pagets disease 15 marks ortho
Reading File
Finding Sources
Searching PubMed
"Paget disease" bone management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed for a thorough 15-mark answer. Here is the complete structured response:
Paget's Disease of Bone (Osteitis Deformans) - 15 Marks
Definition
Paget's disease of bone (PDB) is a chronic, focal metabolic bone disorder characterized by accelerated but disorganized bone remodeling - excessive osteoclastic resorption followed by a compensatory osteoblastic response - resulting in structurally abnormal, enlarged, and mechanically weak bone.
- Harrison's Principles of Internal Medicine 22E p. 3355
- Rockwood & Green's Fractures in Adults 10th ed. p. 123
Epidemiology
- Age of onset: rarely before 50; prevalence increases with age (~3% autopsy prevalence in those >40 years)
- More common in males (M:F ratio 1.4:1)
- High prevalence in UK, France, Spain, Italy, and European migrant populations (Australia, USA, New Zealand)
- Rare in Scandinavia, Africa, Far East, Indian subcontinent
- Prevalence and severity have been declining over recent decades
- Monostotic: ~15% of cases; Polyostotic: ~85% of cases
- Axial skeleton or proximal femur involved in up to 80% of cases
Etiology and Pathogenesis
Genetic Factors
The most important gene is SQSTM1 (sequestosome-1), mutated in ~50% of familial and ~10% of sporadic cases. SQSTM1 mutations lead to increased NF-kB activity, which drives osteoclast overactivity.
| Gene/Locus | Association |
|---|---|
| SQSTM1 (5q35) | Classic PDB - activates NF-kB |
| TNFRSF11A (RANK) | Juvenile PDB - activating mutation |
| TNFRSF11B (OPG) | Juvenile PDB - inactivating mutation |
| VCP | Inclusion body myopathy + PDB + frontotemporal dementia |
| DCSTAMP | Promotes osteoclast precursor fusion |
- First-degree relatives have ~7-fold increased risk
- Positive family history found in 15-25% of patients
Environmental Factors
- Paramyxovirus (measles virus) infection of osteoclast precursors was historically proposed; now questioned by large-scale serological studies
- Low dietary calcium/vitamin D in childhood, mechanical loading, and toxin exposure have also been proposed
Pathophysiology - The 3 Phases
- Osteolytic (hot) phase: Numerous large osteoclasts (up to 100 nuclei per cell) with active resorption pits. The hallmark is a "blade of grass" or "flame-shaped" lytic front on radiograph.
