Make simplefy ABG analysis from basic to clinical
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Here is a complete, simplified guide to ABG analysis from basic concepts all the way to clinical application.
ABG Analysis: From Basic to Clinical
PART 1 - What Is an ABG?
An arterial blood gas (ABG) is a blood sample taken from an artery (usually the radial artery). It directly measures the partial pressures of oxygen and carbon dioxide in arterial blood, along with pH, and estimated bicarbonate (HCO3-). It may also report lactate, hemoglobin, and electrolytes on modern analyzers.
"By using the combination of an arterial blood gas sample and serum electrolyte levels, a patient's acid-base status can be evaluated." - Roberts and Hedges' Clinical Procedures in Emergency Medicine
PART 2 - Normal Values (Memorize These)
| Parameter | Normal Range | Mnemonic |
|---|---|---|
| pH | 7.35 - 7.45 | Neutral = 7.40 |
| PaCO2 | 35 - 45 mmHg | Lungs control this |
| HCO3- | 22 - 26 mEq/L | Kidneys control this |
| PaO2 | 80 - 100 mmHg | Oxygenation |
| SaO2 | 94 - 100% | Saturation |
| Base Excess (BE) | -2 to +2 | Metabolic buffer |
Quick memory trick:
- pH < 7.35 = Acidosis
- pH > 7.45 = Alkalosis
- PaCO2 up = More acid (respiratory)
- HCO3- down = More acid (metabolic)
PART 3 - The Henderson-Hasselbalch Equation (The Foundation)
pH = 6.1 + log [HCO3-] / (0.03 × PaCO2)
In simple terms:
- CO2 = respiratory acid (controlled by lungs, minute-to-minute)
- HCO3- = metabolic base (controlled by kidneys, over hours to days)
The body defends pH by adjusting one when the other goes wrong.
PART 4 - The 4 Primary Disorders
| Disorder | pH | Primary Change | Compensation |
|---|---|---|---|
| Respiratory Acidosis | Low | PaCO2 ↑ | HCO3- ↑ (kidneys) |
| Respiratory Alkalosis | High | PaCO2 ↓ | HCO3- ↓ (kidneys) |
| Metabolic Acidosis | Low | HCO3- ↓ | PaCO2 ↓ (lungs hyperventilate) |
| Metabolic Alkalosis | High | HCO3- ↑ | PaCO2 ↑ (lungs hypoventilate) |
PART 5 - Compensation Formulas (The Numbers)
Compensation is the body's attempt to bring pH back toward normal. It never fully corrects the pH - that would require treatment of the underlying cause.
Metabolic Disorders (Respiratory Compensation - Fast, minutes-hours)
| Disorder | Formula |
|---|---|
| Metabolic Acidosis | Expected PaCO2 = 1.5 × HCO3- + 8 ± 2 (Winter's formula) |
| OR: ↓PaCO2 = 1.3 × ↓HCO3- | |
| Metabolic Alkalosis | Expected PaCO2 = 0.7 × HCO3- + 21 |
| OR: ↑PaCO2 = 0.6 × ↑HCO3- |
Respiratory Disorders (Metabolic Compensation - Slow, 3-5 days)
| Disorder | Acute (buffer response) | Chronic (renal response) |
|---|---|---|
| Resp. Acidosis | HCO3- ↑ 1 mEq/L per 10 mmHg ↑ PaCO2 | HCO3- ↑ 4 mEq/L per 10 mmHg ↑ PaCO2 |
| Resp. Alkalosis | HCO3- ↓ 2 mEq/L per 10 mmHg ↓ PaCO2 | HCO3- ↓ 5 mEq/L per 10 mmHg ↓ PaCO2 |
Important: "Respiratory compensation for metabolic disorders is more rapid and occurs through a change in the respiratory rate... Metabolic compensation for a respiratory disturbance requires renal adjustment of HCO3- and can take 3 to 5 days." - Schwartz's Principles of Surgery
PART 6 - Step-by-Step ABG Interpretation (The 5-Step Method)
Step 1 - Is the patient acidemic or alkalemic?
- pH < 7.35 → Acidosis
- pH > 7.45 → Alkalosis
- pH 7.35-7.45 → Could still have a disorder (look at CO2 and HCO3-)
Step 2 - What is the primary disorder?
