Staghorn stones
Reading File
Finding Sources
Finding Sources
Searching PubMed
"staghorn calculi" management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive answer. Here is a full synthesis:
Staghorn Calculi
Definition
Staghorn calculi are large renal stones that occupy most or all of the renal collecting system - the renal pelvis and one or more surrounding infundibula and calyces. The name comes from their branched appearance on imaging, resembling a stag's antlers. There is no universally standardized definition, but by convention:
-
Complete staghorn: occupies the entire collecting system
-
Partial staghorn: extends into some but not all calyces
-
Campbell-Walsh-Wein Urology, p. 2754
Composition
While struvite (magnesium ammonium phosphate) is the classic and most common composition, any stone type can form a staghorn configuration:
| Composition | Notes |
|---|---|
| Struvite (MgNH₄PO₄) | Most common; infection-related |
| Calcium carbonate apatite | Co-precipitates with struvite |
| Cystine | Autosomal recessive disorder |
| Uric acid | Less common |
| Calcium oxalate | Can form staghorn in favorable anatomy |
A notable caveat: one series of 52 complete staghorn stones found 56% were metabolic in nature and 44% were infectious - a reminder that not all staghorn stones are struvite.
- Campbell-Walsh-Wein Urology, p. 2758
Pathogenesis of Struvite Stones
Struvite stones form only in the presence of urease-producing bacteria. The mechanism:
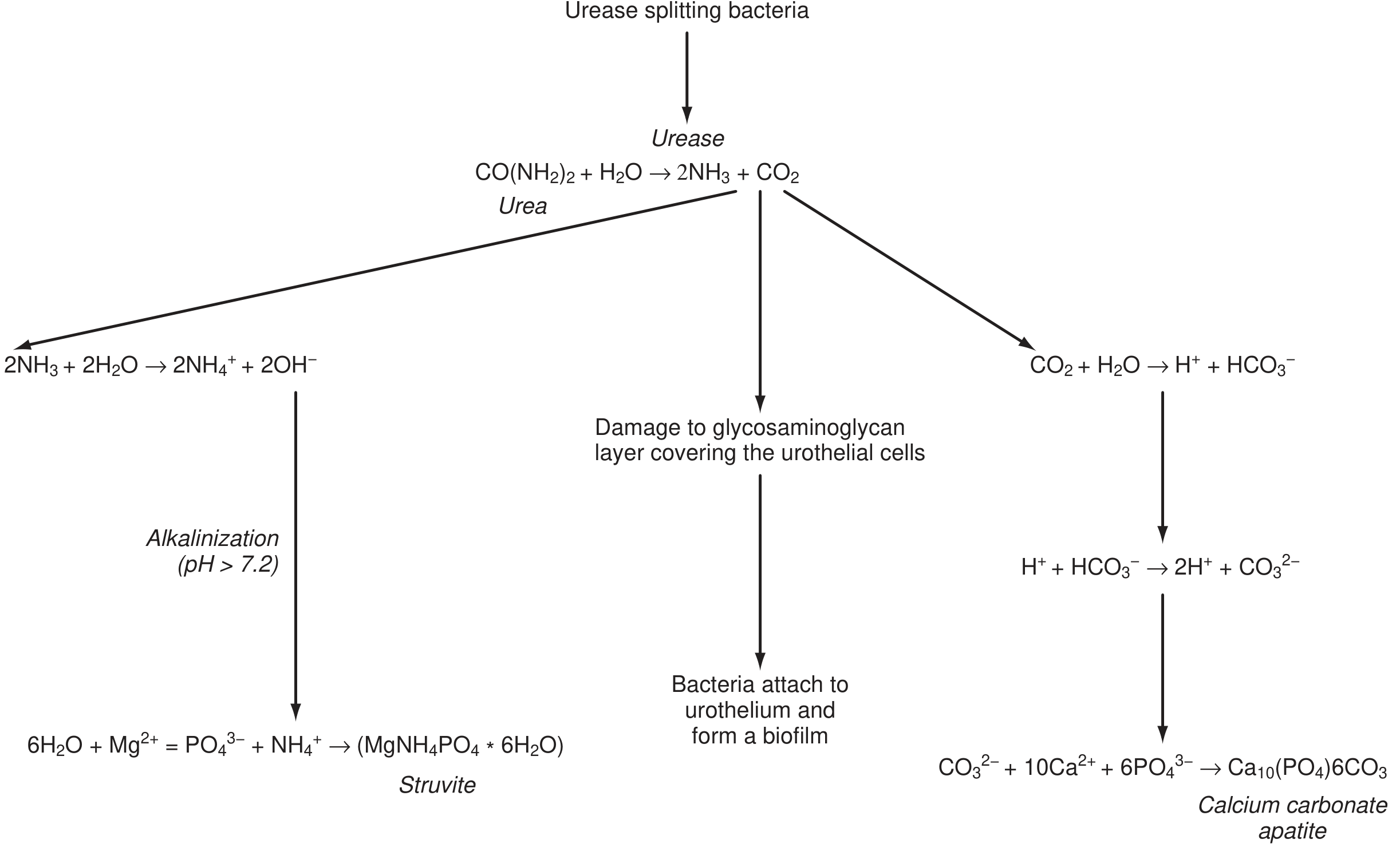
- Urease-splitting bacteria hydrolyze urea: CO(NH₂)₂ + H₂O → 2NH₃ + CO₂
- NH₃ + H₂O → NH₄⁺ + OH⁻ → alkalinizes urine (pH >7.2)
- At alkaline pH, phosphate becomes insoluble and precipitates with Mg²⁺ and NH₄⁺ → struvite (MgNH₄PO₄·6H₂O)
- CO₂ → CO₃²⁻, which combines with Ca²⁺ and PO₄³⁻ → calcium carbonate apatite
