Abg analysis basics to clinical
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
I now have sufficient comprehensive data. Let me compile the full, authoritative ABG analysis guide.
ABG Analysis: Basics to Clinical
1. What Is an ABG?
An arterial blood gas (ABG) is a blood sample drawn from an artery (usually radial) that reports the partial pressures of oxygen and CO2, serum pH, bicarbonate, and oxygen saturation in arterial blood - after it has left the pulmonary circulation and before peripheral tissue gas exchange. It is the reference standard for evaluating oxygenation, ventilation, and acid-base status.
"Blood gas analysis also typically includes direct measurement of lactic acid as lactate, total hemoglobin, and serum electrolytes." - Tintinalli's Emergency Medicine
2. Normal ABG Values
| Parameter | Normal Range |
|---|---|
| pH | 7.35 - 7.45 |
| PaCO2 | 35 - 45 mm Hg |
| HCO3- | 22 - 26 mEq/L |
| PaO2 | 80 - 100 mm Hg |
| SaO2 | 95 - 100% |
| BE (Base Excess) | -2 to +2 mEq/L |
- Acidemia = pH < 7.35
- Alkalemia = pH > 7.45
Note: Acidemia/alkalemia describe the pH of the blood; acidosis/alkalosis describe discrete pathological processes. Multiple disorders can coexist - pH reflects their balance. - Rosen's Emergency Medicine
3. Core Physiology: Henderson-Hasselbalch
The key equation:
pH = pKa + log ( [HCO3-] / [0.03 × PaCO2] )
Simplified (Kassirer-Bleich approximation):
[H+] = 24 × PaCO2 / [HCO3-]
- At pH 7.4 → [H+] ≈ 40 nmol/L
- At pH 7.2 → [H+] ≈ 63 nmol/L
- At pH 7.6 → [H+] ≈ 25 nmol/L
Lungs regulate PaCO2 (respiratory axis). Kidneys regulate HCO3- (metabolic axis). Both work together to keep pH in the narrow 7.35-7.45 range. - Murray & Nadel's Respiratory Medicine
4. The Four Primary Acid-Base Disorders
| Disorder | pH | Primary Change | Compensatory Response |
|---|---|---|---|
| Metabolic Acidosis | ↓ | ↓ HCO3- | ↑ Ventilation → ↓ PaCO2 |
| Metabolic Alkalosis | ↑ | ↑ HCO3- | ↓ Ventilation → ↑ PaCO2 |
| Respiratory Acidosis | ↓ | ↑ PaCO2 | Renal ↑ HCO3- reabsorption, ↑ H+ excretion |
| Respiratory Alkalosis | ↑ | ↓ PaCO2 | Renal ↓ HCO3- reabsorption, ↓ H+ excretion |
5. Compensation Formulas (MUST MEMORIZE)
These predict expected compensation for simple disorders. If actual values differ significantly, a mixed disorder is present.