- Acidosis + PaCO2 ↑ → Respiratory Acidosis
- Acidosis + HCO3- ↓ → Metabolic Acidosis
- Alkalosis + PaCO2 ↓ → Respiratory Alkalosis
- Alkalosis + HCO3- ↑ → Metabolic Alkalosis
If the pH is normal but CO2 and HCO3- are both abnormal, there is likely a mixed disorder.
Step 3 - Is there appropriate compensation?
Use the formulas from Part 5. If compensation is MORE or LESS than expected, a second disorder is present.
Step 4 - Calculate the Anion Gap (if metabolic acidosis)
Anion Gap (AG) = Na+ - (Cl- + HCO3-)
Normal = 8-12 mEq/L (or up to 16 if not albumin-corrected)
- AG > 12 = High AG metabolic acidosis (MUDPILES mnemonic below)
- AG normal (8-12) = Non-AG (hyperchloremic) metabolic acidosis (HARDUP mnemonic below)
Step 5 - Assess oxygenation
- PaO2 < 80 mmHg = Hypoxemia
- Check the P/F ratio = PaO2 / FiO2
- Normal: > 400
- Mild ARDS: 200-300
- Moderate ARDS: 100-200
- Severe ARDS: < 100
PART 7 - Anion Gap Acidosis: The MUDPILES Causes
When AG > 12, an unmeasured anion is consuming bicarbonate. The conjugate base of the culprit acid raises the AG while HCO3- falls.
| Letter | Cause |
|---|---|
| M | Methanol |
| U | Uremia |
| D | DKA (Diabetic Ketoacidosis) |
| P | Propylene glycol / Paracetamol (acetaminophen OD) |
| I | Isoniazid / Iron |
| L | Lactic acidosis |
| E | Ethylene glycol |
| S | Salicylates |
PART 8 - Non-Anion Gap (Normal AG) Acidosis: HARDUP Causes
In non-AG acidosis, HCO3- is lost and replaced by Cl-, so the gap stays normal but the patient is acidotic.
| Letter | Cause |
|---|---|
| H | Hyperalimentation (TPN) |
| A | Addison's disease / Acetazolamide |
| R | Renal Tubular Acidosis (RTA) |
| D | Diarrhea (GI HCO3- loss) |
| U | Ureteral diversions |
| P | Pancreatic fistula / Post-hypocapnia |
PART 9 - The Delta-Delta (ΔΔ) Ratio (Advanced: Detecting Mixed Disorders)
When you find a high AG metabolic acidosis, ask: is there also a hidden metabolic alkalosis or a non-AG acidosis?
ΔAG = Calculated AG - 12 (rise in AG)
ΔHCO3- = 24 - Measured HCO3- (fall in HCO3-)
Delta-Delta ratio = ΔAG / ΔHCO3-
| Ratio | Interpretation |
|---|---|
| < 1 | Concurrent non-AG metabolic acidosis |
| 1 - 2 | Pure high AG metabolic acidosis |
| > 2 | Concurrent metabolic alkalosis |
"In pure AG metabolic acidosis, the decrease in serum HCO3- should be roughly the same as the ΔAG (i.e., ratio of ΔAG to ΔHCO3- is roughly 1:1)." - Frameworks for Internal Medicine
PART 10 - The Acid-Base Map
This chart plots where a patient's values fall. Points within a named zone indicate a single disorder. Points between zones indicate a mixed disorder.
