Clinical features of diabetic kidney disease
Reading File
Finding Sources
Finding Sources
Searching PubMed
"diabetic kidney disease" clinical features
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent - I have a clear natural history diagram. Now I have comprehensive content from multiple top-tier textbooks to write a thorough answer.
Clinical Features of Diabetic Kidney Disease (DKD)
Diabetic kidney disease is the leading cause of end-stage renal disease (ESKD) worldwide, affecting approximately 40% of all patients with diabetes. It typically manifests 10-15 years after the onset of diabetes, though patients with type 2 diabetes (T2D) may present with advanced DKD at the time of diagnosis because onset of T2D is often unrecognized.
Natural History and Staging
The classical progression of DKD is best understood as a series of overlapping stages. The diagram below illustrates the changes in GFR and albuminuria over time:
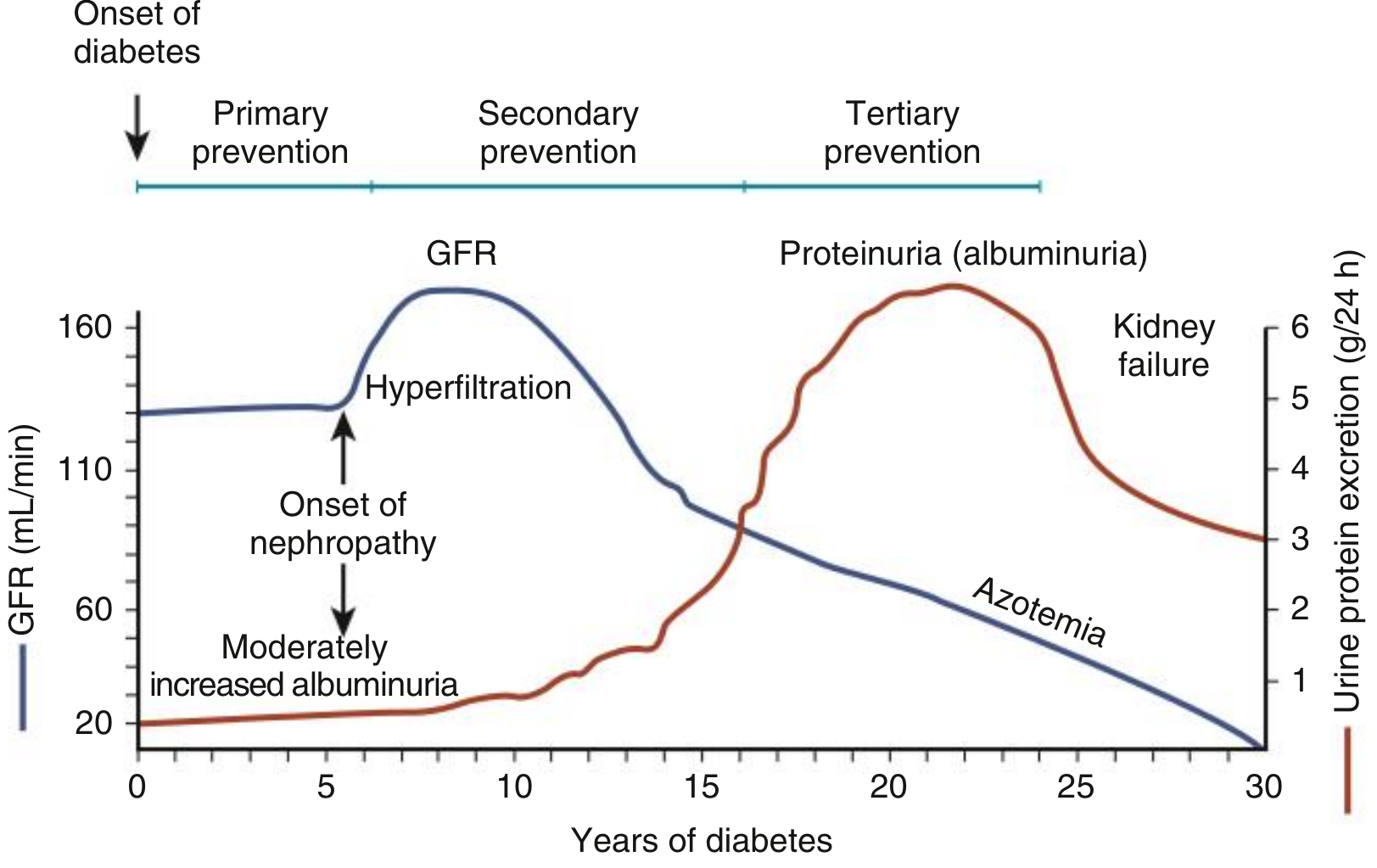
Fig. Natural History of Diabetic Nephropathy. GFR rises early (hyperfiltration), then declines; albuminuria increases progressively until kidney failure. - Comprehensive Clinical Nephrology, 7th Ed.