| Primary Disorder | Expected Compensation |
|---|---|
| Metabolic Acidosis | ↓ PaCO2 = 1.3 × ↓ HCO3- (Winter's formula) |
| Metabolic Alkalosis | ↑ PaCO2 = 0.6 × ↑ HCO3- |
| Respiratory Acidosis - Acute | For every ↑ PaCO2 of 10 mm Hg → HCO3- ↑ by 1 mEq/L |
| Respiratory Acidosis - Chronic | For every ↑ PaCO2 of 10 mm Hg → HCO3- ↑ by 4 mEq/L |
| Respiratory Alkalosis - Acute | For every ↓ PaCO2 of 10 mm Hg → HCO3- ↓ by 2 mEq/L |
| Respiratory Alkalosis - Chronic | For every ↓ PaCO2 of 10 mm Hg → HCO3- ↓ by 5 mEq/L |
Respiratory compensation for metabolic disorders is rapid (minutes to hours). Metabolic compensation for respiratory disorders takes 3-5 days (requires renal adjustment). - Roberts & Hedges' Clinical Procedures in Emergency Medicine
6. Step-by-Step ABG Interpretation
Step 1: Determine pH Status
- pH < 7.35 → Acidemia
- pH > 7.45 → Alkalemia
- pH 7.35-7.45 → Normal (but a disorder may still be present with compensation or mixed states)
Step 2: Identify the Primary Process
- Look at PaCO2 and HCO3-:
- Respiratory: PaCO2 moves opposite to pH (↑ PaCO2 + ↓ pH = respiratory acidosis)
- Metabolic: PaCO2 and pH move in the same direction (↓ PaCO2 + ↓ pH = metabolic acidosis)
Step 3: Check Compensation
- Use the formulas above. If observed compensation ≠ predicted → suspect a mixed disorder
Step 4: Calculate the Anion Gap (in metabolic acidosis)
Anion Gap (AG) = Na+ - (Cl- + HCO3-)
- Normal AG: 8-12 mEq/L (some use <15)
- High AG → unmeasured anions accumulating
- Normal AG → hyperchloremic acidosis
Step 5: Delta-Delta Ratio (if high AG acidosis present)
(AG - 12) / (24 - HCO3-)
- < 1 → concurrent non-AG metabolic acidosis
- 1-2 → pure AG acidosis
-
2 → concurrent metabolic alkalosis
Step 6: Assess Oxygenation
- PaO2, SaO2, and A-a gradient
7. Acid-Base Map
This map plots pH vs. PaCO2 and visually identifies where a patient's values fall among simple and mixed disorders:
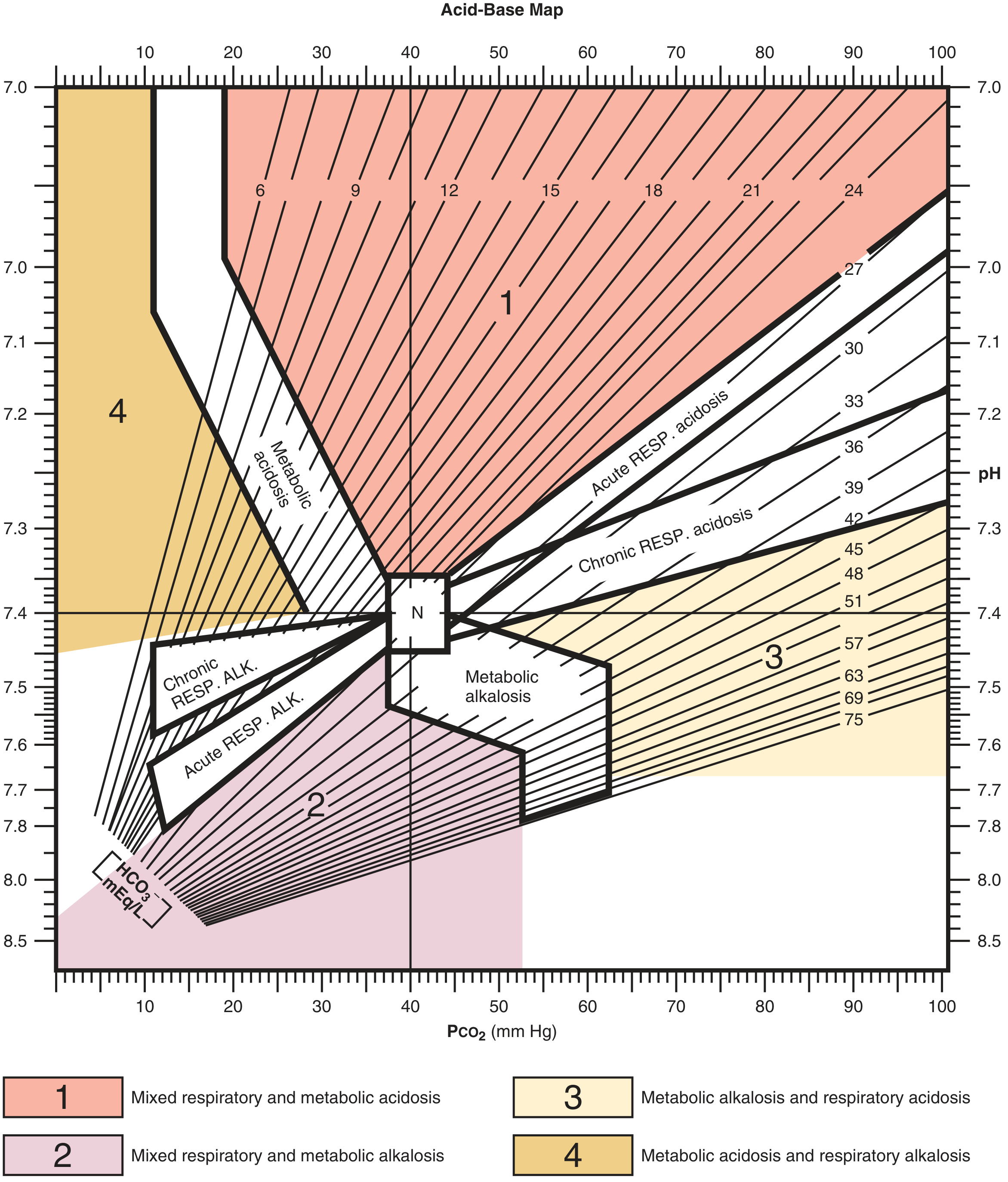
Zone 1 = Mixed respiratory + metabolic acidosis | Zone 2 = Mixed respiratory + metabolic alkalosis | Zone 3 = Metabolic alkalosis + respiratory acidosis | Zone 4 = Metabolic acidosis + respiratory alkalosis
8. Metabolic Acidosis in Detail
High Anion Gap - Mnemonic: MUDPILES
| Letter | Cause |
|---|---|
| M | Methanol |
| U | Uremia (CKD) |
| D | DKA / Alcoholic ketoacidosis |
| P | Paraldehyde, Polyethylene glycol, Paracetamol (acetaminophen) |
| I | Iron |
| L | Lactic acidosis (most common - ~50% of cases) |
| E | Ethylene glycol |
| S | Salicylates |
