Ecg changes with images top 10
Reading File
Finding Sources
Searching Images
ECG changes electrocardiogram patterns STEMI ST elevation myocardial infarction
Finding Sources
Searching Images
ECG hyperkalemia peaked T waves QRS widening sine wave pattern
Searching Images
atrial fibrillation ECG irregularly irregular no P waves
Searching Images
Wolff-Parkinson-White syndrome ECG delta wave short PR interval
Searching Images
complete heart block third degree AV block ECG P waves dissociation
Searching Images
pericarditis ECG saddle shaped ST elevation PR depression diffuse
Searching Images
left bundle branch block LBBB ECG broad QRS notched R wave
Searching Images
Brugada syndrome ECG coved ST elevation V1 V2 right bundle branch pattern
Searching Images
long QT syndrome torsades de pointes ECG twisting QRS axis polymorphic VT
Searching Images
pulmonary embolism ECG S1Q3T3 right heart strain sinus tachycardia
I now have excellent images for all 10 ECG patterns. Let me compile the comprehensive answer.
Top 10 ECG Changes — With Images
1. 🫀 STEMI — ST-Elevation Myocardial Infarction
Key ECG Features:
- Convex ("tombstone") ST elevation ≥1 mm in ≥2 contiguous limb leads or ≥2 mm in precordial leads
- Reciprocal ST depression in opposing leads
- Hyperacute T waves (earliest sign)
- Q waves (evolve over hours — sign of necrosis)
- T-wave inversion (late sign)
Territories:
| Territory | ST Elevation | Reciprocal Changes | Culprit Vessel |