- Ammonia also damages the glycosaminoglycan layer of the urothelium, allowing bacteria to attach and form a biofilm - which perpetuates stone growth
Key urease-producing organisms:
| Usually (>90%) | Occasionally (5-30%) |
|---|---|
| Proteus mirabilis, P. vulgaris, P. rettgeri | Klebsiella pneumoniae |
| Staphylococcus aureus | Pseudomonas aeruginosa |
| Haemophilus influenzae | Serratia marcescens |
| Bordetella pertussis | Enterococcus spp. |
Note: E. coli - the most common uropathogen - does not produce urease (only ~1.4% of strains do).
- Campbell-Walsh-Wein Urology, p. 2736; Goldman-Cecil Medicine, p. 1290; Comprehensive Clinical Nephrology, p. 706
Risk Factors
- Female sex (increased susceptibility to upper UTI)
- Indwelling urinary catheters
- Neurogenic bladder
- Spinal cord injury
- Urinary tract anomalies with stasis
- Prior urologic surgery
Natural History (Why Treatment is Mandatory)
Untreated staghorn stones carry a serious prognosis:
- 50% complete renal function loss in affected kidney within 2 years
- Recurrent UTIs and urosepsis
- End-stage renal disease
- Increased overall mortality (up to 28% in some series)
- Conservative management carries nephrectomy rates up to 50%
The AUA guideline (2016, with specific staghorn guidance from 2005) advocates for surgical treatment in all patients healthy enough to undergo it, with complete stone clearance as the goal.
- Campbell-Walsh-Wein Urology, p. 2754; Comprehensive Clinical Nephrology, p. 2403
Surgical Management
The diagram below shows the three PCNL access routes for a complete staghorn stone:
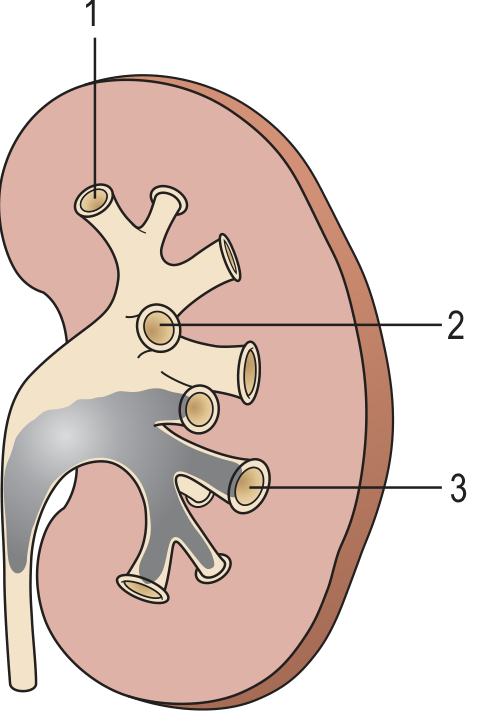
First-Line: Percutaneous Nephrolithotomy (PCNL)
PCNL is the method of choice for both partial and complete staghorn stones (AUA and EAU guideline recommendation).
