Tell me about compartment syndrome
Reading File
Finding Sources
Searching PubMed
"compartment syndrome" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Here is a detailed overview of compartment syndrome:
Compartment Syndrome
Definition
Compartment syndrome is raised pressure within a closed osseofascial (bone-and-fascia-bounded) compartment to a level that compromises tissue perfusion. When tissue pressure exceeds capillary perfusion pressure, oxygen delivery fails and ischaemia progresses to irreversible muscle and nerve necrosis if untreated. - Bailey and Love's Short Practice of Surgery, 28th Ed.
Causes
Fractures account for ~70% of cases, soft tissue contusions for ~23%. Less common causes include:
- Reperfusion/post-ischaemic swelling after arterial repair or embolectomy
- Circumferential third-degree burns
- Bleeding disorders or anticoagulation
- Tight circumferential casts or dressings
- IV extravasation (contrast under pressure, intraosseous infusion leaks)
- Combined arterial and venous injury
- Prolonged crush injury
(Bailey and Love's; Rosen's Emergency Medicine)
Pathophysiology
The underlying mechanism follows a vicious cycle:
- Swelling or bleeding within a non-expandable fascial compartment raises tissue pressure.
- Elevated pressure compresses venules and capillaries, reducing microperfusion below the threshold needed to sustain muscle and nerve viability.
- Ischaemia triggers reperfusion injury - release of oxygen free radicals, lipid peroxidation, and intracellular calcium influx - causing further cellular damage, oedema, and necrosis.
- The resulting oedema further raises compartment pressure, completing the cycle.
Elevated CPK and myoglobinuria are late markers of tissue destruction and should not be used to make the diagnosis. - Current Surgical Therapy, 14th Ed.
Anatomical Compartments
The most commonly affected regions are the leg and forearm:
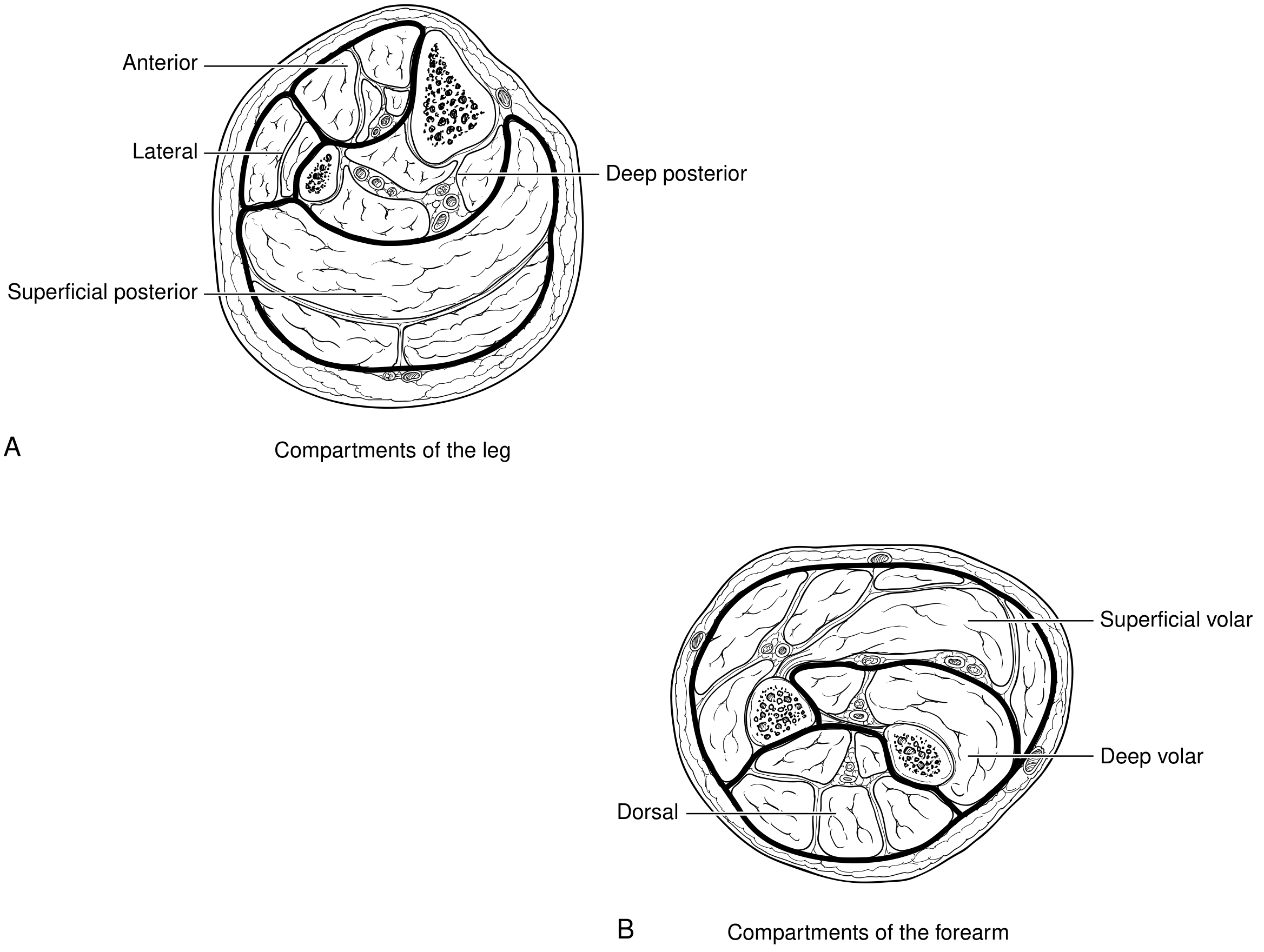
Leg (4 compartments):
- Anterior
- Lateral
- Superficial posterior
- Deep posterior
Forearm (3 compartments):
- Superficial volar
- Deep volar
- Dorsal
(Current Surgical Therapy, 14th Ed.)