- Mixed phase: Concurrent osteoblastic and osteoclastic activity. Bone formation begins but is disorganized (woven bone laid down randomly, not along stress lines). Marrow fibrosis and hypervascularization occur.
- Osteosclerotic (burned-out/quiescent) phase: Predominantly osteoblastic activity. Bone is thickened but structurally weak due to the mosaic pattern of lamellar bone joined by irregular cement lines (jigsaw puzzle appearance).
Histopathology
The hallmark is a mosaic pattern of lamellar bone - haphazardly oriented units of lamellar bone joined by prominent, irregular cement lines, producing a "jigsaw puzzle" appearance.
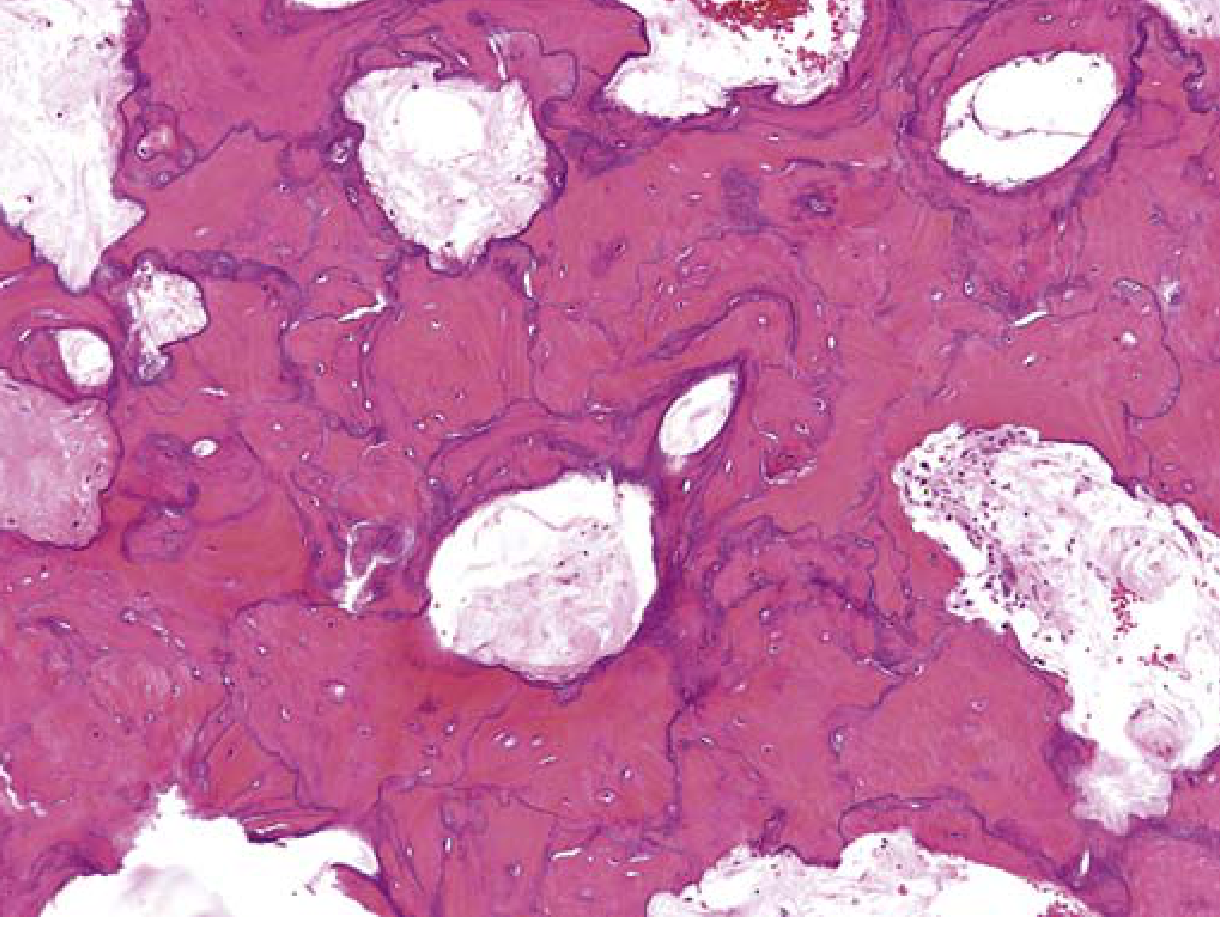
Robbins & Kumar Basic Pathology - FIG. 19.10: Mosaic pattern of lamellar bone pathognomonic of Paget disease
Clinical Features
Most patients (majority) are asymptomatic - discovered incidentally on radiograph or as elevated serum alkaline phosphatase (ALP).
Symptoms (when present)
| System | Manifestation |
|---|---|
| Bone | Deep, aching bone pain (most common symptom); worse at rest and at night |
| Skull | Enlarging hat size, frontal bossing, leontiasis ossea (lion face), platybasia (skull base invagination), deafness (CN VIII compression or cochlear involvement) |
| Spine | Kyphosis, spinal cord compression, nerve root compression (radiculopathy) |
| Long bones | Anterior bowing of femur and tibia ("sabre tibia"), chalk-stick (banana) fractures |
| Joints | Secondary osteoarthritis (femoral head distortion, acetabular involvement) |
| Vascular | Increased bone vascularity -> high-output cardiac failure (rare, only in extensive polyostotic disease) |
| Malignant transformation | Osteosarcoma (most serious complication): <1% of cases but should be suspected with sudden worsening of pain or soft tissue mass |
Classic Physical Findings
- Enlarged skull with prominent veins
- Anterior bowing of tibia (sabre tibia)
- Waddling gait
- Angioid streaks on fundoscopy
Investigations
Biochemical Markers (most important)
| Test | Finding |
|---|---|
| Serum Alkaline Phosphatase (ALP) | Most sensitive marker - markedly elevated; reflects osteoblastic activity |
| Serum calcium | Normal (distinguishes from hyperparathyroidism) |
| Serum phosphate | Normal |
| Urinary hydroxyproline / NTx / CTx | Elevated (reflect osteoclastic bone resorption) |
| Serum bone-specific ALP | More specific than total ALP |
Note: Immobilization may rarely cause hypercalcemia in active PDB. Discovery of hypercalcemia should prompt search for another cause (e.g., primary hyperparathyroidism, malignancy).
