Management of hypertention conceptually
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hypertension"[MeSH Terms] AND "antihypertensive agents"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Excellent content gathered. Now I have everything needed for a thorough conceptual overview. Let me compose the comprehensive answer.
Management of Hypertension - Conceptual Overview
Sources: Lippincott Illustrated Reviews: Pharmacology, Harrison's Principles of Internal Medicine 22E (2025), Braunwald's Heart Disease, Comprehensive Clinical Nephrology 7e
1. What Is the Goal?
The overarching goal of antihypertensive therapy is to reduce cardiovascular and renal morbidity and mortality - not just to lower a number. This means preventing stroke, MI, heart failure, and CKD progression.
Blood pressure targets (ACC/AHA 2017 - most widely adopted):
- General population: < 130/80 mmHg
- CKD patients (KDIGO 2020): SBP < 120 mmHg
- Elderly >80 years (NICE): < 150/90 mmHg
- Diabetes (ADA): < 140/90, or < 130/80 in high ASCVD risk
2. Non-Pharmacologic (Lifestyle) Interventions - First Line
Before or alongside any drug, lifestyle changes can meaningfully reduce BP and may be the only treatment needed in mild hypertension:
| Intervention | Expected BP Reduction |
|---|---|
| Aerobic exercise (30 min, 5 days/week) | 4-9 mmHg |
| Sodium restriction (< 2.4 g/day) | 2-8 mmHg |
| DASH diet | 8-14 mmHg |
| Weight loss (per 10 kg lost) | 5-20 mmHg |
| Alcohol restriction | 2-4 mmHg |
| Smoking cessation | Reduces CV risk overall |
These are especially important in older adults to minimize polypharmacy.
- Braunwald's Heart Disease, p. 2945
3. When to Start Drugs and How Many?
- Stage 1 hypertension (130-139/80-89): lifestyle first; add drug if cardiovascular risk is high or lifestyle fails after 3 months.
- Stage 2 hypertension (≥140/90): start drug therapy alongside lifestyle.
- If SBP > 20 mmHg above goal or DBP > 10 mmHg above goal: start with two drugs simultaneously rather than monotherapy.
- Approximately two-thirds of patients with hypertension will require two or more drugs to reach target BP.
Combination therapy allows lower doses of each agent, reduces dose-dependent side effects, and achieves additive organ protection.
- Lippincott Illustrated Reviews: Pharmacology, p. 294
4. The Four First-Line Drug Classes
Current guidelines (ACC/AHA, ESH/ESC) recommend four major classes as initial therapy:
A. Thiazide Diuretics
Prototype: Hydrochlorothiazide, Chlorthalidone
- Mechanism: Initially reduce intravascular volume via Na+/water excretion; long-term effect is decreased peripheral vascular resistance.
- Key advantage: Inexpensive, proven mortality reduction.
- Avoid if: eGFR < 30 mL/min (use loop diuretics instead; metolazone is an exception).
- Adverse effects: Hypokalemia, hyperuricemia, hyperglycemia.
B. ACE Inhibitors (ACEi)
Prototype: Enalapril, Lisinopril, Ramipril
- Mechanism: Block conversion of angiotensin I to angiotensin II → decrease vasoconstriction and aldosterone release → lower BP + reduce cardiac/renal afterload.
- Special benefit: Slow CKD progression (beyond BP lowering - reduce intraglomerular hyperfiltration), reduce albuminuria, improve outcomes post-MI and in heart failure with reduced EF.
- Key adverse effects: Dry cough (up to 10% - due to bradykinin accumulation), angioedema (rare but serious), hyperkalemia, teratogenicity (absolutely contraindicated in pregnancy).
- A rise in serum creatinine of up to 30% after starting ACEi is acceptable and does not require stopping the drug.
C. Angiotensin Receptor Blockers (ARBs)
Prototype: Losartan, Valsartan, Irbesartan
- Mechanism: Block AT1 receptors directly → similar hemodynamic effects to ACEi, but do NOT increase bradykinin - so no cough.
- Use: All indications of ACEi, preferred when ACEi is not tolerated (cough). Do NOT combine ACEi + ARB (no added benefit, increased harm).
D. Calcium Channel Blockers (CCBs)
Prototype: Amlodipine (dihydropyridine), Diltiazem/Verapamil (non-dihydropyridine)
-
Mechanism: Block L-type Ca2+ channels in vascular smooth muscle and (for non-DHP) myocardium → vasodilation and reduced cardiac output.