Stage-by-Stage Clinical Features
Stage 1 - Glomerular Hyperfiltration (Early, Functional)
- Elevated GFR (may reach 130-160 mL/min) due to glomerular hyperperfusion driven by hyperglycemia, RAAS activation, and SGLT2 upregulation in the proximal tubule
- Renal hypertrophy - kidney enlargement detectable on imaging
- No albuminuria - urine dipstick and routine urinalysis are normal
- No symptoms - entirely asymptomatic
- Begins within the first 5 years of diabetes onset
Harrison's Principles of Internal Medicine 22E
Stage 2 - Silent Structural Damage
- GFR returns toward normal
- Thickening of the glomerular basement membrane (GBM), mesangial expansion, and glomerular hypertrophy develop on biopsy but are not clinically apparent
- Still normoalbuminuric (UACR < 30 mg/g)
- No overt clinical symptoms
- Duration: approximately 5-10 years from onset
Stage 3 - Moderately Increased Albuminuria (Microalbuminuria)
- UACR 30-299 mg/g (or 30-300 mg/24 h) - not detectable by routine dipstick
- Appears 5-10 years after diabetes onset
- GFR may still be normal or mildly elevated
- Blood pressure begins to rise - often the first detectable clinical sign
- This stage is the key intervention window; regression to normoalbuminuria is possible with treatment
- In type 1 diabetes (T1D), microalbuminuria classically progresses over the next 5-10 years to overt proteinuria; in T2D, regression is more common with effective therapy
Harrison's Principles of Internal Medicine 22E
Stage 4 - Severely Elevated Albuminuria (Overt Proteinuria / Macroproteinuria)
- UACR ≥ 300 mg/g (equivalent to ≥ 500 mg/day total protein on dipstick)
- Proteinuria can range from 500 mg to as high as 25 g/24 hours
- GFR begins declining - rate of decline varies from 1.8 to 14 mL/min/year depending on treatment and comorbidities
- Hypertension is nearly universal at this stage
- Edema may develop - peripheral pitting edema from nephrotic-range proteinuria with hypoalbuminemia
- Nephrotic syndrome (proteinuria >3.5 g/day, hypoalbuminemia, edema) may develop when glomerulosclerosis is severe
- Azotemia (elevated blood urea nitrogen and creatinine) appears
- Diabetic retinopathy is present in > 90% of T1D patients with overt nephropathy (only ~50-60% in T2D)
Harrison's Principles of Internal Medicine 22E; Comprehensive Clinical Nephrology, 7th Ed.