Stone-free rates by modality:
| Modality | Stone-free rate |
|---|---|
| PCNL | ~78% (up to 91-96%) |
| Open nephrolithotomy | ~71-85% |
| SWL monotherapy | 22-54% |
Key PCNL principles for staghorn stones:
- Upper pole access is generally preferred for single-tract approach - allows access to upper pole, renal pelvis, and many lower pole stones with the rigid nephroscope; mid-calyceal stones treated with flexible nephroscopy
- Flexible nephroscopy during PCNL improves clearance and reduces the number of access tracts needed
- Multiple tracts are often required for complete calculi
- Retrograde flexible ureteroscopy (URS) can be used as an adjunct (ECIRS - endoscopic combined intrarenal surgery)
SWL (Shockwave Lithotripsy)
- Should not be used as monotherapy for staghorn stones
- High failure rate + risk of steinstrasse (stone street)
- In the only prospective RCT comparing SWL vs. PCNL for staghorn stones, PCNL provided superior stone-free rates (74% vs. 22%), shorter treatment duration, and fewer septic complications
- May be used as adjunct to PCNL (sandwich therapy) for residual inaccessible fragments
Ureteroscopy (URS)
- As sole modality for complete staghorn stones: highly unlikely to succeed and not recommended
- May be considered for simple partial staghorn stones with favorable anatomy or PCNL contraindications, but often requires multiple stages
Laparoscopic/Robotic Approaches
- Described in small series; stone-free rates relatively low (29-67%)
- No obvious advantage over PCNL in routine cases
- May help in ectopic kidneys where percutaneous access is challenging
Open Nephrolithotomy
- Now reserved for rare cases where PCNL is impossible or likely to fail within an acceptable number of procedures
- Stone-free rates up to 85%, but inferior to modern PCNL with respect to length of stay, transfusion risk, renal function loss, and recovery
Nephrectomy
-
Indicated for poorly functioning or nonfunctioning kidneys
-
Also appropriate when xanthogranulomatous pyelonephritis is present
-
Conservative therapy without treatment leads to nephrectomy in up to 50% of patients
-
Campbell-Walsh-Wein Urology, pp. 2758-2762; Comprehensive Clinical Nephrology, p. 2403-2405; Brenner & Rector's The Kidney, p. 1252
Prevention and Medical Management
Complete stone clearance is essential for infectious stones - residual fragments harbor urease-producing bacteria within the stone matrix, perpetuating bacteriuria and enabling rapid stone recurrence. PCNL achieves stone-free status ~90% of the time; recurrence rate is only ~10% in stone-free kidneys vs. ~60% at 6 months if fragments remain (Brenner & Rector data).
Post-treatment measures:
- Treat underlying UTI with appropriate antibiotics
- Surveillance urine cultures
- Urease inhibitor acetohydroxamic acid (AHA) can be used adjunctively but has significant side effects (thromboembolism, neuropsychiatric effects)
- Urine acidification with vitamin C or ammonium chloride to keep pH <6.5
- Address predisposing structural/functional abnormalities (catheterizable channels, neurogenic bladder management)
Summary Box
| Feature | Detail |
|---|---|
| Definition | Branched stone filling renal pelvis ± calyces |
| Predominant composition | Struvite (infection), but also cystine, uric acid, CaOx |
| Causative bacteria | Proteus spp., Staph aureus, Klebsiella (not E. coli) |
| Key mechanism | Urease → alkaline urine → MgNH₄PO₄ precipitation |
| Untreated consequence | 50% renal loss at 2 years; urosepsis; death |
| First-line treatment | PCNL |
| SWL | Adjunct only; never monotherapy |
| Goal | Complete stone clearance (stone free) |
Recent evidence note: A 2024 systematic review and meta-analysis (PMID 39120845) on robotic pyelolithotomy for large renal stones (including staghorn configuration) confirms feasibility of robotic approaches as an emerging option, though PCNL remains the established standard.
This is a shared conversation. Sign in to Orris to start your own chat.