-
Dihydropyridines (amlodipine): Primarily vascular - preferred in hypertension; used in Black patients, elderly, stable angina.
-
Non-dihydropyridines (diltiazem, verapamil): Also slow AV conduction - useful in AF with hypertension; avoid in HFrEF.
-
Lippincott Illustrated Reviews: Pharmacology, p. 296-305
5. Drug Selection by Comorbidity (Compelling Indications)
This is the conceptual heart of hypertension management - matching the drug class to the patient's comorbidities:
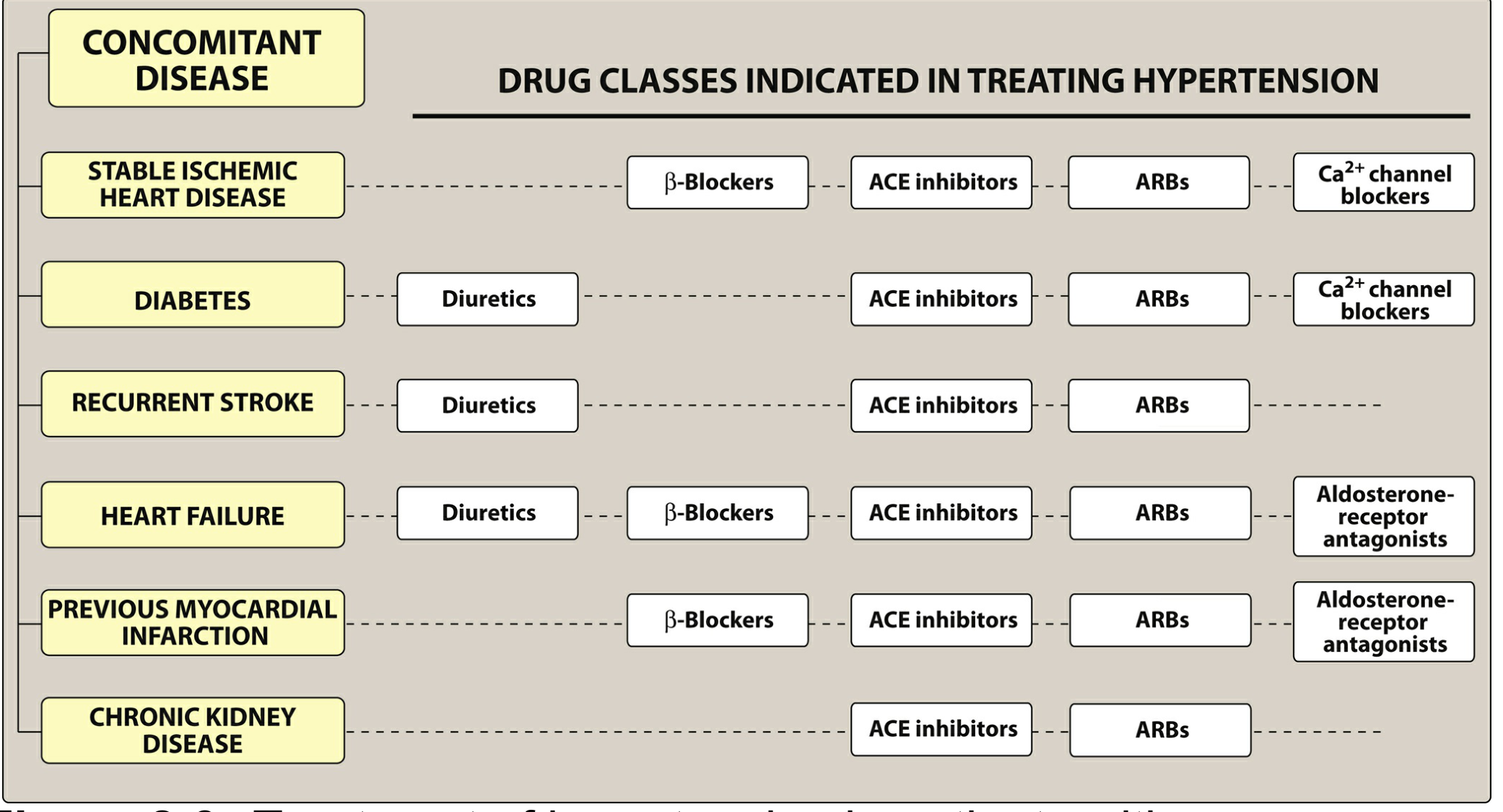
| Comorbidity | Preferred Drug Classes |
|---|---|
| Stable ischemic heart disease | Beta-blockers, ACEi, ARBs, CCBs |
| Heart failure (HFrEF) | Diuretics, Beta-blockers, ACEi/ARBs, Aldosterone antagonists |
| Post-MI | Beta-blockers, ACEi/ARBs, Aldosterone antagonists |
| Diabetes | Diuretics, ACEi, ARBs, CCBs |
| CKD (with/without proteinuria) | ACEi or ARB (first-line - renoprotective) |
| Recurrent stroke prevention | Diuretics, ACEi, ARBs |
| Black patients | Thiazide diuretics or CCBs (ACEi/ARBs less effective as monotherapy) |
| Pregnancy | Methyldopa, labetalol, nifedipine (ACEi/ARBs contraindicated) |
6. Step-Up Approach (Sequential Intensification)
Step 1: Lifestyle modification alone (mild HTN)
↓ (if not at goal in 3 months)
Step 2: Single first-line drug (thiazide OR ACEi/ARB OR CCB)
↓ (if not at goal)
Step 3: Add a second drug from a different class
Preferred combos: ACEi/ARB + CCB, or ACEi/ARB + Thiazide
↓ (if not at goal on two drugs at optimal doses)
Step 4: Add a third drug (triple therapy)
↓ (if still not at goal on 3 drugs including a diuretic)
Step 5: Resistant hypertension workup + add-on agents
(spironolactone, alpha-blockers, beta-blockers, direct vasodilators)
Preferred combination pairs (ESH/ESC 2018):
- ACEi/ARB + CCB (best tolerated, cardioprotective)
- ACEi/ARB + thiazide diuretic
- CCB + thiazide diuretic
Avoid: ACEi + ARB together (dual RAS blockade - hyperkalemia risk, no added CV benefit).
7. Resistant Hypertension
Defined as BP above target despite optimal doses of three antihypertensives including a diuretic. Causes to rule out first:
- Poor adherence ("pseudoresistance")
- White-coat hypertension