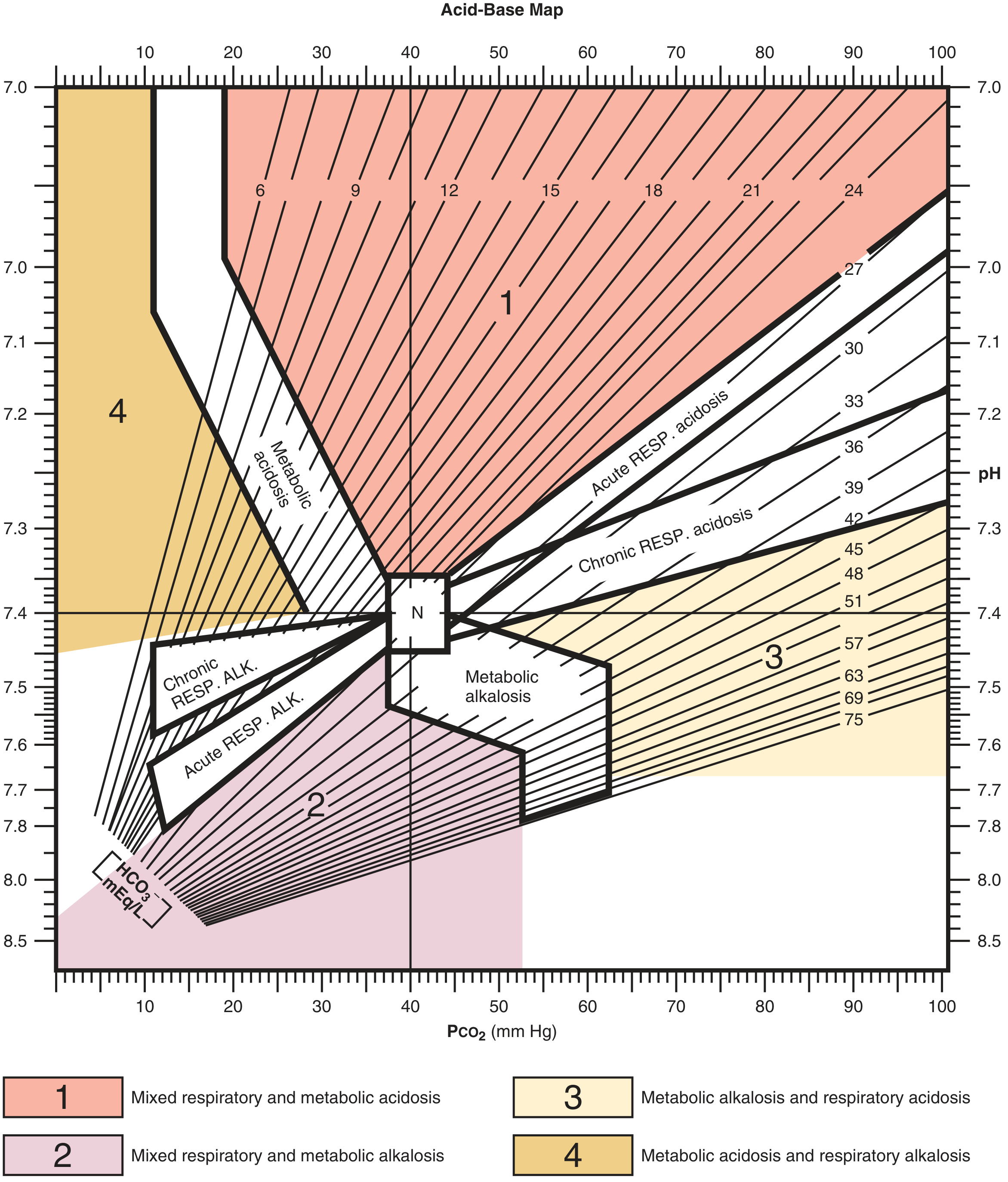
- Zone 1 (pink/red, high pH + high PaCO2): Mixed respiratory and metabolic acidosis
- Zone 2 (purple, low pH + low PaCO2): Mixed respiratory and metabolic alkalosis
- Zone 3 (tan, high pH + high PaCO2): Metabolic alkalosis + respiratory acidosis
- Zone 4 (gold, low pH + low PaCO2): Metabolic acidosis + respiratory alkalosis
- N = Normal point (pH 7.40, PaCO2 40)
PART 11 - Common Causes of Each Disorder (Clinical Scenarios)
Respiratory Acidosis (PaCO2 ↑)
- COPD exacerbation, severe asthma
- Opioid/sedative overdose (respiratory depression)
- Neuromuscular disease (Guillain-Barre, myasthenia crisis)
- Obesity hypoventilation syndrome
Respiratory Alkalosis (PaCO2 ↓)
- Anxiety/hyperventilation
- Sepsis (early), pregnancy
- High altitude
- Salicylate poisoning (early phase - stimulates the respiratory center)
- Hepatic encephalopathy
Metabolic Acidosis (HCO3- ↓)
- Lactic acidosis (sepsis, shock, ischemia)
- DKA
- Renal failure (uremia)
- Diarrhea
- Toxic ingestions (methanol, ethylene glycol, salicylates)
Metabolic Alkalosis (HCO3- ↑)
- Vomiting (loss of HCl)
- NG suction
- Diuretics (loop and thiazides - volume contraction alkalosis)
- Hyperaldosteronism
- Exogenous bicarbonate or antacid overuse
PART 12 - Worked Clinical Examples
Example 1 - Diarrhea (from Roberts & Hedges)
58-year-old woman, 1 week of profuse diarrhea. Na+ 133, K+ 2.8, pH 7.26, Cl- 118, PaCO2 13, HCO3- 5.