Lactic acidosis is the single most common cause of high-AG metabolic acidosis. A normal AG does not rule out lactic acidosis or ketoacidosis - measure these directly when clinical concern is high. - Rosen's Emergency Medicine
Normal Anion Gap (Hyperchloremic) - Mnemonic: HARDUP
| Letter | Cause |
|---|---|
| H | Hyperalimentation, Hospital saline infusion |
| A | Acid infusion, Addison's disease, Acetazolamide (carbonic anhydrase inhibitor) |
| R | Renal Tubular Acidosis (RTA) |
| D | Diarrhea (GI loss of HCO3-) |
| U | Ureterosigmoidostomy |
| P | Pancreatic drainage/fistula |
Osmolar Gap (useful in high-AG + toxic alcohol suspicion)
Osmolar Gap = Measured Osm - [2(Na) + Glucose/18 + BUN/2.8 + EtOH/3.7]
- Normal ≤ 10 mOsm/kg
- Elevated → suspect toxic alcohol (methanol, ethylene glycol)
- To estimate methanol: Osmolar gap × 3 = mg/dL
- To estimate ethylene glycol: Osmolar gap × 6 = mg/dL
Clinical Manifestations
- Tachypnea (Kussmaul breathing in severe cases)
- Fatigue, confusion, coma in severe acidemia
- Cardiac arrhythmias, decreased contractility
- Insulin resistance, hyperkalemia
Treatment
- Treat the underlying cause
- NaHCO3 considered to raise pH > 7.10 in severe metabolic acidosis, or > 7.20 when combined with acute kidney injury - Rosen's Emergency Medicine
9. Metabolic Alkalosis in Detail
Causes
Chloride-responsive (urine Cl- < 20 mEq/L):
- Vomiting, nasogastric suction (HCl loss)
- Diuretics (loop, thiazide)
- Post-hypercapnia
- Diarrhea with high Cl- loss
Chloride-resistant (urine Cl- > 20 mEq/L):
- Primary hyperaldosteronism, Cushing's syndrome
- Severe hypokalemia
- Exogenous mineralocorticoids
- Liddle syndrome
Mechanism: Volume depletion activates the renin-angiotensin-aldosterone system → kidneys reabsorb Na+, HCO3-, and excrete H+ and K+ → worsens alkalosis. - Rosen's Emergency Medicine
Treatment
- Chloride-responsive: IV normal saline + KCl replacement
- Chloride-resistant: Treat underlying cause (surgical for primary aldosteronism, stop offending agent)
10. Respiratory Acidosis in Detail
Definition: ↑ PaCO2 (> 45 mm Hg) → ↓ pH
Causes (hypoventilation or impaired CO2 excretion)
- CNS depression: Opioids, sedatives, brainstem lesion, obesity hypoventilation
- Neuromuscular: Guillain-Barré, myasthenia gravis, ALS, high cervical cord injury
- Chest wall: Kyphoscoliosis, flail chest, massive obesity
- Airway obstruction: Severe COPD, asthma, foreign body, tracheal stenosis
- Severe parenchymal disease: ARDS, severe pneumonia