Stage 5 - ESKD / Kidney Failure
- GFR < 15 mL/min/1.73 m²
- Features of uraemia: fatigue, nausea, vomiting, anorexia, pruritus, fluid overload
- Proteinuria may paradoxically decrease as GFR falls very low (less glomerular filtrate to lose protein into)
- Patients with DM have worse survival on dialysis than non-diabetics
- Kidney transplantation yields better outcomes than dialysis in eligible patients
Key Clinical Features at Presentation
| Feature | Detail |
|---|---|
| Proteinuria/Albuminuria | The cardinal feature; ranges from microalbuminuria to nephrotic-range proteinuria |
| Hypertension | Nearly universal; often the first clinical sign; worsens with progression |
| Edema | Peripheral pitting edema when nephrotic syndrome develops |
| Declining GFR / Azotemia | Progressive rise in creatinine and BUN |
| Diabetic Retinopathy | Present in >90% of T1D with nephropathy; 50-60% in T2D; absence in T1D should prompt biopsy |
| Neuropathy | Sensory polyneuropathy, autonomic neuropathy (gastroparesis, erectile dysfunction, neurogenic bladder), diabetic foot |
| Cardiovascular disease | Stroke, coronary disease, and peripheral vascular disease occur at 5x higher frequency in DKD vs. diabetics without DKD |
| Type IV RTA | Hyporeninemic hypoaldosteronism - propensity to hyperkalemia and metabolic acidosis |
| Anemia | Earlier and more severe than in non-diabetic CKD |
| Susceptibility to AKI | Increased risk with NSAIDs, radiocontrast agents, sepsis, or cardiovascular events |
Urinary Sediment
The urine sediment in DKD is typically bland - no more than occasional erythrocytes. The presence of dysmorphic RBCs, RBC casts, or active nephritic sediment is atypical and should raise suspicion for a superimposed non-diabetic glomerulonephritis.
Atypical Presentations Warranting Kidney Biopsy
DKD is usually a clinical diagnosis (diabetes + CKD + albuminuria without another obvious cause). Biopsy is reserved for:
- Frank hematuria with negative urological workup
- Rapid or accelerated decline in GFR
- Nephrotic-range albuminuria with normal GFR
- Absence of retinopathy in T1D with proteinuria
- Duration of T1D < 5 years with proteinuria
- Serological or clinical features suggesting a non-diabetic cause
Comprehensive Clinical Nephrology, 7th Ed.; NKF Primer on Kidney Diseases, 8th Ed.
Pathological Correlates of Clinical Stages
The renal lesions underlying these clinical features include:
- Glomerular basement membrane thickening - detectable by electron microscopy before clinical change; the earliest structural lesion
- Diffuse mesangial sclerosis - present in most patients after >10 years; causes nephrotic syndrome when severe; associated with hypertension
- Nodular glomerulosclerosis (Kimmelstiel-Wilson nodules) - ball-like deposits of laminated matrix in the glomerular periphery; found in 15-30% of long-term diabetics; virtually pathognomonic of DM; strongly correlates with retinopathy
- Hyaline arteriolosclerosis - uniquely affects both afferent and efferent arterioles in DM (efferent involvement is almost unique to diabetes); contributes to glomerular hypertension
- Nephrosclerosis - diffuse cortical scarring from ischemia; manifests as a finely granular cortical surface
- Pyelonephritis - more severe in diabetics; necrotizing papillitis (papillary necrosis) is more prevalent in diabetes
Robbins & Kumar Basic Pathology; Brenner & Rector's The Kidney, 2-Volume Set
Important Clinical Considerations
- Normoalbuminuric DKD: Up to 24% of T1D and 50% of T2D patients with CKD are normoalbuminuric - albuminuria is not universally required for diagnosis
- Cardiovascular risk: Albuminuria and decreased GFR are independent and potent risk factors for CV death - many patients die of CV events before reaching ESKD
- T2D asymmetry: In T2D, many patients have small kidneys and low GFR without significant albuminuria, possibly from macrovascular disease; atherosclerotic renal artery stenosis must be excluded
- Screening: T1D - screen 5 years after diagnosis; T2D - screen at diagnosis; both annually thereafter with spot UACR and eGFR
Sources: Harrison's Principles of Internal Medicine 22E | Comprehensive Clinical Nephrology, 7th Ed. | Brenner & Rector's The Kidney, 2-Vol Set | NKF Primer on Kidney Diseases, 8th Ed. | Robbins & Kumar Basic Pathology
This is a shared conversation. Sign in to Orris to start your own chat.