Tetanus prophylaxis in neet pg aspects
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Searching the Web
tetanus prophylaxis NEET PG high yield points wound management 2024
I now have all the information needed for a comprehensive, high-yield NEET PG answer. Let me compile it:
Tetanus Prophylaxis - High-Yield NEET PG
1. Causative Organism & Mechanism
- Caused by Clostridium tetani - gram-positive, anaerobic, spore-forming bacillus
- Produces tetanospasmin (exotoxin) - blocks inhibitory neurotransmitters (GABA, glycine) at spinal interneurons → spastic paralysis
- Tetanus does NOT confer natural immunity (toxin concentration lethal before immune response) - a classic NEET PG fact
2. Classification of Wounds (KEY EXAM TABLE)
| Feature | Tetanus-Prone Wound | Non-Tetanus-Prone (Clean Minor) Wound |
|---|---|---|
| Age of wound | > 6 hours old | < 6 hours old |
| Depth | > 1 cm deep | Superficial |
| Contamination | Soil, feces, saliva, rust | Minimally contaminated |
| Tissue | Devitalized / necrotic tissue | No devitalized tissue |
| Type | Stellate, crush, explosion, burn, frostbite, puncture, animal bite | Clean laceration |
| Foreign body | Present | Absent |
Mnemonic for tetanus-prone wounds: "DASHED" - Devitalized tissue, Avascular/ischemic tissue, Soil/fecal contamination, Hours >6, Embedded foreign body, Deep puncture
3. Prophylaxis Decision Table (THE MOST IMPORTANT TABLE FOR NEET PG)
| Prior Tetanus Toxoid Doses | Clean Minor Wound | All Other Wounds (Tetanus-Prone) | ||
|---|---|---|---|---|
| Toxoid | TIG | Toxoid | TIG | |
| Unknown or <3 doses | YES | NO | YES | YES |
| ≥3 doses, last dose <5 yr | NO | NO | NO | NO |
| ≥3 doses, last dose 5-10 yr | NO | NO | YES | NO |
| ≥3 doses, last dose >10 yr | YES | NO | YES | NO |
The critical rule:
- TIG is ONLY given when: (a) Tetanus-prone wound AND (b) incomplete/unknown immunization (<3 doses)
- 5-year rule = tetanus-prone wounds get booster if last dose >5 years
- 10-year rule = clean wounds get booster if last dose >10 years
(Source: Tintinalli's Emergency Medicine; Harriet Lane Handbook; Miller's Review of Orthopaedics)
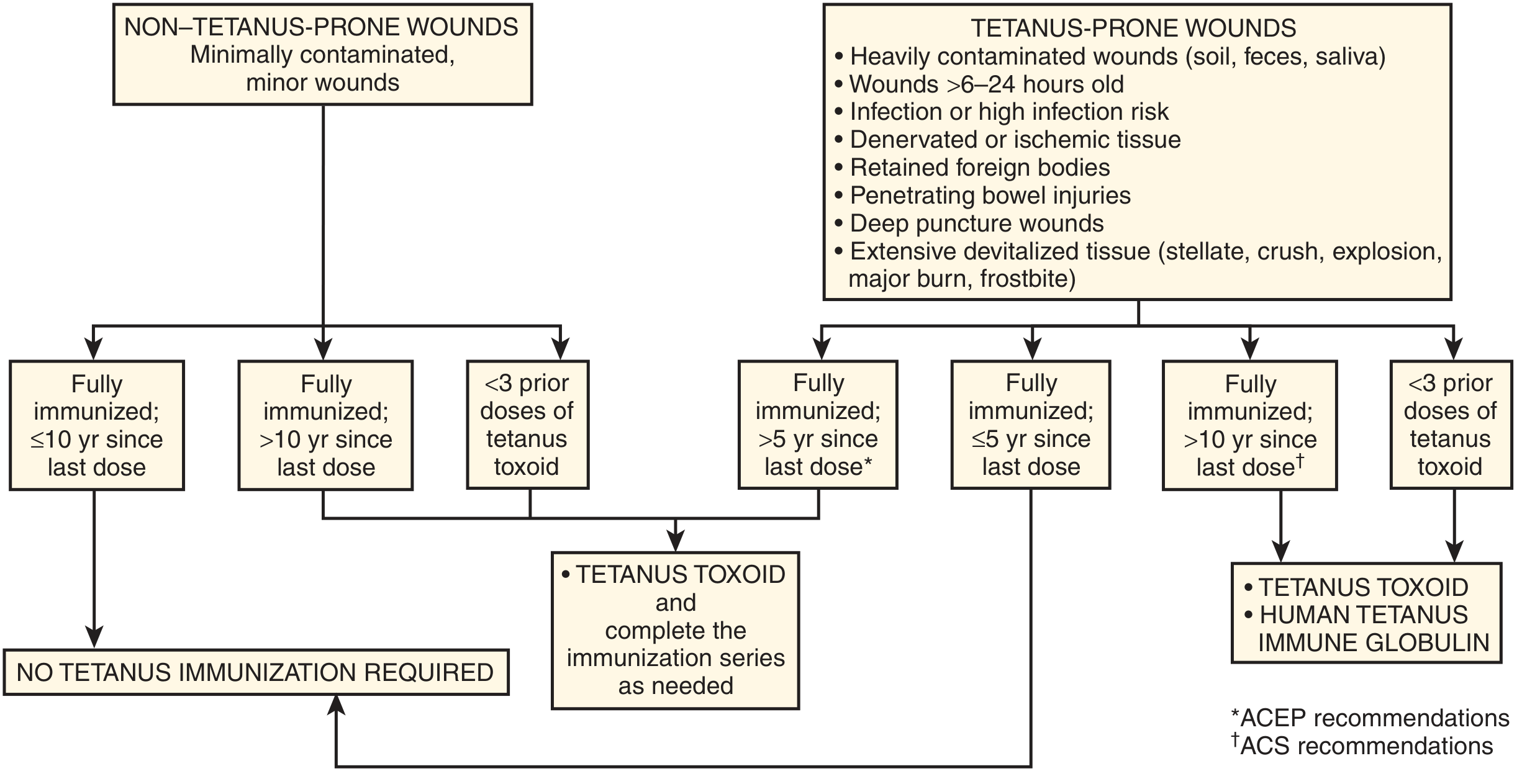
4. Prophylaxis Flowchart
5. Drugs Used - Doses (HIGH YIELD)
Active Immunization (Tetanus Toxoid)
| Vaccine | Age Group | Dose | Route |
|---|---|---|---|
| DTaP | < 7 years | 0.5 mL | IM |
| Tdap | ≥ 7 years (preferred) | 0.5 mL | IM |
| Td | Adults | 0.5 mL | IM |
- Primary series: 3 doses (0, 6 weeks, 12 months)
- Routine booster: every 10 years
Passive Immunization (TIG - Tetanus Immune Globulin)
| Indication | Dose |
|---|---|
| Prophylaxis | 250 units IM |
| Treatment (therapeutic) | 3000-6000 units IM |
- TIG = human tetanus immunoglobulin (preferred - no serum sickness)