Acute vs. Chronic
- Acute: HCO3- rises ~1 mEq/L per 10 mm Hg rise in PaCO2 (limited buffering)
- Chronic: HCO3- rises ~4 mEq/L per 10 mm Hg rise in PaCO2 (full renal compensation over 3-5 days)
Clinical Manifestations
- CO2 narcosis: headache, confusion, asterixis, somnolence, coma
- Vasodilation, warm flushed skin, bounding pulse
- Papilledema (from cerebral vasodilation)
Treatment
- Correct underlying cause
- Mechanical ventilation if severe or acute decompensation
- Avoid rapid correction in chronic respiratory acidosis (risks post-hypercapnic metabolic alkalosis)
11. Respiratory Alkalosis in Detail
Definition: ↓ PaCO2 (< 35 mm Hg) → ↑ pH
Causes (hyperventilation)
- Hypoxemia: Any cause (altitude, pneumonia, PE, pulmonary edema) - stimulates carotid bodies
- CNS stimulation: Anxiety/panic attacks, pain, fever, TBI, meningitis, stroke
- Drugs: Salicylates (early), progesterone, catecholamines
- Mechanical ventilation: Over-ventilation
- Liver failure: Ammonia-driven hyperventilation
- Pregnancy: Progesterone-driven mild respiratory alkalosis
Clinical Manifestations
- Paresthesias (perioral, fingertips)
- Carpopedal spasm, tetany (↓ ionized Ca2+)
- Lightheadedness, syncope
Treatment
- Treat the underlying cause
- Rebreathing into bag (anxiety only - with caution)
- Correct hypoxemia if present
12. Oxygenation Assessment
Key Parameters
| Parameter | Formula/Normal | Clinical Use |
|---|---|---|
| PaO2 | 80-100 mm Hg | Direct measurement of dissolved O2 |
| SaO2 | 95-100% | Hemoglobin saturation |
| A-a Gradient | (see formula) | Distinguishes lung vs. non-lung hypoxemia |
| P/F Ratio | PaO2/FiO2 (normal >400) | Severity of lung injury/ARDS |
Alveolar-Arterial (A-a) Oxygen Gradient
PAO2 = (FiO2 × [Patm - PH2O]) - (PaCO2/RQ)
At room air: PAO2 ≈ 150 - (PaCO2/0.8)
A-a gradient = PAO2 - PaO2
- Normal (young adults): < 10-15 mm Hg (increases with age: ~(age/4) + 4)
- Elevated A-a gradient → pathology within the lung (V/Q mismatch, shunt, diffusion defect)
- Normal A-a gradient with low PaO2 → hypoventilation or low FiO2
P/F Ratio and ARDS Berlin Criteria
| Category | P/F Ratio |
|---|---|
| Mild ARDS | 200-300 |
| Moderate ARDS | 100-200 |
| Severe ARDS | < 100 |
Causes of Hypoxemia (and A-a gradient status)
| Mechanism | A-a Gradient | Example |
|---|---|---|
| Hypoventilation | Normal | Opioid overdose, NMJ disease |
| V/Q Mismatch | Elevated | COPD, PE, atelectasis |
| Shunt | Elevated (doesn't correct with O2) | ARDS, hepatopulmonary syndrome, intracardiac shunt |
