Approach to patient with Pyelonephritis and Diabetes
Reading File
Finding Sources
Finding Sources
Searching PubMed
pyelonephritis diabetes management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information to synthesize a thorough answer. Let me compile everything.
Approach to Pyelonephritis in a Diabetic Patient
Pyelonephritis in a diabetic patient is always classified as a complicated UTI - diabetes mellitus itself is a recognized risk factor for more severe disease, atypical presentations, and life-threatening complications. The approach must be more aggressive than in the general population.
Why Diabetes Worsens Pyelonephritis
Several mechanisms make diabetic patients uniquely vulnerable (per Smith & Tanagho's General Urology):
| Mechanism | Effect |
|---|---|
| Glycosuria | Provides substrate for bacterial fermentation; promotes bacterial growth |
| Neutrophil dysfunction | Elevated glucose impairs phagocytosis and bacterial clearance |
| Autonomic neuropathy | Causes dysfunctional voiding and urinary retention, preventing bacterial clearance |
| Defective local cytokine response | Reduced innate immunity in the urinary tract |
| Increased bacterial adherence | Uropathogens adhere more readily to uroepithelium |
There is a 2- to 5-fold increase in acute pyelonephritis in diabetic patients vs. non-diabetics, and the risk correlates directly with HbA1c levels. - Smith and Tanagho's General Urology, 19e
Step 1: Clinical Assessment
Symptoms to Elicit
- Fever, rigors, chills
- Flank pain / costovertebral angle (CVA) tenderness
- Nausea, vomiting, prostration
- Lower urinary symptoms: dysuria, frequency, urgency (may or may not be present)
- Symptom onset and duration
Important: In diabetic patients, the presentation may be subtle or atypical due to neuropathy - fever, pain, and inflammatory response may be blunted or absent. - Tintinalli's Emergency Medicine
Red Flags Suggesting Complicated/Severe Disease
- High fever (>39°C) with rigors
- Inability to tolerate oral intake (vomiting)
- Persistent symptoms despite >48-72h of outpatient antibiotics
- Signs of sepsis (tachycardia, hypotension, altered mental status)
- Known urinary obstruction or stone disease
- Prior resistant organisms
- Pneumaturia (gas in urine - suggests emphysematous pyelonephritis)
Step 2: Physical Examination
- Vital signs: temperature, BP, heart rate, respiratory rate (sepsis screen)
- CVA tenderness (percussion over kidney angle)
- Suprapubic tenderness
- Abdominal exam for mass/rigidity (perinephric abscess)
- Look for signs of septic shock
Step 3: Investigations
Mandatory
| Test | Rationale |
|---|---|
| Urine dipstick / microscopy | Nitrites, leukocyte esterase, WBC casts (casts = upper tract disease) |
| Urine culture & sensitivity | Always obtain in diabetic patients - guides antibiotic therapy |
| Blood cultures x 2 | Bacteremia is common in severe pyelonephritis |
| CBC | Leukocytosis |
| BMP/LFTs | Creatinine, electrolytes (renal function baseline) |
| Blood glucose & HbA1c | Glycemic control assessment |
| Serum procalcitonin / CRP | Severity markers |
Imaging
Ultrasound (KUB or renal): First-line to exclude obstruction, hydronephrosis, or abscess.
CT abdomen/pelvis (with contrast): Preferred in diabetic patients with:
- Failure to respond to antibiotics within 48-72h