|---|---|---|---|
| Inferior | II, III, aVF | aVL, I | RCA or LCx |
| Anterior | V1–V4 | II, III, aVF | LAD |
| Anterolateral | V1–V6, I, aVL | II, III, aVF | LAD (proximal) |
| Lateral | I, aVL, V5–V6 | aVF | LCx diagonal |
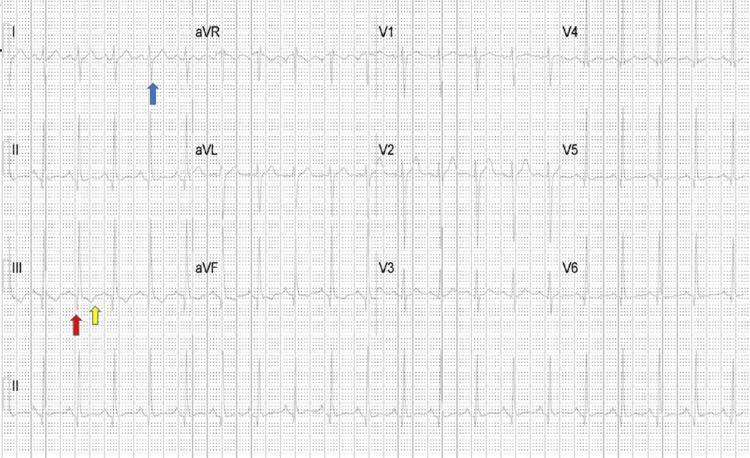
Inferior STEMI (Tombstone Pattern)
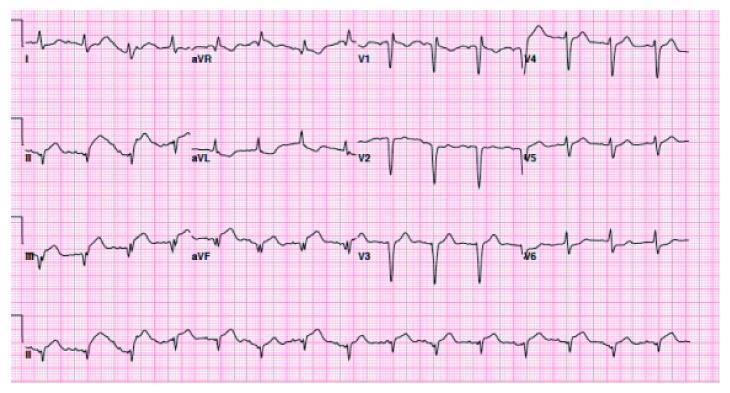
Anterolateral STEMI
Inferolateral STEMI with annotated leads
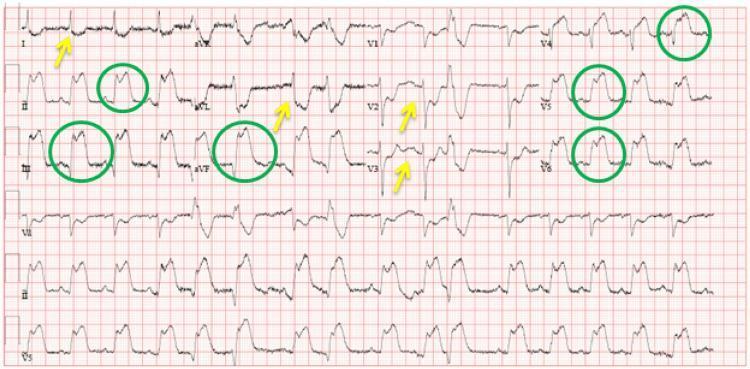
2. 🔥 Pericarditis
Key ECG Features (4 stages):
- Stage 1 (acute): Diffuse concave ("saddle-shaped") ST elevation in nearly all leads; PR depression (most specific) in II, V4–V6; PR elevation in aVR
- Stage 2: ST normalises, T-wave flattening
- Stage 3: T-wave inversion
- Stage 4: Normalisation
Distinguishing from STEMI: ST elevation is diffuse (not territory-limited), concave (not convex), PR depression is present, no reciprocal ST depression (except aVR).
Spodick's sign: Downsloping TP segment in multiple leads — highly specific.

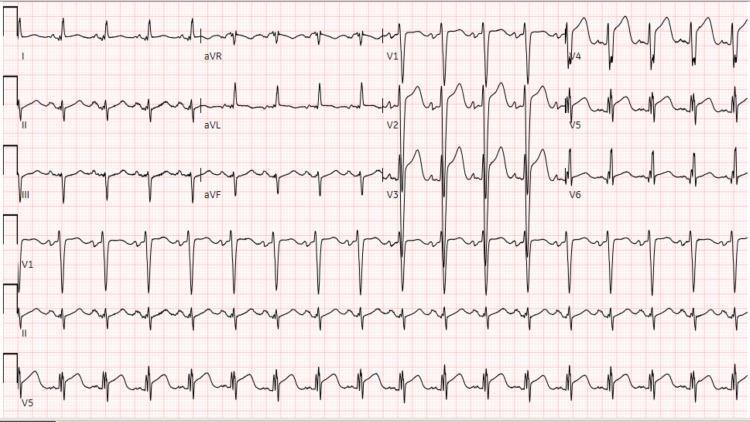
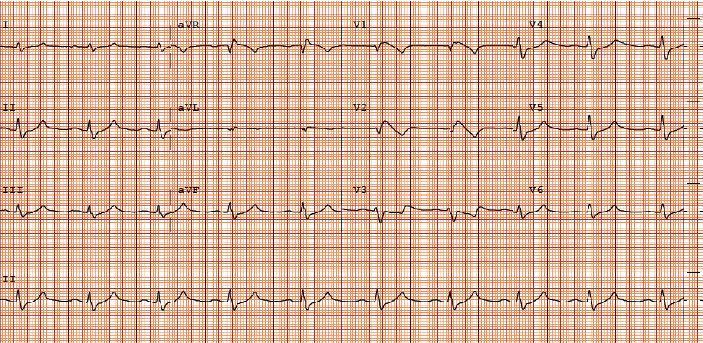
3. ⚡ Atrial Fibrillation (AF)
Key ECG Features:
- Absent P waves — replaced by chaotic fibrillatory (f) waves (best seen in V1, II)
- Irregularly irregular R-R intervals (hallmark)
- Narrow QRS complexes (unless aberrant conduction)
- Ventricular rate 100–160 bpm if uncontrolled
Coarse AF (f waves >1 mm) vs fine AF (f waves <1 mm — may look like isoelectric baseline).