- pH 7.26 → Acidosis
- HCO3- 5 (low), PaCO2 13 (low, not elevated) → Metabolic Acidosis
- AG = 133 - (118 + 5) = 10 → Normal AG → Non-AG metabolic acidosis (diarrhea causing HCO3- loss)
- Winter's formula: Expected PaCO2 = 1.5(5) + 8 = 15.5 ± 2. Actual PaCO2 = 13. Within range → Appropriate respiratory compensation only
Example 2 - Sepsis/Respiratory Alkalosis (from Roberts & Hedges)
74-year-old, septic shock, E. coli bacteremia. pH 7.49, PaCO2 25, HCO3- 22.
- pH 7.49 → Alkalosis
- PaCO2 25 (low) → Respiratory Alkalosis
- Expected HCO3- decrease: 2 mEq/L per 10 mmHg drop in PaCO2. Drop = 15 mmHg → expected ↓HCO3- = 3 mEq/L → expected HCO3- = 24 - 3 = 21 mEq/L. Actual = 22 → Appropriate compensation
- Cause: Sepsis drives hyperventilation via inflammatory cytokines stimulating the respiratory center
PART 13 - Quick Reference: ABG Interpretation Cheat Sheet
Step 1: pH → Acidosis (<7.35) or Alkalosis (>7.45)?
Step 2: CO2 or HCO3-? → Respiratory or Metabolic?
Step 3: Does compensation match the formula? → Simple or Mixed?
Step 4: If Met Acidosis → Calculate AG = Na - (Cl + HCO3-)
AG > 12 → MUDPILES
AG normal → HARDUP
Step 5: If High AG → Calculate Delta-Delta ratio
Step 6: PaO2 and P/F ratio → Assess oxygenation
Sources
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, Chapter on Acid-Base Balance
- Schwartz's Principles of Surgery, 11th Edition, Chapter 3
- Frameworks for Internal Medicine, Chapter 32
- Tintinalli's Emergency Medicine, ABG Analysis section
- Fishman's Pulmonary Diseases and Disorders, 2-Volume Set
Hii
Hi there! 👋 How can I help you today?
Make simplefy ABG analysis from basic to clinical
Here is a complete, simplified guide to ABG analysis — from the very basics to full clinical application.
🫁 ABG Analysis: Simplified from Basic to Clinical
PART 1 - What Is an ABG?
An Arterial Blood Gas (ABG) is a blood test taken from an artery (usually the radial artery) that tells you:
| What it measures | What it means |
|---|---|
| pH | How acid or alkaline the blood is |
| PaCO2 | How much CO2 is in the blood (lung function) |
| HCO3- | Bicarbonate level (kidney/metabolic function) |
| PaO2 | How much oxygen is dissolved in blood |
| SaO2 | % of hemoglobin carrying oxygen |
PART 2 - Normal ABG Values (Memorize These First)
| Parameter | Normal Value | Controlled By |
|---|---|---|
| pH | 7.35 - 7.45 | Lungs + Kidneys together |
| PaCO2 | 35 - 45 mmHg | Lungs (minute-to-minute) |
| HCO3- | 22 - 26 mEq/L | Kidneys (hours to days) |
| PaO2 | 80 - 100 mmHg | Lungs / inspired O2 |
| SaO2 | 94 - 100% | Hemoglobin binding |
| Base Excess | -2 to +2 | Metabolic buffer reserve |
Simple rule to remember:
- pH low = Acidosis
- pH high = Alkalosis
- CO2 up = more acid (respiratory)
- HCO3- down = more acid (metabolic)
PART 3 - The Core Concept: CO2 vs HCO3-
Think of it like a seesaw:
pH (balance point)
/ \
CO2 (acid) HCO3- (base)
Lungs control Kidneys control
(fast - minutes) (slow - days)
- When CO2 rises → blood becomes more acidic (respiratory acidosis)
- When HCO3- falls → blood becomes more acidic (metabolic acidosis)
- The body always tries to compensate by adjusting the other side
PART 4 - The 4 Primary Acid-Base Disorders
| Disorder | pH | Primary Change | Body's Compensation |
|---|---|---|---|
| Respiratory Acidosis | ↓ Low | PaCO2 ↑ | Kidneys retain HCO3- ↑ |
| Respiratory Alkalosis | ↑ High | PaCO2 ↓ | Kidneys excrete HCO3- ↓ |
| Metabolic Acidosis | ↓ Low | HCO3- ↓ | Lungs hyperventilate → PaCO2 ↓ |
| Metabolic Alkalosis | ↑ High | HCO3- ↑ | Lungs hypoventilate → PaCO2 ↑ |
PART 5 - Compensation Formulas
Compensation never fully corrects pH - it just minimizes the damage. If compensation is more or less than expected, a second disorder is hiding.