- Suspected emphysematous pyelonephritis
- Suspected perinephric or intrarenal abscess
- Suspected papillary necrosis
CT is the gold standard for defining the extent of disease and guiding management in complicated cases. - Campbell-Walsh-Wein Urology
Step 4: Classification of UTI Severity
Diabetes automatically makes this a complicated UTI. Further classify:
1. Uncomplicated pyelonephritis (mild-moderate)
- Fever + CVA tenderness, tolerating oral intake
- No signs of sepsis
- Can be managed as outpatient (rarely applicable in diabetics)
2. Complicated pyelonephritis (severe)
- Systemic toxicity, sepsis
- Inability to tolerate oral antibiotics
- Requires hospitalization
3. Life-threatening complications (see below) - require urgent intervention
Step 5: Antibiotic Management
Key Rule for Diabetics:
Oral outpatient therapy is NOT recommended for a diabetic patient with a complicated UTI. - Smith & Tanagho's General Urology, 19e
Empirical IV Therapy (Hospitalized)
- First choice: IV beta-lactam (ceftriaxone, cefepime) - select based on local antibiogram
- Alternatives: Piperacillin-tazobactam, carbapenems (for suspected ESBL or resistant organisms)
- Fluoroquinolones (ciprofloxacin, levofloxacin): historically first-line but quinolone resistance is now prevalent; still useful once culture sensitivities confirmed
Important Drug Interaction in Diabetics:
TMP-SMX should be avoided if possible in diabetics on oral hypoglycemics - it can potentiate hypoglycemia. - Smith & Tanagho's General Urology, 19e
Step-Down Oral Therapy (Once Tolerating PO, Fever-Free)
- Ciprofloxacin or levofloxacin (if susceptible): 5-7 days
- TMP-SMX (if susceptible, avoid with sulfonylureas): 7-14 days
- Total duration: typically 14 days for complicated pyelonephritis in diabetics
- Beta-lactam orals: less effective, use with close follow-up
Drugs NOT appropriate for pyelonephritis: Nitrofurantoin, fosfomycin, pivmecillinam (inadequate renal tissue levels). - Harrison's, 22e
Step 6: Glycemic Management
- Monitor blood glucose closely (infection drives hyperglycemia)
- Insulin often required even in type 2 diabetics during acute illness
- Optimize glycemic control to improve immune function
- Consider stopping SGLT2 inhibitors during acute illness (risk of euglycemic DKA and also associated with UTI risk per [2025 meta-analysis PMID 39885375])
Step 7: Diabetic-Specific Complications to Watch For
1. Emphysematous Pyelonephritis (EPN) - Urologic Emergency
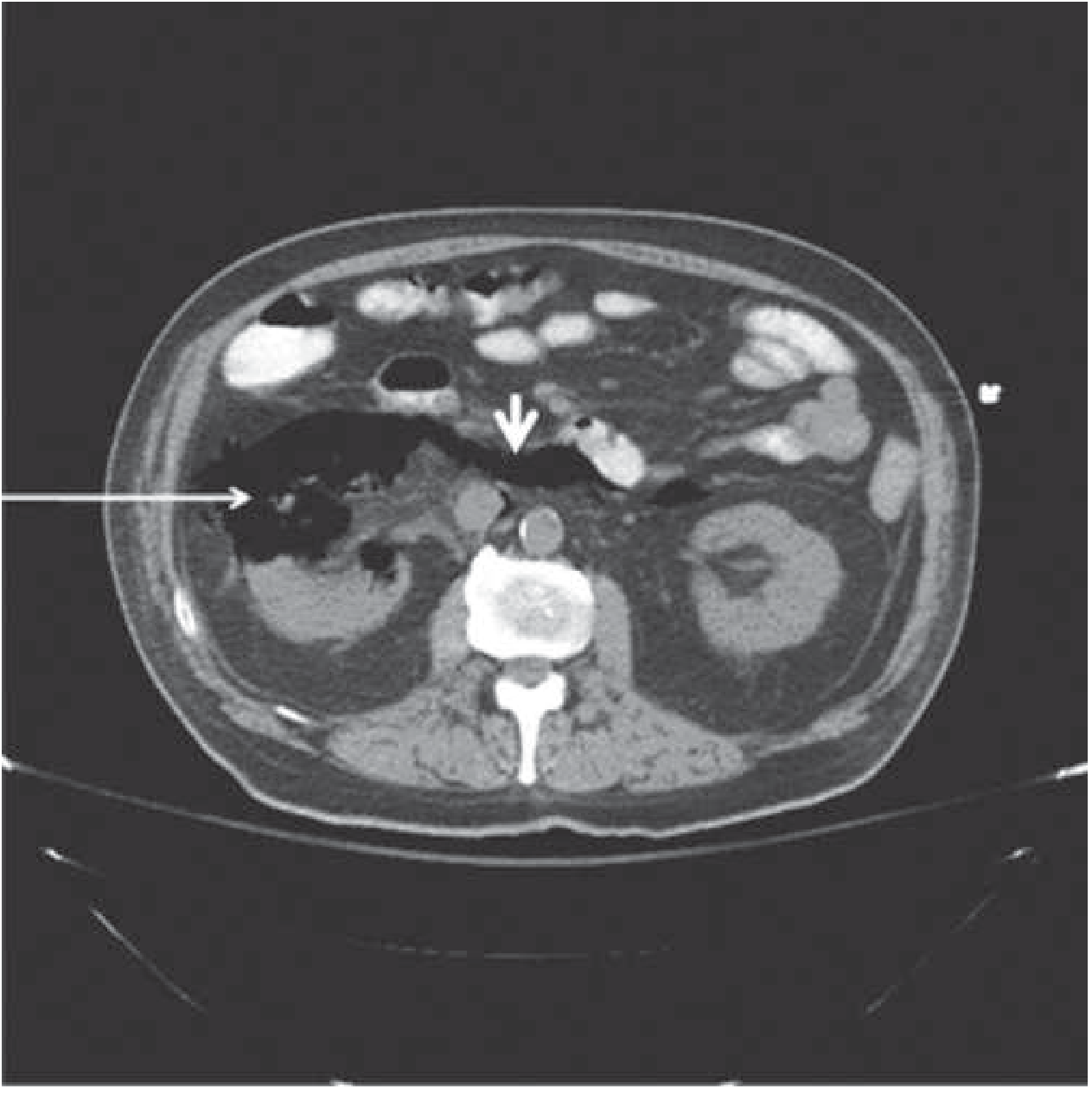
CT of emphysematous pyelonephritis: gas-forming E. coli infection causing destruction of renal parenchyma (arrow) and tracking of gas through the retroperitoneal space (arrowhead). (Harrison's Principles, 22e)
- ~95% occur in diabetics (predominantly women)
- Pathogenesis: high tissue glucose → fermentation by gas-forming organisms (E. coli most common; also Klebsiella, Proteus)
- Classic triad: fever + vomiting + flank pain
- Diagnosis: CT scan (gold standard) showing intraparenchymal or perinephric gas
- Huang-Tseng CT Classification (grades 1-4) guides management
- Mortality: 19-43% overall
- Management:
- IV antibiotics
- Percutaneous drainage (preferred for Classes 1-2)
- Emergency nephrectomy for severe bilateral disease or failure of drainage (Classes 3-4)
- Campbell-Walsh-Wein Urology; Harrison's Principles, 22e
