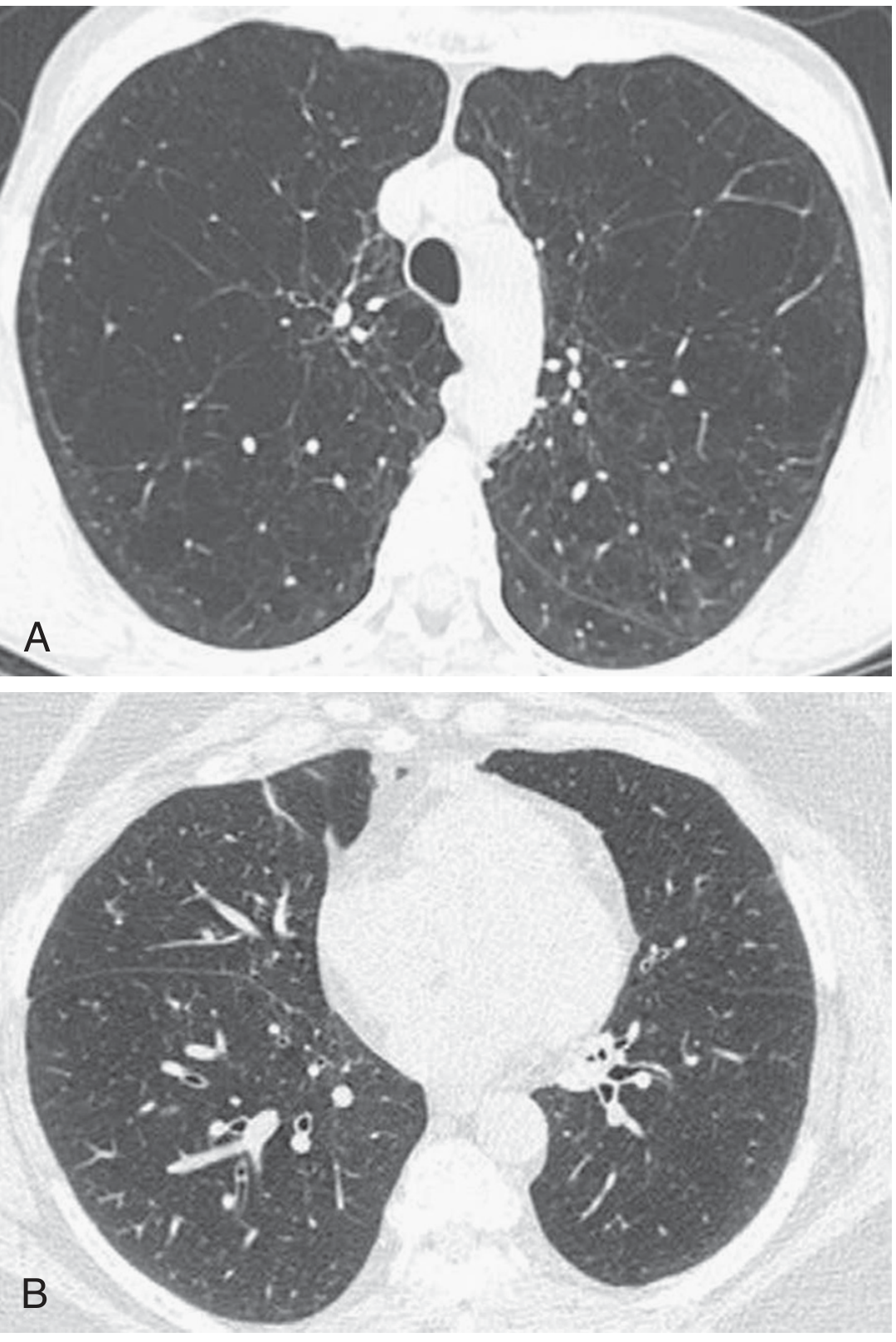
- (A) Emphysema-predominant phenotype: Extensive low-attenuation areas (black areas) = destroyed alveolar tissue; sparse vascular markings
- (B) Airway-predominant phenotype: Less emphysema; bronchial wall thickening is more prominent; patchier distribution
CT findings include:
- Low-attenuation areas (LAA) - marker of emphysema, threshold typically -950 HU
- Air trapping on expiratory views = small airway obstruction
- Bronchial wall thickening - ratio of wall thickness to outer diameter >0.5 is abnormal
- Bronchiectasis - associated with increased mortality in COPD
Radiological Pattern by COPD Subtype
| Feature | Centriacinar (Centrilobular) | Panacinar |
|---|---|---|
| Cause | Cigarette smoking | Alpha-1 antitrypsin deficiency |
| Distribution | Upper lobe predominant | Lower lobe predominant |
| Severity | Often asymmetric | Often diffuse |
Limitations of Plain CXR
- Only ~50% sensitive for mild-to-moderate emphysema
- Normal CXR does not rule out COPD
- CT is needed for: surgical planning (lung volume reduction surgery), lung transplant evaluation, screening for lung cancer, evaluation of bronchiectasis or ILD
Quick Summary - "COPD on CXR" Checklist
- Hyperinflated lungs (>6 anterior ribs above R. hemidiaphragm)
- Flat diaphragms (PA and lateral)
- Prominent retrosternal space (lateral)
- Hyperlucency / bullae
- Peripheral vascular pruning
- Small, vertical heart
- Possible central pulmonary artery enlargement (cor pulmonale)
Source: Murray & Nadel's Textbook of Respiratory Medicine, Fig. 64.3-64.4, pp. 1472-1473
This is a shared conversation. Sign in to Orris to start your own chat.