4. 🔌 Complete (Third-Degree) AV Block
Key ECG Features:
- Complete AV dissociation — P waves and QRS complexes march independently
- Atrial rate > ventricular escape rate
- Regular P-P intervals AND regular R-R intervals (both regular, but unrelated)
- Escape QRS morphology:
- Narrow (junctional escape, rate 40–60 bpm) — higher block
- Wide (ventricular escape, rate 20–40 bpm) — infranodal block

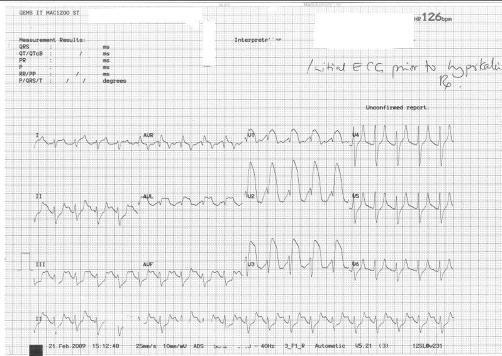
5. 🌩 Hyperkalemia
Key ECG Features (progressive with rising K⁺):
| K⁺ Level | ECG Change |
|---|---|
| 5.5–6.5 mEq/L | Tall, peaked ("tented") T waves — narrow base, symmetric |
| 6.5–7.5 mEq/L | Prolonged PR, flattened/absent P waves |
| 7.5–8.0 mEq/L | Widened QRS (intraventricular conduction delay) |
| >8.0 mEq/L | Sine wave pattern → VF → asystole |
6. 🚧 Left Bundle Branch Block (LBBB)
Key ECG Features (WiLLiaM mnemonic — W in V1, M in V6):
- QRS ≥120 ms (complete LBBB)
- Deep, broad S waves in V1–V3
- Broad, notched ("M-shaped" or monophasic) R waves in I, aVL, V5–V6
- No septal Q waves in lateral leads
- Discordant ST-T changes (ST and T wave opposite to QRS direction)
- Left axis deviation common
Clinical pearl: New LBBB in the context of chest pain = treat as STEMI equivalent (Sgarbossa criteria apply).
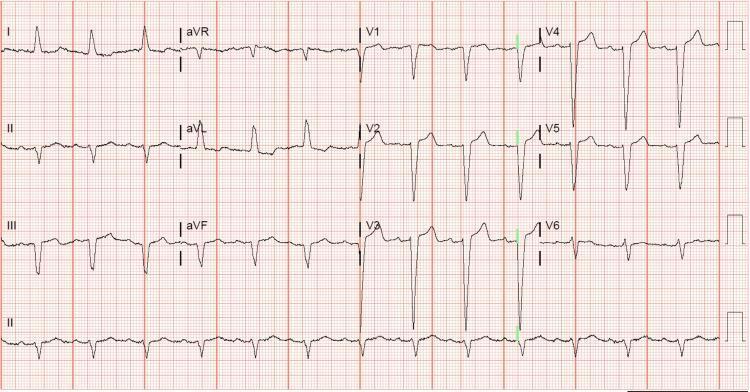
7. ⚠️ Brugada Syndrome (Type 1 Pattern)
Key ECG Features:
- Coved ST elevation ≥2 mm in V1–V2 with a descending ST segment directly into an inverted T wave (no isoelectric gap)
- Pseudo-RBBB morphology
- Normal QRS duration
- No actual structural heart disease
Three Brugada patterns:
| Type | Morphology | Clinical Significance |
|---|---|---|
| Type 1 (coved) | ST ≥2 mm coved + inverted T | Diagnostic |
| Type 2 (saddle-back) | ST ≥1 mm with upright/biphasic T | Suggestive, needs provocation |
| Type 3 | ST <1 mm | Not diagnostic alone |
Associated with SCN5A mutation (sodium channel), risk of sudden cardiac death.