- Secondary causes (primary aldosteronism, renal artery stenosis, OSA, pheochromocytoma, Cushing's)
- Drug interactions (NSAIDs, sympathomimetics, oral contraceptives, licorice)
Add-on treatment: Spironolactone (most evidence for resistant HTN), alpha-blockers (doxazosin), beta-blockers, or direct vasodilators (hydralazine, minoxidil - last resort).
Refractory hypertension = uncontrolled on five or more agents at maximal doses.
- Fuster and Hurst's The Heart, 15th Edition
8. Special Populations
CKD
- ACEi/ARB are first-line - they reduce intraglomerular pressure beyond their systemic BP effect.
- SGLT2 inhibitors (gliflozins) are now gaining a role in cardiorenal protection.
- A modest GFR dip (<30% of baseline) after starting ACEi/ARB is acceptable - it may reflect reduced hyperfiltration.
- Avoid ACEi + ARB combination; monitor potassium carefully.
- Harrison's Principles of Internal Medicine 22E, p. 295-299
Elderly
- Start low, go slow - age-related changes in drug metabolism.
- Check both seated and standing BP (orthostatic hypotension risk).
- Two or more drugs commonly needed.
Pregnancy
- ACEi and ARBs are absolutely contraindicated (fetal renal malformations).
- Safe options: Methyldopa, labetalol, nifedipine.
9. Key Conceptual Principles (Summary)
- Treat the patient, not just the number - comorbidities dictate drug choice.
- Most patients need 2+ drugs - combination therapy is the rule, not the exception.
- RAS blockade (ACEi/ARB) is cornerstone in CKD, heart failure, diabetes, and post-MI.
- CCBs and thiazides are especially effective in Black patients and the elderly.
- Non-pharmacologic measures are always part of management - never optional.
- Avoid dual RAS blockade (ACEi + ARB) - same class should not be combined.
- Resistant hypertension requires secondary cause workup before escalating drugs.
Recent evidence note: A 2025 Lancet systematic review (PMID 40885583) confirmed the BP-lowering efficacy of all four first-line drug classes and their combinations in randomized controlled trials, supporting current guidelines. No major paradigm shifts from guideline recommendations were identified.
This is a shared conversation. Sign in to Orris to start your own chat.