Metabolic Disorders (Lungs compensate - Fast)
| Disorder | Formula |
|---|---|
| Metabolic Acidosis | Expected PaCO2 = 1.5 × HCO3- + 8 ± 2 (Winter's Formula) |
| Metabolic Alkalosis | Expected PaCO2 = 0.7 × HCO3- + 21 |
Respiratory Disorders (Kidneys compensate - Slow, 3-5 days)
| Disorder | Acute Response | Chronic Response |
|---|---|---|
| Resp. Acidosis | HCO3- ↑ 1 mEq/L per 10 mmHg ↑ CO2 | HCO3- ↑ 4 mEq/L per 10 mmHg ↑ CO2 |
| Resp. Alkalosis | HCO3- ↓ 2 mEq/L per 10 mmHg ↓ CO2 | HCO3- ↓ 5 mEq/L per 10 mmHg ↓ CO2 |
PART 6 - The 5-Step ABG Interpretation Method
✅ Step 1 - Look at the pH
- pH < 7.35 → Acidosis
- pH > 7.45 → Alkalosis
- pH normal but CO2 and HCO3- both abnormal → likely mixed disorder
✅ Step 2 - Identify the Primary Disorder
- Acidosis + CO2 ↑ → Respiratory Acidosis
- Acidosis + HCO3- ↓ → Metabolic Acidosis
- Alkalosis + CO2 ↓ → Respiratory Alkalosis
- Alkalosis + HCO3- ↑ → Metabolic Alkalosis
✅ Step 3 - Check Compensation
Use the formulas above. Ask: "Is the compensation appropriate?"
- If YES → Simple single disorder
- If NO (too much or too little) → Mixed disorder
✅ Step 4 - Calculate Anion Gap (if metabolic acidosis)
Anion Gap = Na+ - (Cl- + HCO3-)
Normal = 8 - 12 mEq/L
- AG > 12 → High AG metabolic acidosis → MUDPILES causes
- AG normal → Non-AG (hyperchloremic) acidosis → HARDUP causes
✅ Step 5 - Assess Oxygenation
- PaO2 < 80 mmHg = Hypoxemia
- P/F Ratio = PaO2 ÷ FiO2
| P/F Ratio | Meaning |
|---|---|
| > 400 | Normal |
| 200 - 300 | Mild ARDS |
| 100 - 200 | Moderate ARDS |
| < 100 | Severe ARDS |
PART 7 - Anion Gap Causes: MUDPILES
When AG > 12, an unmeasured acid is consuming bicarbonate.
| Letter | Cause |
|---|---|
| M | Methanol |
| U | Uremia (renal failure) |
| D | Diabetic Ketoacidosis (DKA) |
| P | Propylene glycol / Paracetamol overdose |
| I | Isoniazid / Iron toxicity |
| L | Lactic acidosis (sepsis, shock) |
| E | Ethylene glycol |
| S | Salicylates (aspirin OD) |
PART 8 - Non-Anion Gap Causes: HARDUP
When AG is normal but pH is low, HCO3- is being lost (not consumed).