Imaging
Plain X-ray - key diagnostic tool:
- Lytic phase: "Blade of grass" or "flame-shaped" advancing lytic front
- Mixed/sclerotic phase: Bone expansion with thickened, coarsened trabeculae; cortical thickening; "cotton wool" appearance in skull; "picture frame" vertebra
- Long bones: Anterior bowing (tibia, femur); chalk-stick fractures (transverse, cortical)
- Skull: "Osteoporosis circumscripta" (lytic phase), then "cotton wool" skull
Radionuclide Bone Scan (Tc-99m):
- Most sensitive for detecting extent and activity of disease
- Shows "hot spots" in affected bones
- Best for mapping distribution before treatment
CT scan: Best for assessing structural detail, especially vertebral involvement and neural compression
MRI: Used when cord or nerve root compression is suspected
Differential Diagnosis
- Osteoblastic metastases (prostate, breast)
- Fibrous dysplasia
- Primary hyperparathyroidism (brown tumors)
- Osteomalacia
- Osteosarcoma (in rapidly progressing lesion)
Treatment
Indications for Treatment
- Symptomatic disease (bone pain, fracture, headache, radiculopathy)
- High disease activity (markedly elevated ALP) with involvement of weight-bearing bones, joints, vertebral bodies, skull
- Pre-operative (to reduce vascularity and blood loss)
- Hypercalciuria during immobilization
- Neurological complications
Pharmacological Treatment
Bisphosphonates are the first-line treatment:
| Drug | Dose | ALP Normalization |
|---|---|---|
| Zoledronic acid (most effective) | 5 mg IV over 15 min (single infusion) | ~90% at 6 months |
| Risedronate | 30 mg/day PO x 2 months | 73% |
| Alendronate | 40 mg/day PO x 6 months | 63% |
| Pamidronate | 30 mg/day IV x 3 days | ~50% |
| Etidronate | 200-400 mg/day PO x 6 months | 15% (weakest) |
| Calcitonin | 100 U SC daily x 6-18 months | ALP reduction ~50% |
Zoledronic acid is now the treatment of choice for most patients - a single IV infusion produces sustained remission.
Important: Adequate calcium and vitamin D supplementation must be given before and during bisphosphonate therapy. Bisphosphonates rapidly suppress bone resorption while active formation continues, risking hypocalcemia especially in vitamin D-deficient patients.
Calcitonin is now rarely used (reserved for those who cannot tolerate bisphosphonates).
Surgical Treatment
Indications:
- Correction of long bone deformity (osteotomy for sabre tibia)
- Pathological fracture fixation (intramedullary nailing preferred; pre-treat medically to reduce vascularity and blood loss)
- Joint replacement for severe secondary osteoarthritis
- Spinal decompression for cord/nerve root compression
- Biopsy/resection if osteosarcoma is suspected
Pre-operative bisphosphonate therapy (zoledronic acid) is given 4-6 weeks before elective surgery at pagetic sites to reduce blood loss.
Monitoring Treatment Response
- Serum ALP is the primary monitoring marker
- Measured every 3-6 months initially
- Bone scan for distribution mapping and follow-up
- Aim: normalization of ALP
Complications (Summary)
| Complication | Notes |
|---|---|
| Pathological fracture | Chalk-stick (banana) fractures; transverse cortex of long bones |
| Secondary osteoarthritis | Hip most commonly affected |
| Deafness | Both sensorineural and conductive |
| High-output cardiac failure | Only in severe polyostotic disease with extensive AV shunting |
| Osteosarcoma | <1%, but most feared; usually osteoblastic; very poor prognosis |
| Spinal stenosis/cord compression | Vertebral involvement |
| Cranial nerve palsies | Skull base foraminal narrowing |
Key Exam Points (15-mark Answer)
- Definition: Focal metabolic bone disorder with disorganized remodeling
- Pathology: 3 phases - lytic, mixed, sclerotic; mosaic (jigsaw) pattern on histology
- Genetics: SQSTM1 mutation most common; RANK/OPG in juvenile PDB
- Most common site: Pelvis > lumbar spine > femur > skull > tibia
- Key lab: Elevated ALP with normal serum calcium - distinguishes from hyperparathyroidism
- Best imaging for extent: Bone scan (Tc-99m); best for diagnosis: X-ray
- Best treatment: Zoledronic acid 5 mg IV single infusion (90% ALP normalization)
- Most feared complication: Osteosarcoma
- Surgical pearl: Pre-treat with bisphosphonate before operating on pagetic bone to minimize bleeding
- Chalk-stick fracture: Transverse fracture through sclerotic cortex of long bones; starts on convex side
Sources: Harrison's Principles of Internal Medicine 22E | Rockwood & Green's Fractures in Adults 10th ed. | Robbins & Kumar Basic Pathology | Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.