2. Acute Papillary Necrosis
- Much more prevalent in diabetics than non-diabetics
- Sloughed papillae can obstruct the ureter → acute hydronephrosis, acute kidney injury
- Bilateral necrosis → rapid rise in creatinine
- Diagnosis: CT or IVP showing "ring sign," clubbed calyces
- Management: relieve obstruction, IV antibiotics
- Robbins Pathologic Basis of Disease; Harrison's, 22e
3. Perinephric / Renal Abscess
- Suspected when: fever persists >48-72h despite appropriate antibiotics
- CT shows ring-enhancing fluid collection
- Management: CT-guided percutaneous drainage + prolonged IV antibiotics
- In diabetics: consider staphylococcal infection (renal carbuncle) even without obvious source - can arise hematogenously
- Campbell-Walsh-Wein Urology
4. Acute Focal/Multifocal Bacterial Nephritis
- ~50% of patients are diabetic; sepsis is common, >50% bacteremic
- Represents a spectrum between pyelonephritis and frank abscess
- CT: wedge-shaped areas of decreased enhancement without liquefaction
- Treatment: IV antibiotics for ≥7 days + 7 days oral; failure → indicates need for drainage
- Campbell-Walsh-Wein Urology
5. Urosepsis
- 10-19% of all sepsis arises from GU source
- Manage per sepsis bundle: IV fluids, early antibiotics, vasopressors if needed, source control
Step 8: Hospitalization Criteria
Admit if ANY of the following:
- Diabetic patient (most warrant admission for IV therapy)
- Unable to tolerate oral medications
- Signs of sepsis or septic shock
- Suspected complicated disease (abscess, EPN, obstruction)
- Failure of outpatient therapy
- Significant comorbidities or poor adherence
- Harrison's, 22e; Tintinalli's Emergency Medicine
Summary Algorithm
Diabetic patient + Flank pain/Fever/CVA tenderness
↓
Urine culture, blood cultures, CBC, CMP, glucose
Urine microscopy, dipstick
↓
Complicated UTI by default (diabetes = risk factor)
↓
Imaging: Renal USS → CT if no improvement or red flags
↓
Hospitalize → IV beta-lactam empirically
Avoid TMP-SMX (hypoglycemia risk with OHAs)
Optimize blood glucose (insulin if needed)
Stop SGLT2 inhibitors
↓
Reassess 48-72h
┌──────────────────┬───────────────────────┐
Improving Persistent fever/symptoms
Step down oral ↓ CT scan urgently
14 days total Rule out: EPN, abscess,
papillary necrosis,
obstruction
↓ Drainage/Surgery if needed
Recent Evidence Note
A 2025 meta-analysis (PMID 39885375) confirmed that SGLT2 inhibitors are associated with severe UTIs in real-world cohort data - these should be held during acute pyelonephritis episodes. A 2026 systematic review (PMID 41597508) highlighted the importance of CT imaging and biomarkers (CRP, procalcitonin) in identifying complicated forms of acute pyelonephritis.
Key Take-Home Points:
- Diabetes = complicated UTI by definition - never manage as uncomplicated
- No oral outpatient therapy - hospitalize and start IV antibiotics
- Avoid TMP-SMX with oral hypoglycemics; fluoroquinolones effective but check local resistance
- CT scan liberally - emphysematous pyelonephritis and abscess are common in diabetics and must not be missed
- Optimize glycemic control actively - it directly impacts immune response and outcomes
- Monitor for the 4 dangerous complications: EPN, papillary necrosis, perinephric abscess, urosepsis
This is a shared conversation. Sign in to Orris to start your own chat.