| Letter | Cause |
|---|---|
| H | Hyperalimentation (TPN) |
| A | Addison's disease / Acetazolamide |
| R | Renal Tubular Acidosis (RTA) |
| D | Diarrhea (GI bicarbonate loss) |
| U | Ureteral diversions |
| P | Pancreatic fistula / Post-hypocapnia |
PART 9 - Delta-Delta Ratio (Detect Hidden Mixed Disorders)
When you find a high AG metabolic acidosis, always check if another metabolic disorder is hiding:
Delta Ratio = ΔAG / ΔHCO3-
ΔAG = Calculated AG - 12
ΔHCO3- = 24 - Measured HCO3-
| Delta Ratio | Hidden Disorder |
|---|---|
| < 1 | Also has non-AG metabolic acidosis |
| 1 - 2 | Pure high AG metabolic acidosis only |
| > 2 | Also has metabolic alkalosis |
PART 10 - The Acid-Base Map
Plot your patient's pH and PaCO2 on this map. If the point falls inside a named zone, it's a single disorder. If it falls between zones, it's a mixed disorder.
PART 11 - Clinical Causes at a Glance
Respiratory Acidosis (CO2 ↑)
- COPD exacerbation, severe asthma
- Opioid/sedative overdose
- Neuromuscular failure (Guillain-Barre, MG crisis)
- Obesity hypoventilation
Respiratory Alkalosis (CO2 ↓)
- Anxiety / panic attack
- Sepsis (early), pregnancy
- High altitude
- Salicylate poisoning (early)
Metabolic Acidosis (HCO3- ↓)
- Sepsis/shock → lactic acidosis
- DKA
- Renal failure
- Diarrhea, toxic ingestions
Metabolic Alkalosis (HCO3- ↑)
- Vomiting / NG suction
- Diuretics (loop, thiazides)
- Hyperaldosteronism
- Antacid overuse
PART 12 - Worked Clinical Examples
Case 1 - COPD Patient in Respiratory Distress
pH 7.28, PaCO2 72, HCO3- 33, PaO2 52
- pH 7.28 → Acidosis
- PaCO2 72 (↑) → Respiratory Acidosis
- HCO3- 33 - check chronic compensation: ↑ by 4 per 10 mmHg CO2 rise = 4 × 3.2 = ~13 → expected HCO3- = 24 + 13 = 37. Actual is 33 - slightly less → mild concurrent metabolic acidosis possible
- PaO2 52 → Hypoxemia
- Diagnosis: Chronic respiratory acidosis with acute-on-chronic exacerbation + hypoxemia
Case 2 - Diabetic in ER
pH 7.15, PaCO2 20, HCO3- 7, Na 138, Cl 100
- pH 7.15 → Acidosis
- HCO3- 7 (↓), PaCO2 not elevated → Metabolic Acidosis
- Winter's: Expected PaCO2 = 1.5(7) + 8 = 18.5 ± 2. Actual = 20 → appropriate compensation
- AG = 138 - (100 + 7) = 31 → High AG metabolic acidosis
- Delta-Delta: ΔAG = 31-12 = 19; ΔHCO3- = 24-7 = 17; ratio = 19/17 = 1.1 → Pure high AG
- Diagnosis: DKA with pure high anion gap metabolic acidosis
Case 3 - Post-Vomiting Patient
pH 7.52, PaCO2 48, HCO3- 38
- pH 7.52 → Alkalosis
- HCO3- 38 (↑) → Metabolic Alkalosis
- Expected PaCO2 = 0.7(38) + 21 = 47.6 → Actual 48 → appropriate compensation
- Diagnosis: Metabolic alkalosis from vomiting (HCl loss) - fully compensated
PART 13 - Master Cheat Sheet
STEP 1: pH < 7.35 = Acidosis | pH > 7.45 = Alkalosis
STEP 2: CO2 ↑ = Resp Acidosis | CO2 ↓ = Resp Alkalosis
HCO3- ↓ = Met Acidosis | HCO3- ↑ = Met Alkalosis
STEP 3: Apply compensation formula → Simple or Mixed?
STEP 4: Met Acidosis → AG = Na - (Cl + HCO3-)
AG > 12 → MUDPILES
AG normal → HARDUP
STEP 5: High AG → Delta-Delta ratio → hidden disorder?
STEP 6: PaO2 and P/F ratio → oxygenation status
Sources: Roberts and Hedges' Clinical Procedures in Emergency Medicine | Schwartz's Principles of Surgery, 11th Ed. | Frameworks for Internal Medicine | Tintinalli's Emergency Medicine | Fishman's Pulmonary Diseases and Disorders
This is a shared conversation. Sign in to Orris to start your own chat.