| Diffusion impairment | Elevated | ILD, pulmonary fibrosis |
| Low FiO2 | Normal | High altitude |
13. Venous Blood Gas (VBG) vs. ABG
| Parameter | VBG vs. ABG |
|---|---|
| pH | VBG ≈ ABG - 0.03-0.05 (clinically close) |
| PaCO2 | VBG higher by up to 6 mm Hg (use for trending; not reliable for hypercarbia evaluation) |
| PaO2 | VBG does NOT correlate with arterial O2 - cannot be used for oxygenation |
| Lactate | Normal/markedly elevated venous values correlate; mildly elevated may not |
"Venous PCO2 values do not correlate with arterial oxygen content and cannot be used for evaluation of oxygenation." - Tintinalli's Emergency Medicine
14. Clinical Case Examples
Case 1: Diarrhea (Compensated Metabolic Acidosis)
- Na+ 133, K+ 2.8, Cl- 118, pH 7.26, PaCO2 13, HCO3- 5
- Step 1: Acidemia (pH < 7.35)
- Step 2: Metabolic (↓ HCO3- + ↓ PaCO2 = same direction as pH)
- Compensation check (Winter's): ΔPaCO2 = 1.3 × (25-5) = 26 → Expected PaCO2 = 40-26 = 14 mm Hg. Actual = 13 ✓ Pure metabolic acidosis with appropriate respiratory compensation
- AG = 133-(118+5) = 10 → Normal AG → Hyperchloremic (from diarrhea)
Case 2: Sepsis (Respiratory Alkalosis)
- Na+ 138, K+ 3.2, Cl- 105, pH 7.49, PaCO2 25, HCO3- 22
- Step 1: Alkalemia (pH > 7.45)
- Step 2: Respiratory (↓ PaCO2 + ↑ pH = opposite direction)
- Compensation: Acute respiratory alkalosis → HCO3- should ↓ by 2 per 10 mm Hg drop in PaCO2 → ↓ PaCO2 = 15 → expected ↓ HCO3- = 3 → expected HCO3- ≈ 22 ✓ Pure respiratory alkalosis
- Clinical: Sepsis driving hyperventilation
15. Mixed Acid-Base Disorders
Suspect when:
- Compensation values do not match formulas
- pH is normal but both PaCO2 and HCO3- are markedly abnormal
- Clinical scenario suggests multiple processes
Common mixed disorders:
- DKA + vomiting: High-AG metabolic acidosis + metabolic alkalosis
- COPD + diuretics: Respiratory acidosis + metabolic alkalosis
- Sepsis + renal failure: Respiratory alkalosis + high-AG metabolic acidosis
- Cardiac arrest: Respiratory acidosis + lactic acidosis (mixed acidosis)
Use the Acid-Base Map above to visually identify where values fall outside expected single-disorder zones.
Sources
- Roberts & Hedges' Clinical Procedures in Emergency Medicine, 15th edition
- Rosen's Emergency Medicine: Concepts and Clinical Practice, 9th edition
- Murray & Nadel's Textbook of Respiratory Medicine, 7th edition
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9th edition
This is a shared conversation. Sign in to Orris to start your own chat.