- ATS (Equine Antitetanus Serum) = older, risk of anaphylaxis, 1500 IU IM for prophylaxis
- When both toxoid and TIG are given: use separate syringes at different sites
(Source: Park's Preventive & Social Medicine; Washington Manual; Roberts & Hedges' Clinical Procedures)
6. Contraindications to Tetanus Toxoid
- History of neurologic or severe systemic reaction after a previous dose
- Mild local reactions (erythema, induration, pain) are NOT contraindications
7. Antibiotics in Tetanus Prophylaxis (Park's - NEET PSM)
- Active immunization (toxoid) = ideal method but no immediate effect
- Penicillin: Benzathine penicillin 1.2 mega units IM (single dose) - covers 3-4 weeks
- Penicillin allergy: Erythromycin 500 mg 6-hourly × 7 days
- Must be given within 6 hours of injury (antibiotics kill vegetative forms, NOT spores)
- Antibiotics are NOT a substitute for immunization - only adjunct
8. Special Scenarios (Exam Favorites)
| Scenario | Management |
|---|---|
| Unimmunized patient, clean wound | Toxoid YES + TIG NO + complete primary series |
| Unimmunized patient, dirty wound | Toxoid YES + TIG YES |
| Fully immunized, last booster 3 years ago, dirty wound | Nothing needed (< 5 years) |
| Fully immunized, last booster 7 years ago, dirty wound | Toxoid YES + TIG NO |
| Fully immunized, last booster 12 years ago, clean wound | Toxoid YES (>10 years) |
| Burns >10% TBSA | 0.5 mL toxoid; if last booster >10 years or unknown → add TIG 250 units |
| Pregnant (unimmunized) | 2 doses TT between 16-36 weeks, ≥1 month apart, ≥3 weeks before delivery |
9. Neonatal Tetanus - Prevention
- "Five Cleans": Clean hands, clean delivery surface, clean blade, clean cord tie, clean cord stump (no application)
- Maternal TT during pregnancy protects neonates (transplacental IgG)
- Training birth attendants alone reduces neonatal tetanus deaths by 90%
10. Key One-Liners for MCQs
- Tetanus does NOT give natural immunity - most asked concept
- TIG dose for prophylaxis = 250 units IM; for treatment = 3000-6000 units
- 5-year rule for dirty wounds; 10-year rule for clean wounds (when booster needed)
- TIG and toxoid given at different sites simultaneously
- Preferred passive immunization = human TIG (not horse ATS - risk of serum sickness/anaphylaxis)
- Tetanus-prone wound: >6 hours old, devitalized tissue, contaminated, >1 cm deep
- Contraindication to toxoid = prior neurologic reaction (not local reaction)
- In children <7 years use DTaP; ≥7 years use Tdap (preferred) or Td
- Antibiotic prophylaxis: penicillin kills vegetative forms only, not spores
- Tdap preferred in adults who have never received it (also covers pertussis)
This is a shared conversation. Sign in to Orris to start your own chat.