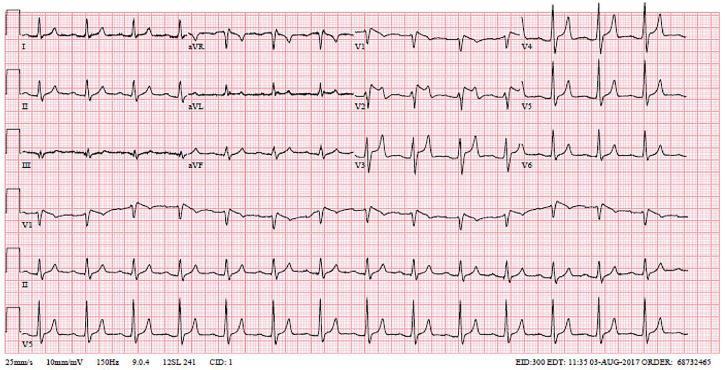
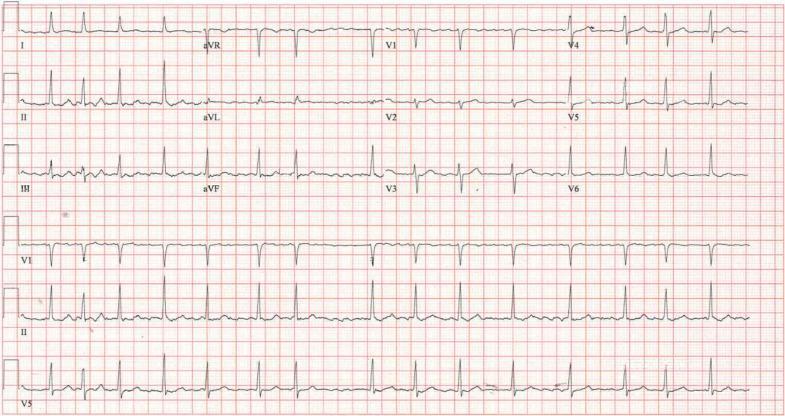
8. 🔁 Wolff-Parkinson-White (WPW) Syndrome
Key ECG Features (classic triad):
- Short PR interval (<120 ms) — accessory pathway bypasses AV node
- Delta wave — slurred upstroke at start of QRS (pre-excitation)
- Widened QRS >120 ms (due to fusion of normal + accessory conduction)
- Secondary ST-T changes — discordant with QRS
Localising the accessory pathway: Delta wave polarity in various leads predicts location (e.g., positive delta in V1 = left-sided pathway; negative delta in inferior leads = posteroseptal pathway).
Risk: WPW + AF can conduct at very high rates via accessory pathway → pre-excited AF → VF.

9. 🌀 Torsades de Pointes (TdP) / Long QT Syndrome
Long QT ECG:
- QTc >450 ms (men), >460 ms (women) — corrected with Bazett's formula
- T-wave morphology abnormalities (bifid T waves in LQT2, broad-based in LQT1)
Torsades de Pointes ECG:
- Polymorphic ventricular tachycardia with QRS complexes that appear to "twist" around the isoelectric baseline
- Rate 200–250 bpm
- Classic initiator: pause-dependent onset (long-short RR sequence)
- Preceded by prolonged QT on baseline ECG
Common causes: Electrolyte disturbances (↓K⁺, ↓Mg²⁺), drugs (antiarrhythmics, antipsychotics, antibiotics), congenital LQTS.
Treatment: IV magnesium sulfate 2g, overdrive pacing, remove offending agents.

10. 🫁 Pulmonary Embolism (PE)
Key ECG Features (right heart strain pattern):
- Sinus tachycardia — most common finding (seen in >40%)
- S1Q3T3 pattern — S wave in lead I, Q wave + T-wave inversion in lead III (seen in ~20%)
- Right axis deviation
- Incomplete or complete RBBB
- T-wave inversions V1–V4 (right ventricular strain)
- P pulmonale (tall P wave >2.5 mm in II)
- Right precordial ST changes
None of these changes are specific — ECG is primarily used to exclude other diagnoses (e.g., STEMI, pericarditis) in suspected PE.

Quick Reference Summary
| # | Condition | Key ECG Finding | Emergency? |
|---|---|---|---|
| 1 | STEMI | Convex ST elevation + reciprocal depression | 🔴 Yes — PCI |
| 2 | Pericarditis | Diffuse concave ST elevation + PR depression | 🟡 Urgent eval |
| 3 | Atrial Fibrillation | Absent P waves, irregular R-R | 🟡 Rate/rhythm control |
| 4 | Complete AV Block | AV dissociation, slow escape | 🔴 Yes — pacing |
| 5 | Hyperkalemia | Peaked T → sine wave | 🔴 Yes — calcium IV |
| 6 | LBBB | Wide QRS, notched R V6, deep S V1 | 🟡 If new + chest pain |
| 7 | Brugada | Coved ST V1–V2, inverted T | 🔴 ICD referral |
| 8 | WPW | Short PR + delta wave | 🟡 Ablation referral |
| 9 | Torsades de Pointes | Twisting polymorphic VT | 🔴 Yes — Mg²⁺ IV |
| 10 | Pulmonary Embolism | S1Q3T3, sinus tachycardia | 🔴 Yes — anticoagulation |
This is a shared conversation. Sign in to Orris to start your own chat.