Clinical Features
Compartment syndrome is primarily a clinical diagnosis. The classic presentation follows a pattern often remembered as the "6 Ps", though the first three are the most diagnostically useful:
| Sign/Symptom | Significance |
|---|---|
| Pain out of proportion to the injury | Early, cardinal feature |
| Pain increasing despite treatment | Early, cardinal feature |
| Pain on passive stretch of muscles in the compartment | Early, most reliable |
| Paraesthesia | Early nerve ischaemia |
| Paralysis | Late sign - significant ischaemia already present |
| Pallor | Late sign |
| Pulselessness | Extremely late sign - do not wait for this |
The absence of a pulse does NOT rule out compartment syndrome, and waiting for pulselessness means irretrievable limb damage has already occurred.
(Bailey and Love's; Rosen's Emergency Medicine)
Compartment Pressure Monitoring
Pressure measurement is indicated when:
- Clinical diagnosis is uncertain
- Patient has altered level of consciousness (intubated, head injury, sedation)
- Patient is uncooperative or neurologically impaired
Thresholds for fasciotomy:
| Criterion | Threshold |
|---|---|
| Absolute compartment pressure | ≥ 30 mmHg |
| Delta pressure (diastolic BP - compartment pressure) | ≤ 30 mmHg (Bailey & Love) / < 10 mmHg (Current Surgical Therapy) |
Measure multiple sites, near but not directly at the fracture. All compartments of the affected limb should be checked.
Fasciotomy should also be performed if clinical suspicion is high, even with normal pressures.
Special Scenarios
Reperfusion compartment syndrome: After arterial repair or thromboembolectomy, the risk rises sharply when ischaemia time was >6 hours. In such cases, prophylactic fasciotomy is recommended rather than waiting for clinical signs. Upper extremity ischaemia is often less severe due to collateral circulation, but forearm and hand fasciotomies may still be needed. - Current Surgical Therapy, 14th Ed.
Open fractures: Compartment syndrome can still occur - do not be falsely reassured by a wound. (Bailey and Love's)
High- and low-energy injuries: The incidence is nearly equal - do not dismiss low-energy mechanisms. (Bailey and Love's)
Management
Immediate / Emergency Measures
- Split and bivalve all circumferential casts and dressings down to skin.
- Elevate the extremity.
- Remove any constricting bandages.
- Seek immediate senior (surgical) input.
Definitive Treatment: Fasciotomy
Surgical fasciotomy is the only definitive treatment. It must be performed urgently once the diagnosis is made (or strongly suspected).
- Lower leg: Four-compartment fasciotomy via medial and lateral incisions.
- Forearm: Volar and dorsal fasciotomy incisions; if swelling extends to the hand, carpal tunnel release and hand fasciotomies may also be needed (hand surgery consultation recommended).
- All fasciotomy wounds are left open.
- A vacuum-assisted closure (VAC) device is applied postoperatively to reduce oedema.
- Do not attempt early wound closure - this risks muscle necrosis.
Postoperative Care
- Haemodynamic monitoring and serial neurovascular examinations.
- Watch for rhabdomyolysis: ischaemic muscle releases myoglobin, which can cause acute tubular necrosis and renal failure.
- Aggressive IV fluid resuscitation, titrating to urine output > 100 mL/hour until CPK < 5,000 U/L.
- Urine alkalinization with bicarbonate in patients with significant tissue damage and rising CPK.
- Correct acidosis and electrolyte imbalances (particularly hyperkalaemia from intracellular potassium release).
(Current Surgical Therapy, 14th Ed.)
Pitfalls and High-Risk Situations
- Do not wait for the 6 Ps to be complete - act on pain out of proportion alone.
- Maintain a high index of suspicion in all patients with altered consciousness.
- Compartment syndrome occurs in open fractures (a wound does not "decompress" a compartment).
- High-energy and low-energy injuries carry nearly equal incidence.
- Delay in diagnosis leads to limb loss, rhabdomyolysis, renal failure, and death.
Sources: Bailey and Love's Short Practice of Surgery, 28th Ed. | Rosen's Emergency Medicine, 10th Ed. | Current Surgical Therapy, 14th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.