Diabetes and it's range and treatment
Reading File
Finding Sources
Finding Sources
Searching PubMed
"diabetes mellitus" AND "treatment guidelines"
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Searching Images
diabetes mellitus types classification blood glucose ranges
I now have comprehensive information to provide a thorough answer. Let me compose the response.
Diabetes Mellitus — Overview, Diagnostic Ranges & Treatment
What Is Diabetes Mellitus?
Diabetes mellitus (DM) is a group of metabolic diseases characterized by chronic hyperglycemia resulting from defects in insulin secretion, insulin action, or both. All forms share elevated blood glucose, but the pathogenic mechanisms differ considerably.
Classification
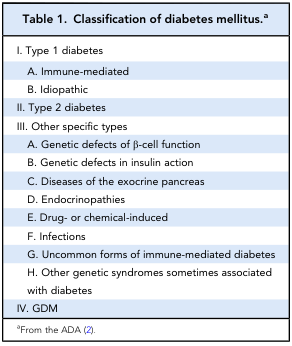
| Type | Mechanism |
|---|---|
| Type 1 | Autoimmune β-cell destruction → absolute insulin deficiency |
| Type 2 | Insulin resistance + progressive β-cell dysfunction |
| Gestational (GDM) | Glucose intolerance first detected in pregnancy |
| Other specific types | MODY (monogenic), pancreatic disease, drug-induced, endocrinopathies |
— Goodman & Gilman's Pharmacological Basis of Therapeutics, Table 51-2
Diagnostic Blood Glucose Ranges (ADA Criteria)
| Category | Fasting Plasma Glucose | 2-hr Post-OGTT | HbA1c |
|---|---|---|---|
| Normal | < 5.6 mmol/L (< 100 mg/dL) | < 7.8 mmol/L | < 5.7% |
| Impaired Fasting Glucose (Prediabetes) | 5.6–6.9 mmol/L (100–125 mg/dL) | — | 5.7–6.4% |
| Impaired Glucose Tolerance (Prediabetes) | — | 7.8–11.0 mmol/L | — |
| Diabetes Mellitus | ≥ 7.0 mmol/L (≥ 126 mg/dL) | ≥ 11.1 mmol/L (≥ 200 mg/dL) | ≥ 6.5% |
| Symptomatic + Random glucose | ≥ 11.1 mmol/L (≥ 200 mg/dL) at any time | — | — |
Note: In the absence of unequivocal hyperglycemia, criteria must be confirmed by repeat testing on a separate day.
— Goodman & Gilman's, Table 51-1; adapted from ADA 2022
HbA1c Treatment Target: Generally ≤ 7% for most non-pregnant adults with diabetes.
Type 1 vs. Type 2 — Key Clinical Differences
| Feature | Type 1 | Type 2 |
|---|---|---|
| Age at onset | Usually < 20 years | Usually > 30 years |
| Body mass | Low/normal | Often overweight/obese |
| Plasma insulin | Low or absent | Normal to high (initially) |
| Insulin sensitivity | Normal | Reduced |
| Primary therapy | Insulin (essential) | Lifestyle + oral agents ± insulin |
— Guyton & Hall Textbook of Medical Physiology, Table 79.3
Treatment
Type 1 Diabetes
- Insulin therapy is mandatory — multiple daily injections (MDI) or continuous subcutaneous insulin infusion (CSII/pump)
- Carbohydrate counting and glucose monitoring are integral
Type 2 Diabetes — Stepwise Approach
Step 1 — Lifestyle Modification (always first)
- Caloric restriction, physical activity, weight loss
- Long-term success is limited; most patients require pharmacotherapy
Step 2 — First-Line Drug: Metformin
- Suppresses hepatic glucose production
- Preferred initial agent; start at diagnosis
- Also useful in polycystic ovary syndrome (PCOS) and prediabetes prevention
Step 3 — Add a Second Agent (if HbA1c target not met in 2–3 months)
| Drug Class | Examples | Mechanism | Notes |
|---|---|---|---|
| Sulfonylureas | Glimepiride, glyburide | Stimulate pancreatic insulin secretion | Risk of hypoglycemia |
| Thiazolidinediones (TZDs) | Pioglitazone | Increase insulin sensitivity (PPARγ agonists) | Weight gain, fluid retention |
| DPP-4 Inhibitors | Sitagliptin | Prolong GLP-1/GIP activity → ↑ insulin secretion | Weight-neutral |
| GLP-1 Receptor Agonists | Semaglutide, liraglutide, dulaglutide | Enhance insulin secretion, reduce appetite, weight loss | ↓ CV events; injectable or oral (semaglutide) |
| SGLT2 Inhibitors (Gliflozins) | Empagliflozin, dapagliflozin | Block renal glucose reabsorption → glucosuria | ↓ CV and renal disease; osmotic diuresis |
| Insulin | Basal, bolus, premixed | Direct glucose lowering | Used when oral agents fail or in advanced T2DM |
Special Considerations:
- Cardiovascular disease or high CV risk: Add a GLP-1 RA (liraglutide, dulaglutide, semaglutide) or SGLT2 inhibitor
- Heart failure or diabetic nephropathy: Prefer SGLT2 inhibitor as second agent
- GIP/GLP-1 dual agonists (e.g., tirzepatide): Greater reductions in weight and blood glucose than GLP-1 agonists alone
Step 4 — Bariatric Surgery
- For severe obesity (BMI > 35) with inadequately controlled T2DM
- Gastric bypass or sleeve gastrectomy → often near-complete diabetes remission
— Goodman & Gilman's, Figure 51-11 treatment algorithm; Guyton & Hall, pp. 975–976
Newer/Advanced Agents
- Semaglutide (oral or injectable): Most potent GLP-1 RA; 13 kg weight reduction vs placebo in obesity trials
- GLP-1/GIP dual agonists: Even greater reductions in adiposity and glucose
- DPP-4 inhibitors: Good tolerability, weight-neutral, no hypoglycemia risk
- SGLT2 inhibitors: Cardioprotective and nephroprotective beyond glucose lowering
Monitoring & Goals
| Parameter | Target |
|---|---|
| HbA1c | ≤ 7% (most adults) |
| Fasting glucose | 4.4–7.2 mmol/L (80–130 mg/dL) |
| Post-meal glucose (2 hr) | < 10 mmol/L (< 180 mg/dL) |
| Blood pressure | < 130/80 mmHg |
| LDL cholesterol | < 2.6 mmol/L (< 100 mg/dL); < 1.8 if high CV risk |
Summary
Diabetes management is individualized. Metformin + lifestyle change remains the foundation for Type 2 DM. GLP-1 receptor agonists and SGLT2 inhibitors have transformed care by providing cardiovascular and renal protection beyond glucose control. Type 1 DM requires lifelong insulin. Regular HbA1c monitoring and complication screening (eyes, kidneys, feet, heart) are essential components of care.
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics; Guyton & Hall Textbook of Medical Physiology; Textbook of Family Medicine 9e
This is a shared conversation. Sign in to Orris to start your own chat.